


Abstract
Background: Changing patterns of referral and management of pediatric surgical conditions, including hypertrophic pyloric stenosis (HPS), have recently been described and often relate to comfort with early nonoperative management, anesthesia and corrective surgery. Travelling distance required for treatment at pediatric centres can also be burdensome for families. We assessed referral patterns for HPS in the maritime provinces of Canada over 10 years to quantify the burden on families travelling for surgical care.
Methods: We reviewed the charts of all patients with HPS in the Maritimes. Length of hospital stay (LOS) and complication rates were analyzed in regards to resuscitation and management at a pediatric centre and/or peripheral centres. We used postal codes for each patient to track distance travelled for management.
Results: We assessed 751 cases of HPS. During the study period (Jan. 1, 2001–Dec. 31, 2010), referral to pediatric centres increased from 49% to 71%. Postoperative complications were 2.5-fold higher in peripheral centres. Infants referred to pediatric centres were 78% less likely to have an LOS longer than 3 days. Laparoscopic pyloromyotomy, which was performed only in pediatric centres, was associated with a shorter postoperative LOS.
Conclusion: Our study supports the current literature demonstrating improved outcomes, shorter overall LOS and decreased risk of complications when infants with HPS are treated in pediatric centres. This should be considered when planning access to pediatric surgical resources.
Changing patterns of referral and management of various surgical conditions have recently been described and often relate to comfort with resuscitation management, infant anesthesia and surgical correction. 1 However, substantial travelling distance to centres offering the appropriate level of care is associated with family stress, increased financial costs and reduction in social supports of the home community. In order to justify this added patient burden, the benefit of primary referral must outweigh the negative aspects.
