


Abstract
Background: There are several different techniques commonly used to perform intramedullary (IM) nailing of the femur to fix femoral fractures. We sought to identify significant differences in outcomes of studies comparing 1) trochanteric and piriformis entry and 2) antegrade and retrograde entry in IM nailing of the femur.
Methods: We searched MEDLINE, Cochrane and Embase databases and the Orthopaedic Trauma Association and American Academy of Orthopaedic Surgeons websites for comparative studies published from inception to November 2015. Criteria used to select articles for detailed review included use of antegrade and retrograde entry point or use of trochanteric and piriformis entry point for IM nailing of the femur in adult patients. Functional and technical outcomes were extracted from accepted studies.
Results: We identified 483 potential studies, of which 52 were eligible. Of these, we included 13 publications and 2 abstracts (2 level I, 7 level II and 6 level III studies). Trochanteric entry significantly reduced operative duration by 14 min compared with piriformis entry (p = 0.030). Retrograde nailing had a greater risk of postoperative knee pain than antegrade nailing (p = 0.05). On the other hand, antegrade nailing had significantly more postoperative hip pain (p = 0.003) and heterotopic ossification (p < 0.001) than retrograde nailing. No significant differences in functional outcomes were observed.
Conclusion: Although some significant differences were found, the varying quality of studies made recommendation difficult. Our meta-analysis did not confirm superiority of either antegrade over retrograde or trochanteric over piriformis entry for IM nailing of the femur.
Level of evidence Level III therapeutic.
Intramedullary (IM) nailing is a proven and effective method for the management of femoral shaft fractures. 1,2 The appropriate entry point can make nail insertion easier, affect fracture reduction, and may prevent complications.1,3 Although both ends of the femur are suitable, there is debate in the literature concerning antegrade versus retrograde entry and, in antegrade nailing, the choice of the piriformis fossa versus greater trochanter as an entry point.1,4 Antegrade nailing is useful for the treatment of proximal femoral fractures; however, studies have found it to result in damage to the hip abductors and sometimes the pudendal nerve if the patient is in the supine position on a fracture table.5 Retrograde nailing is advantageous for patients with multiple injuries, patients sustaining ipsilateral femoral neck and shaft fractures and obese patients;6 however, it may be accompanied by higher rates of knee pain and lower rates of union.7 The entry point for antegrade nailing is also controversial, with advocates for both piriformis and trochanteric entry.4,8,9 The piriformis fossa is colinear with the medullary canal, allowing for straight nails to be inserted easily. However, the piriformis is difficult to access in obese patients, leading to interest in the greater trochanter as an alternative antegrade entry point.1 To our knowledge, a comprehensive systematic review or meta-analysis to summarize the effects of various entry points for IM nailing of the femur has not been performed.
The purpose of this study was to identify significant differences in outcomes of studies comparing 1) trochanteric and piriformis entry and 2) antegrade and retrograde entry in IM nailing of femoral shaft fractures. We conducted a systematic review and meta-analysis using randomized controlled trials (RCTs) and prospective and retrospective comparative studies assessing rates of reoperation, dynamization, union, malalignment, nonunion, delayed union, pain, complications, mortality, operative duration, blood loss and functional outcomes in patients with femoral shaft fractures.
Methods
Eligibility criteria
Three authors (F.N.H., A.S. and P.K.) reviewed each article independently and determined their eligibility based on the following preset inclusion criteria: use of antegrade, retrograde, trochanteric entry or piriformis entry for IM nailing of the femur in adult (age > 18 yr) patients. Based on the search strategy developed, 3 authors (F.N.H., A.S. and P.K.) independently screened the results based on title and abstract alone and then screened all potentially eligible articles via full text. Disagreements were resolved by a consensus meeting.
Search strategy
Comparative studies in English were identified through a systematic search of MEDLINE, Embase, and Cochrane databases from inception to November 2015. The database search strategy was “femur AND fracture AND nail AND (antegrade OR retrograde).” The search strategy used was broad in order to encompass all potentially relevant articles. We examined the bibliographies of retrieved studies. We also searched the Orthopaedic Trauma Association (OTA) and American Academy for Orthopaedic Surgeons (AAOS) websites.
Assessment of study quality
Eligible studies were read in full by 3 authors (F.N.H., A.S. and P.K.). Each author independently assessed the methodological quality of included studies using the Cochrane Bone, Joint and Muscle Trauma Group reporting quality assessment tool.10 This 12-item questionnaire assesses the methodological quality of reports of RCTs. The final reported scores for each study were determined by consensus.
Data abstraction
The relevant data were extracted from each study and recorded in a database. Information on the manufacturer and type of IM nails; number of patients and femoral shaft fractures; patient sex, age and body mass index (BMI); follow- up rate; functional outcome measures; operative duration; presence of pain; and rates of nonunion, malunion, reoperation, dynamization and femoral shortening was included.