Hypertrophic pyloric stenosis (HPS) is one of the most common surgical conditions encountered in infants and is unique in its need for adequate preoperative resuscitation in addition to surgical correction. Historically, HPS was a condition managed and corrected in the community by general surgeons as well as surgeons with pediatric subspecialty training. Recent changes in health care deliverables, however, have identified the value of not only pediatric surgical expertise, but also subspecialty expertise in anesthesiology and perioperative care.2,3 Subsequent reduction in exposure of surgical trainees to pediatric surgery during postgraduate residency training in recent years has also led to a decrease in comfort with overall HPS surgical management. 4
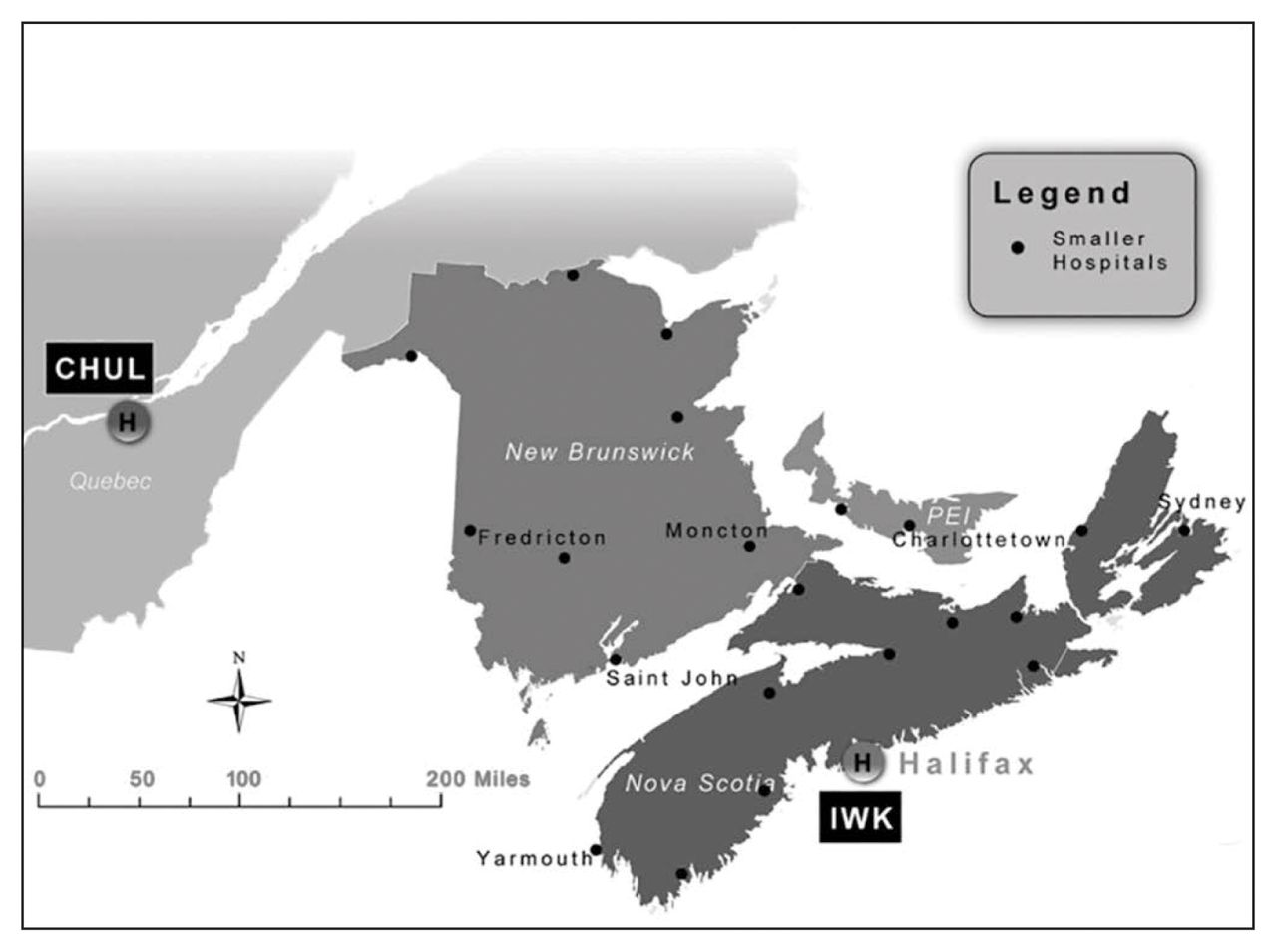
The Maritime provinces — Nova Scotia, New Brunswick and Prince Edward Island (PEI) — serve as an excellent “laboratory” in which to examine referral patterns of HPS (Fig. 1). The most populated province, Nova Scotia (population of 913 462 in 20065), has the only pediatric hospital (IWK Health Centre) in the region, which serves all 3 Maritime provinces and is the main site of pediatric surgical expertise. In New Brunswick (population of 729–997 in 2006) and PEI (population of 135–851 in 2006), 4 and 2 large general hospitals, respectively, with dedicated nonsurgical pediatric services offer basic pediatric surgical care by general surgeons, with medical management (including preoperative resuscitation) managed by general pediatricians. In addition, francophone families in northern New Brunswick have historically been referred to the adjacent province of Quebec, where pediatric surgical services are provided at the Centre Hospitalier de l’Université Laval (CHUL).
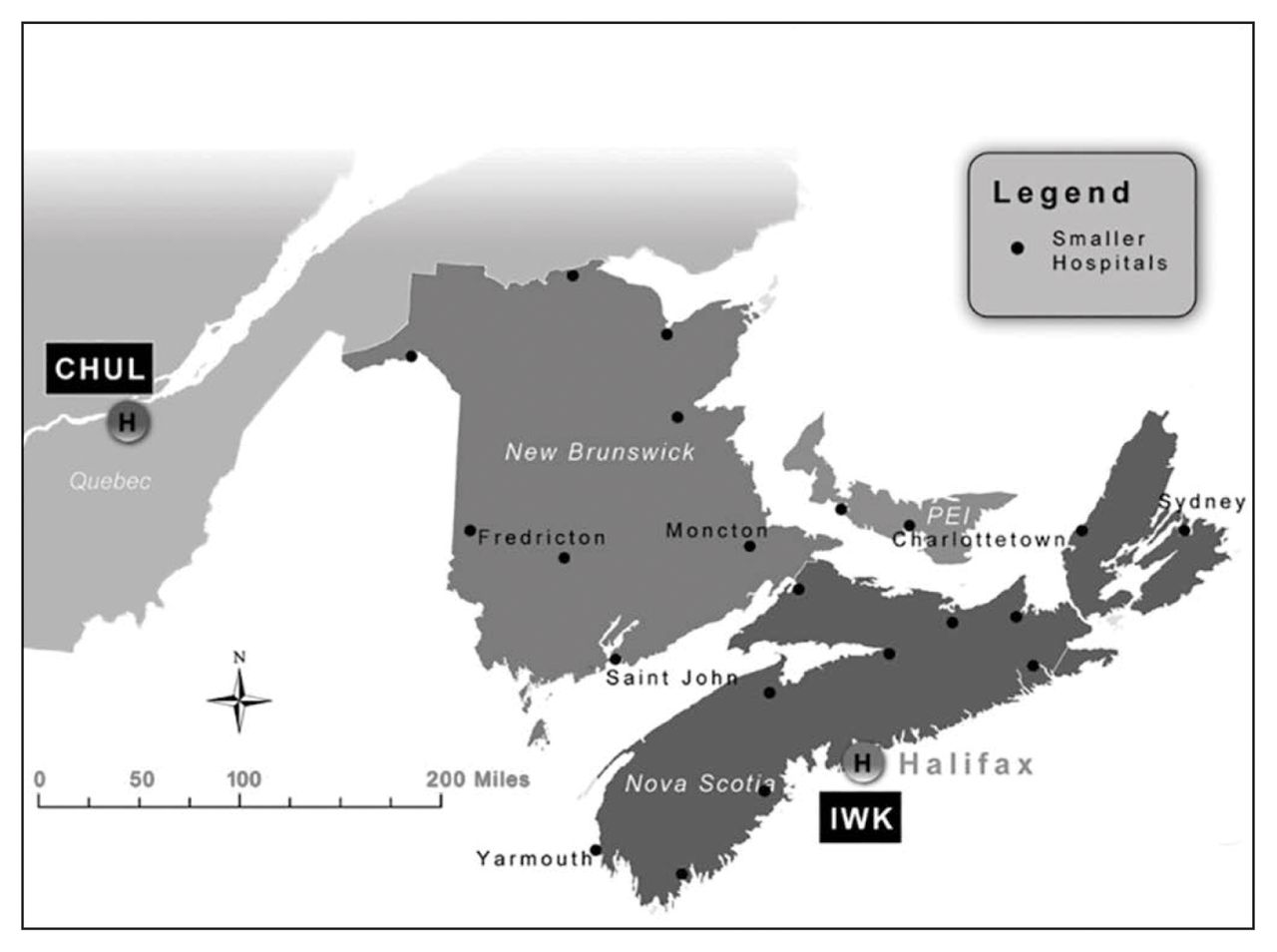
Location of hospitals involved in the study.
Our objective was to investigate the patterns of HPS referral changes in the Maritimes over time and correlate these patterns with patient outcomes. We also endeavoured to quantify and correlate the burden on families with referral patterns, as reflected by distance travelled for surgical care.
Methods
We contacted the medical records departments of all hospitals with pediatric services in the 3 Maritime provinces to identify patients with a discharge diagnosis of HPS during the study period (Jan. 1, 2001–Dec. 31, 2010). Pediatricians or surgeons at each centre with eligible cases were recruited to complete a chart review of such cases. The pediatric hospital in Quebec (CHUL) that takes referrals from New Brunswick was also contacted and queried. Locations of all hospitals involved in the study are shown in Figure 1. This study was approved by the Research Ethics Board of each centre in the study.
Cases included all patients discharged from hospital between Jan. 1, 2001, and Dec. 31, 2010, who had a diagnosis of HPS; a residential address in New Brunswick, Nova Scotia or PEI; and who had a pyloromyotomy (open or laparoscopic). Data included patient name, date of birth, sex, postal code, age at diagnosis, hospital of first admission, hospital of transfer (if transferred to second hospital for surgery), hospital of surgery (coded as pediatric or nonpediatric), date of surgery, overall preoperative length of stay (LOS; defined as tine from date of first admission to date of surgery, including LOS at first hospital if ultimately transferred), postoperative LOS (defined as time from surgery to final date of discharge), total LOS (defined as time from date of first admission to final date of discharge) and complications (wound infection, leak, or death). Three management groups were established: group 1 included patients who underwent resuscitation and surgery in a pediatric centre, group 2 included those who underwent initial/all resuscitation in a peripheral centre and surgery in a pediatric centre, and group 3 included patients for whom all management occurred in peripheral centre(s). Two time periods were established: the early period included patients with a surgery date between Jan. 1, 2001, and Dec. 31, 2005, and the late period included those with a surgery date between Jan. 1, 2006, and Dec. 31, 2010. Outcomes of interest included preoperative LOS as a proxy measure in efficiency of resuscitation and accessing operating room services, postoperative LOS as a proxy measure of clinical outcome and complications, and total LOS as a measure of overall efficiency of resource utilization.
To determine the burden on families if cases were referred to 1 of the 2 pediatric centres for surgery, driving times from the family’s place of residence to the pediatric centre for all patients who ultimately had surgery performed at one of the pediatric centres were stratified by time period. The driving times were calculated using the ODMatrix function in the Network Analyst tool in ArcGIS 10.1. We used DMTI route logistic as the network road data for driving time. Geopinpoint software was used to geocode all patients’ postal codes.
Statistical analysis
We used descriptive statistics and univariate analyses to determine associations between variables associated with patient management and outcomes of interest. Continuous variables (LOS) were dichotomized at the level of the upper quartile. Unadjusted odds ratios (ORs) of associations were determined using χ2 analyses. For the main outcome of interest, total LOS, we applied backward stepwise logistic regression using all variables reaching a level of p < 0.20 to determine the adjusted ORs, with 95% confidence intervals (CIs) not spanning 1.0 and a value of p > 0.05 ultimately considered to be significant. All statistical analyses were performed using SAS statistical software, version 8.2.