Evaluation of agreement
Agreement among the 3 reviewers (F.N.H., A.S. and P.K.) on scoring the studies was evaluated using the κ statistic, with a score of 0 indicating chance agreement and a score of 1 indicating perfect agreement among the raters.11
Statistical analysis
We calculated the mean difference for operative duration and used the standard deviation (SD) to estimate the variance. If the SD was not available, it was calculated using standard error derived from a p value. If p values were unavailable, the SD was estimated using the range. All calculations were made according to methodology in the Cochrane Handbook.10 The values obtained may be imprecise because the imputation methods used make assumptions about unknown data.10
We calculated risk ratios (RR) and 95% confidence intervals (CI) for the following dichotomous outcomes: union, nonunion/delayed union, malalignment (varus–valgus, longitudinal angular and rotational), femoral shortening, knee pain, hip/thigh pain, dynamization, heterotopic ossification and reoperations. A random-effects model was used to pool the relative risk estimates from these studies.12
Two-tailed tests of significance for treatment effects were used. We considered results to be significant at p < 0.05. RevMan software version 5.0 (The Nordic Cochrane Centre) was used to statistically analyze all pooled outcomes.
Evaluation of heterogeneity
To evaluate the extent to which the results of the subgroups differed from one another, stratified analyses and a statistical test of interaction were performed.13 The I2 statistic was used to quantify heterogeneity among studies, with an I2 value of 0%–40% representing low heterogeneity and values greater than 40% representing moderate to high heterogeneity.10 As a result, we evaluated heterogeneity on the basis of study design and overall study quality when I2 was above 40%.
Results
We identified 483 potential studies. We eliminated 431 studies after reviewing their titles and abstracts, leaving 52 studies for full text screening. Following full text screening, we included a total of 13 publications and 2 abstracts, 4 of which compared greater trochanter with piriformis entry, and 11 of which compared antegrade with retrograde entry (Fig. 1). Our assessment of study quality is summarized in Table 1. Studies were excluded for several reasons, including a lack of an adequate compartor group and a lack of live human participants. Our review includes articles reporting on a total of 1140 femoral shaft fractures treated with antegrade or retrograde nailing and 267 femoral shaft fractures treated with antegrade nailing from the greater trochanter or piriformis fossa (Table 2 and Table 3).

Identification of trials comparing greater trochanter with piriformis entry, and antegrade with retrograde entry in intramedullary nailing of the femoral shaft.
Quality of the 13 comparitive studies assessed using the Cochrane Bone, Joint and Muscle Trauma Group reporting quality assessment tool
Characteristics of included trials comparing antegrade with retrograde intramedullary nailing of the femoral shaft
Characteristics of the 4 included trials comparing greater trochanter with piriformis entry in intramedullary nailing of the femoral shaft
Sample demographics
Overall, the population sampled was similar among studies and was representative of the typical femoral shaft fracture population. The mean age of patients ranged from 21.75 to 52.15 years. The percentage of male patients ranged from 55% to 91%. The BMI ranged from 24 to 29. Except for 1 study in each comparison, the studies followed patients for longer than 12 months. The follow-up rate, when reported, was 14%–100% (Table 2 and Table 3).
Among the studies comparing antegrade with retrograde entry, 5 reported a greater number of distal femoral fractures in the retrograde group14,16–18,25 (Table 2). Although not significant, the reported BMI tended to be greater in patients assigned to trochanteric entry over piriformis entry4,8 (Table 3).
Description of surgical techniques used for placement of IM nails
Two surgical methods were used for placement of IM nails. In studies comparing trochanteric with piriformis entry, 2 used a fracture table for both groups (Table 3). In studies comparing antegrade with retrograde entry, 3 used a radiolucent table in both groups, 3 used a fracture table for antegrade nailing and a radiolucent table for retrograde nailing, and 1 used both methods for antegrade nailing and a radiolucent table for retrograde nailing (Table 2).
Operative duration and blood loss
Six studies comparing antegrade with retrograde entry in 396 fractures reported operative duration14,15,20–22,25 (Table 4). Two studies14,22 did not report an SD, p values or ranges, so the mean difference could not be estimated; however, these 2 studies reported no significant difference in operative duration. Therefore, 4 studies15,20,21,25 reporting on 242 fractures were included in this analysis. There was no significant difference in operative duration between the 2 groups in this analysis (95% CI –21.31 to 15.61, p = 0.76, I2 = 85%; Fig. 2). Two studies comparing trochanteric with piriformis entry in 125 fractures reported operative duration4,8 (Table 5). Operative duration was 14 min shorter when trochanteric entry was used than when piriformis entry was used, and this difference was sigificant (95%CI –26.67 to –1.34, p = 0.030, I2 = 0). Heterogeneity was not successfully resolved when the results were categorized by study design. Further exploration on the basis of overall study quality also did not resolve heterogeneity.