Results
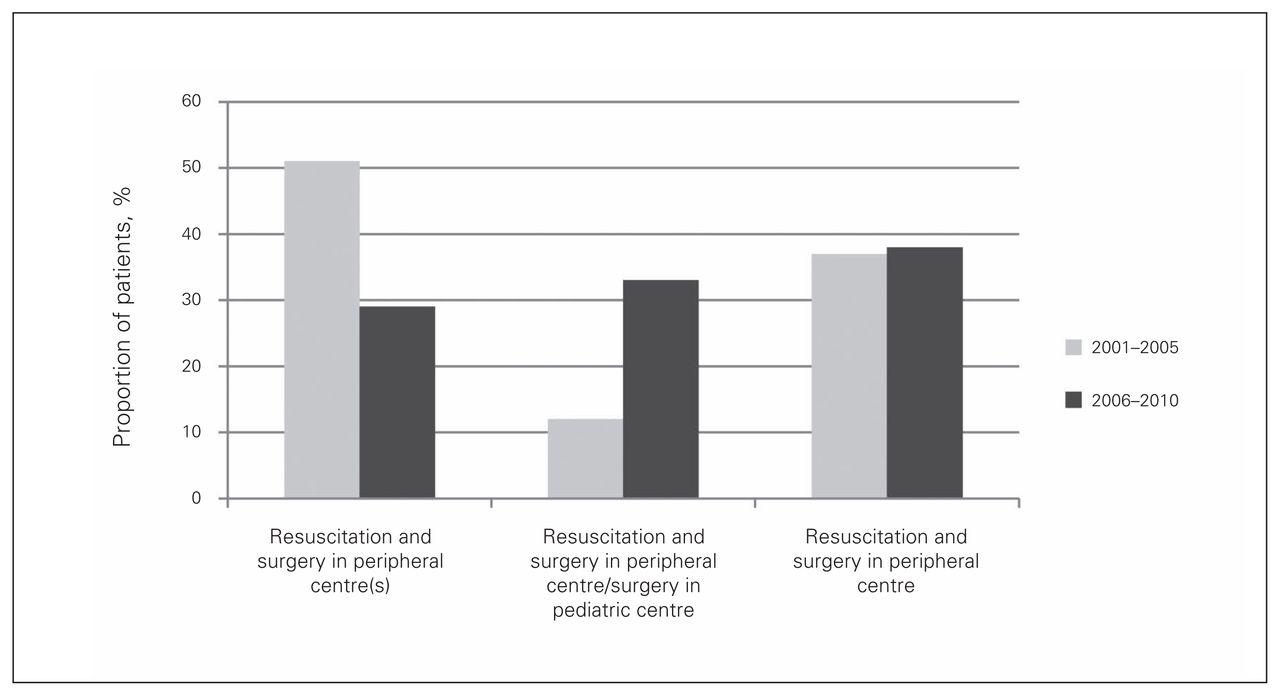
A total of 751 infants meeting our inclusion criteria were identified during the study period. Forty-seven percent (n = 353) had surgery in the early time period (Table 1). Thirty-seven percent (n = 280) were admitted to the pediatric centre for both resuscitation and surgery (group 1), 23% (n = 175) were transferred to a pediatric centre after resuscitation in a peripheral centre (group 2) and the remaining 39% (n = 296) had resuscitation and surgery in the peripheral centres only (group 3; Table 2).
Demographic and clinical characteristics of the study sample, by time period
Clinical characteristics of study sample, by referral group
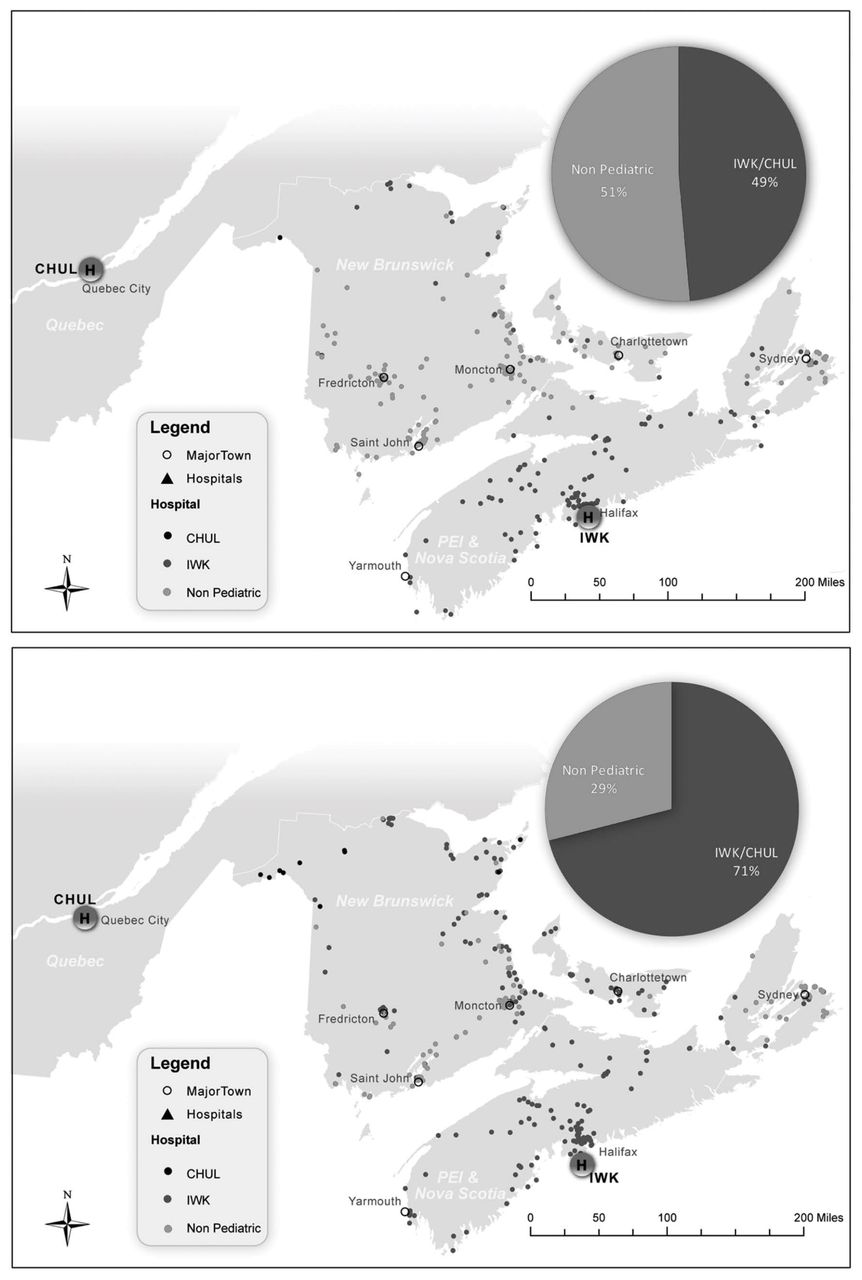
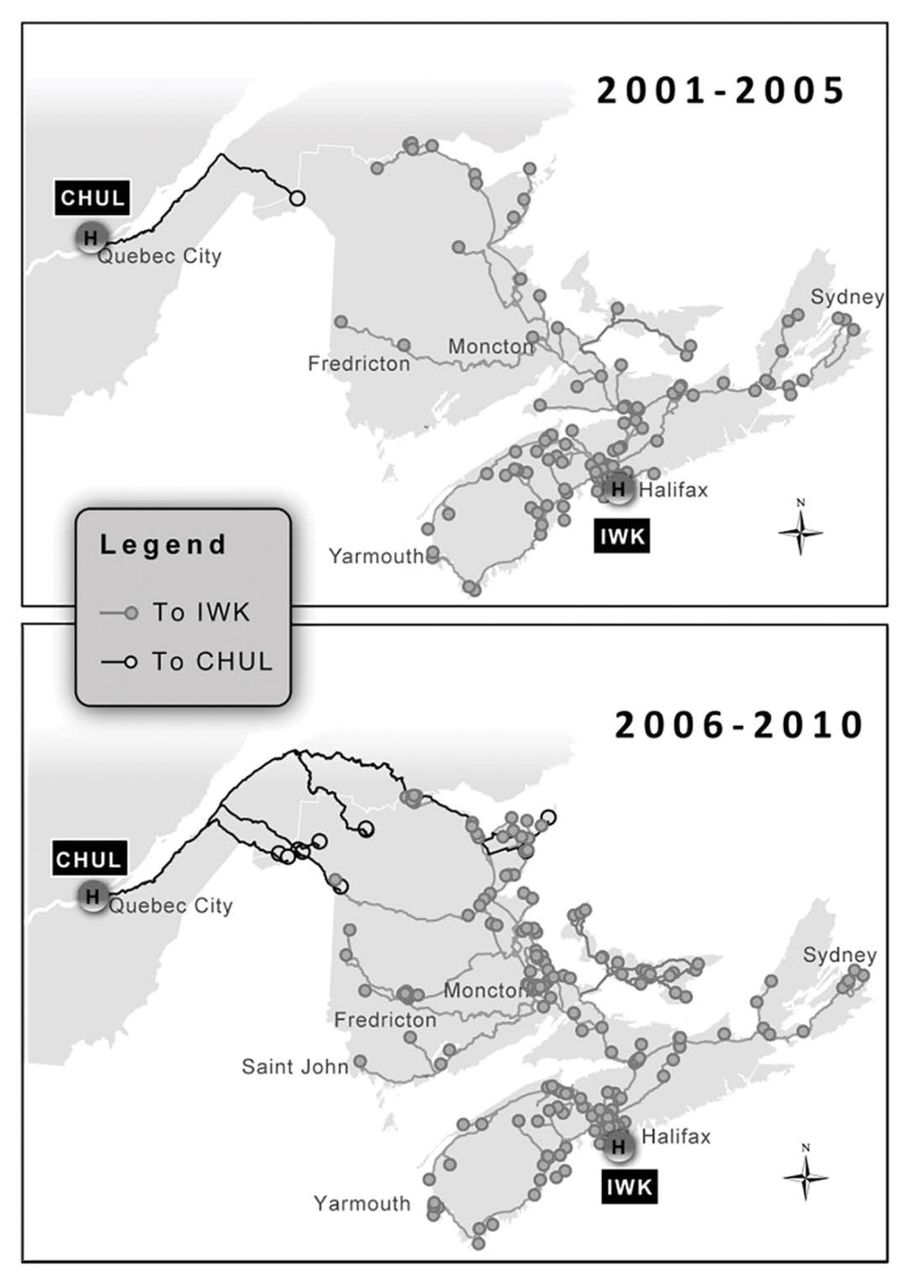
Figure 2 and Figure 3 depict the changes in referral patterns between the 2 time periods, with the proportion of infants having surgery in a pediatric centre increasing from 49% in the early period to 71% in the later period with the inclusion of patients resuscitated in a peripheral hospital. Most of this change appears to have occurred with patients in the 2 Maritime provinces without pediatric centres (New Brunswick and PEI). Despite this, however, there was little apparent change in the proportion of infants undergoing all of their preoperative resuscitation at a pediatric centre. Over the 2 time periods, these findings translated to a 6-fold increase in overall driving times to pediatric centres from the patients’ places of residence (Fig. 4).