Trials comparing operative duration in patients treated with antegrade or retrograde nailing of the femur. CI = confidence interval; SD = standard deviation.
Summary of outcome measures for antegrade versus retrograde studies
Summary of outcome measures for trochanteric versus piriformis studies
Four studies14,19,22,25 estimated blood loss in patients treated with either antegrade or retrograde nailing (Table 4). The results could not be pooled owing to unreported p values and/or ranges. Ricci and colleagues25 reported significantly higher levels of blood loss in patients treated with antegrade nailing, while Ostrum and colleagues, 14 Tornetta and Tiburzi,19 and Dougherty and colleagues22 found no significant differences.
Union
Four studies4,8,9,24 reported rates of union and delayed/nonunion in patients treated with trochanteric or piriformis nailing (Table 5). One study21 did not indicate the number of patients allocated to each treatment arm and was excluded from this analysis. Therefore, 3 studies4,8,9 reporting on 233 fractures were included. There was no significant difference between the 2 treatment groups.
Six studies14,19,20,22,23,25 examining 576 fractures reported rates of union and delayed/nonunion in patients treated with either antegrade or retrograde IM nailing (Table 4). There were no significant differences found among the studies between the 2 treatment groups.
Malalignment and femoral shortening
We defined malalignment as ≥ 5° of deformity in any plane.26–28 Two studies4,8 examining 125 fractures treated with either trochanteric or piriformis nailing reported rates of malalignment (Table 5). There was no significant difference between the 2 treatment groups (RR 2.3, 95% CI 0.57–9.34, p = 0.24, I2 = 0%). Six studies14–16,18–20 examining 693 fractures treated with either antegrade or retrograde nailing reported rates of malalignment (Table 4). There was no significant difference between the 2 treatment groups (RR 0.9, 95% CI 0.57–1.56, p = 0.82, I2 = 42%). Heterogeneity was not successfully resolved when the results were categorized by study design. Further exploration on the basis of overall study quality also did not resolve heterogeneity. Reported rates of varus–valgus, longitudinal and rotational malalignment or deformity did not differ significantly between the 2 groups.
Femoral shortening was defined as inequality in limb length ≥ 10 mm. Data from 3 studies16,19,20 comparing antegrade with retrograde nailing in 140 fractures yielded no significant difference (RR = 0.6, 95% CI 0.16–1.98, p = 0.38, I2 = 35%).
Pain
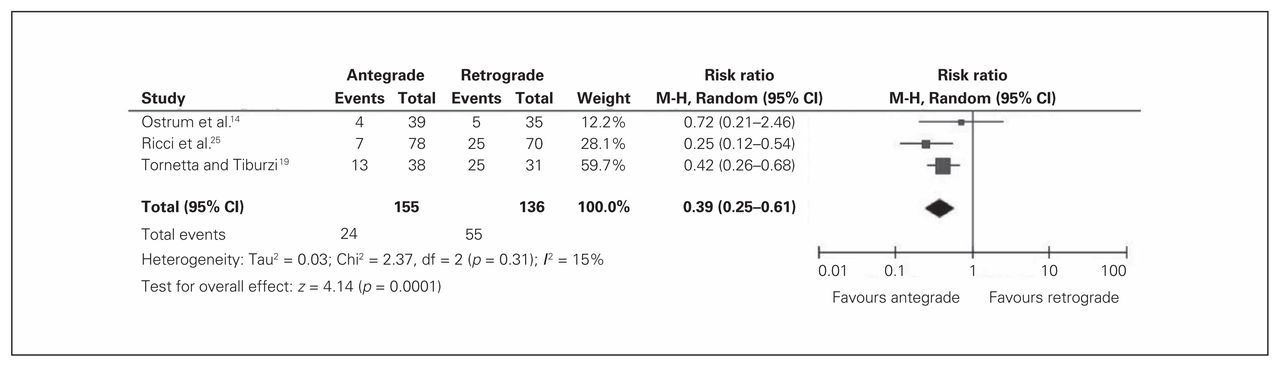
Rates of postoperative pain in the knee and hip/thigh were pooled from studies comparing antegrade with retrograde nailing. Three studies14,19,25 examining 291 fractures reported knee pain (Table 4). The results were significantly in favour of antegrade nailing (RR 0.4, 95% CI 0.25–0.61, p < 0.001, I2 = 15%; Fig. 3). Two studies14,25 examining 256 fractures reported hip/thigh pain (Fig. 2). The risk of having hip/thigh pain was significantly greater in those receiving antegrade nailing than in those receiving retrograde nailing (RR 4.3, 95% CI 1.66–11.10, p = 0.003, I2 = 0; Fig. 4). No studies examining trochanteric versus piriformis entry reported rates of postoperative pain.