Changes in referral patterns between the 2 time periods.
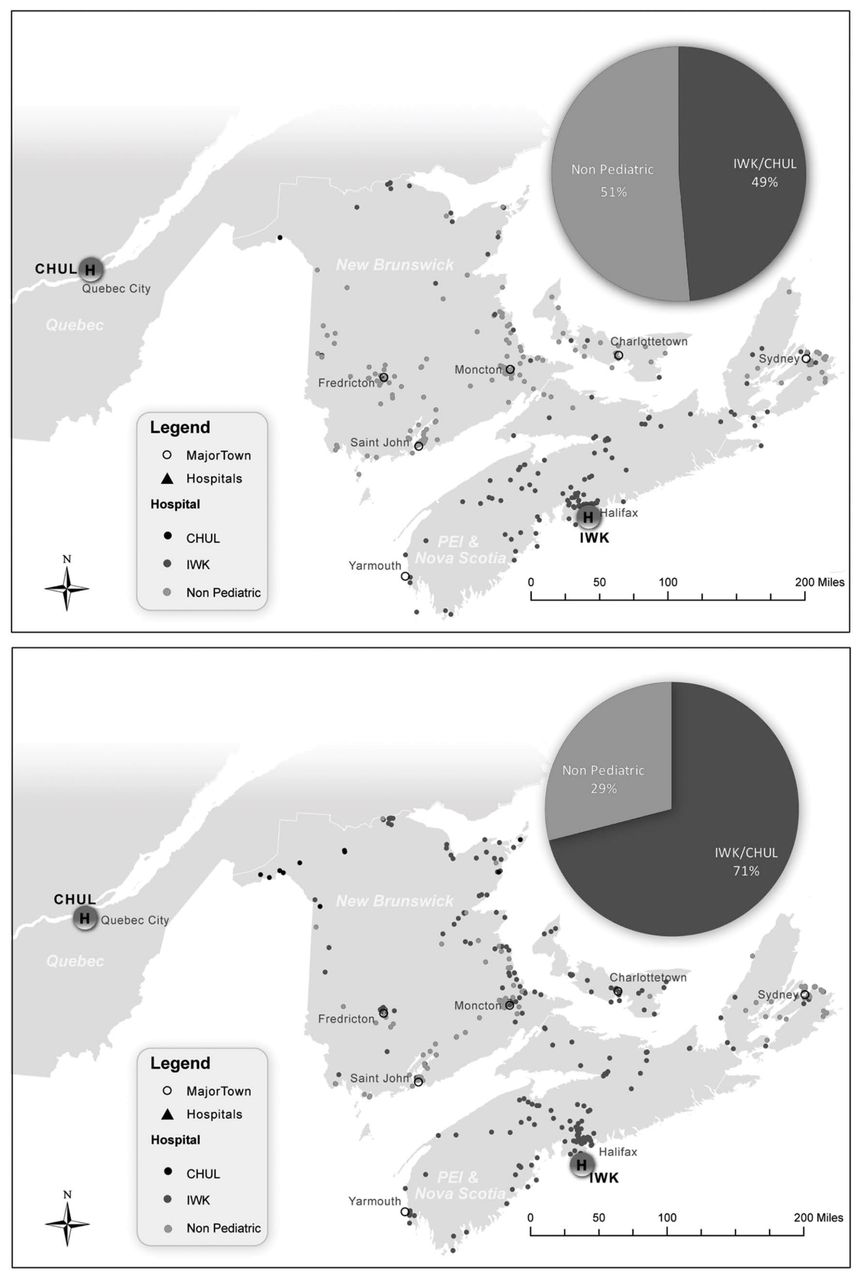
Changes in referral patterns between the 2 time periods, with geographical distribution of all cases based on postal codes.
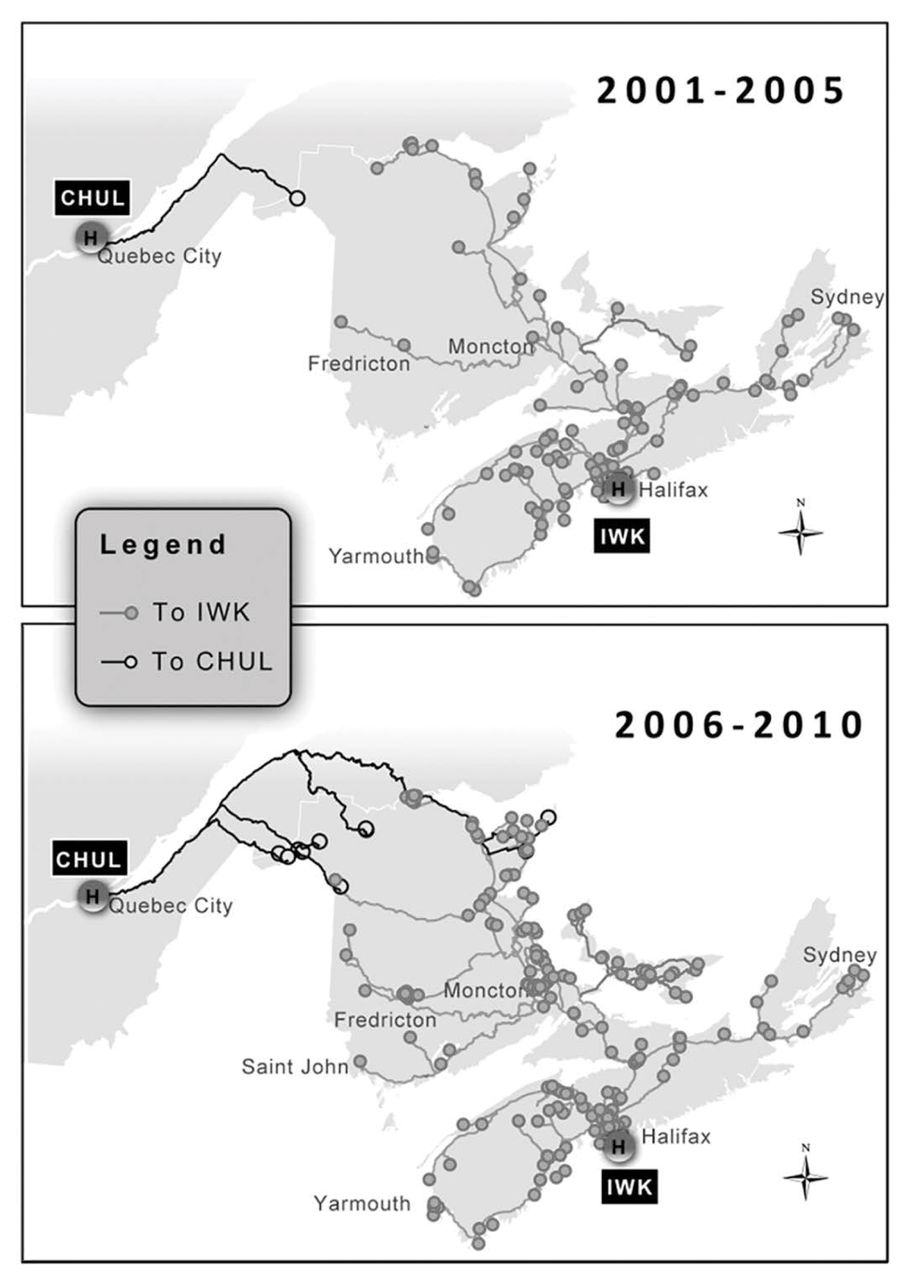
Changes in referral patterns led to a 6-fold increase in overall driving times to pediatric centres from the patients’ places of residence.
Table 2 depicts variations in outcomes relative to the 3 referral pattern groups. All LOS parameters were significantly increased with management in the peripheral centres, whether preoperative resuscitation or surgery. Postoperative complications also increased 2.5-fold with surgery in the peripheral centres.
Table 3 depicts associations with overall longer total LOS beyond 3 days. After adjusting for all covariates, infants who were referred to the pediatric centres for surgery were 78% less likely to have an overall LOS longer than 3 days. Infants with postoperative complications (excluding death) had a 3.2-fold increased risk of a longer LOS. There appeared to be no association between the time period and the overall LOS of these patients. Although protective with univariate analysis, a laparoscopic approach, which was practised at only 1 of the pediatric centres, was associated with a 50% increased risk of a longer overall LOS. This was no longer statistically significant, however, when stratified for time period (p = 0.45 for the early period; p = 0.89 for the later period; data not shown). When only postoperative LOS was considered, logistic regression revealed significant positive associations between postoperative complications and an LOS longer than 2 days (OR 9, 95% CI 4–29), while having surgery in a pediatric centre (OR 0.29, 95%CI 0.1–0.3) and having a laparoscopic procedure (OR 0.33, 95% CI 0.3–0.9) were both significantly protective.
Factors associated with overall longer total LOS beyond 3 days
Table 4 depicts associations with postoperative complications. After controlling for covariates, having surgery in a pediatric versus a nonpediatric centre was the only variable that retained significance and was associated with a 3-fold reduced risk of complications.
Factors associated with postoperative complications
Discussion
Management of HPS in the Maritimes between 2001 and 2010 demonstrated a clinically significant change in practice, with a more than 2.5-fold increase in the proportion of infants undergoing diagnosis and at least initial resuscitation in a nonpediatric centre followed by referral to a pediatric centre for definitive surgical care. This was associated with a significant decrease in the proportion of infants requiring a prolonged postoperative LOS, but no change in the proportion of infants with a prolonged inhospital LOS overall, likely related to the fact that the proportion of infants undergoing diagnosis and initial resuscitation in peripheral centres changed little between time periods. Although the overall complication rate did not change between time periods, undergoing surgery in a pediatric centre was clearly protective for postoperative complications.
McAteer and colleagues6 found a similar trend in the state of Washington for preferential referral to pediatric centres for appendicitis and HPS between 1987 and 2009. In their study, referral to pediatric centres in Washington was associated with decreased postoperative complications. Lower complication rates associated with treatment in pediatric centres have been demonstrated in multiple other studies, likely attributable to subspecialty training, higher volume and greater experience among all staff.7–10 Based on this evidence, all pediatric operations should ideally be performed at specialized pediatric centres. Unfortunately, this can create difficulties in light of Canada’s large geographic distribution.
A few studies have found that general surgeons have similar outcomes and complication rates for appendectomies and pyloromyotomies as long as a minimum number of procedures are performed per year, suggesting that some pediatric surgeries can be performed safely in the community setting.11–13 However, risk of complications, especially with pyloromyotomies, is still increased if not performed in a pediatric centre.11 In addition to surgical experience, the comfort level of anesthesiologists who do not normally treat children must also be taken into account.
Finally, as a result of increases in specialization as well as limitations in trainee work hours, the newer generations of general surgeons have less exposure to infants and children than prior generations, limiting their experience and comfort in the management of this patient population. As a result, the trend of increased referrals of this patient population to regional pediatric centres for surgical care seen in this study will be further exaggerated. In the case of pyloric stenosis in this study, there was no change in immediate referral upon diagnosis, as a similar proportion of infants underwent some or all preoperative resuscitation in the periphery between the 2 time periods. However, shorter preoperative stay observed when all treatment occurred at a pediatric centre suggests that this preoperative resuscitation may be more efficient when done at specialized hospitals. Therefore, immediate transfer upon diagnosis may be more cost-effective and result in better overall outcomes. Adding to the debate of pediatric surgical centralization, Cosper and colleagues14 found there was a higher hospital cost for patients treated in specialized pediatric centres compared with community settings.14 For HPS, however, this cost was only 9% above the mean and could be offset by the costs of higher complication rates. Furthermore, alternative approaches more commonly performed at pediatric centres, including periumbilical and laparoscopic pyloromyotomies, can improve cosmesis without increasing complication rates.15 As seen in other studies, our study found no differences in complication rates or LOS with a laparoscopic approach.16 This study was not powered to look at this specifically; larger studies examining this specific variable are needed to determine any true effect of a minimally invasive approach to pyloromyotomies.
The mental and physical burden on the patient, as well as the emotional and financial burden of travelling incurred by the family for pediatric surgical care is not to be underestimated.17 Studies have demonstrated the willingness of parents to travel significant distances for the potential outcome improvements at specialized hospitals. 18,19 Our study highlights the travel burden (approximated by total kilometers to facility of treatment) families encounter in the Maritimes while relocating for specialized pediatric care. At the IWK Health Centre, local housing resources are made available for parents but likely do not completely eliminate stress on the family, although this was not formally assessed in our study. Further studies focusing on particular family stressors may help identify specific areas for assisted resource allocation for families travelling long distances for pediatric surgical care.
The benefits of lower complication rates, shorter LOS and improvements in overall outcomes associated with management of HPS at pediatric centres imply that all cases of HPS should be primarily referred to a pediatric centre for management. The burden of travel and financial stress on the family unit, while potentially substantial, is outweighed by the gains in outcomes. These findings were corroborated in studies in Washington and Ontario.6,7
The topic of pediatric surgical regionalization is not a novel concept, and there is substantial evidence to suggest that the majority of pediatric surgery should be performed at pediatric centres to decrease overall morbidity, mortality and LOS. Increased pediatric centre referral is a trend in multiple areas of North America. In order to streamline HPS management, policies requiring referral of all cases of HPS to a pediatric centre for definitive management may be required. These changes may help to allocate funds and resources to offset the burden on families of infants being treated.
Conclusion
Our study supports similar observations in the literature of improved outcomes, shorter overall LOS and decreased risk of complications when infants with HPS are referred to a regional pediatric centre for preoperative resuscitation and surgery in the Maritime provinces of Canada. This should be considered when planning access to pediatric surgical resources in other parts of the country to ensure optimal outcomes for all children with HPS. Caution should be taken to not completely limit all pediatric surgery to specialized centres, as this could result in inadequate experience for the management of patients with acute surgical emergencies who cannot afford the time of transfer. National authoritative bodies, such as the British Association of Paediatric Surgeons, have taken steps to develop guidelines to streamline access to appropriate pediatric surgical care services in order to maximize outcomes on individual patient and population levels.20 Development and ongoing evaluation of such guidelines should be considered in Canada and elsewhere.
Acknowledgements
The authors thank Drs. Barbara Bulleid, Anne Canning, Nidal Chami, Andrew Lynk, Cecil Ojah and David Wong for data collection at their regional hospital sites.
Footnotes
Competing interests: None declared.
Contributors: J. Creaser and N. Yanchar designed the study. J. Creaser and S. Leclerc acquired the data, which A. Ednie, O. Amram, J. Creaser, N. Schuurman and N. Yanchar analyzed. A. Ednie and N. Yanchar wrote the article, which all authors reviewed and approved for publication.
- Received October 1, 2016.
- Accepted May 17, 2016.
References

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools


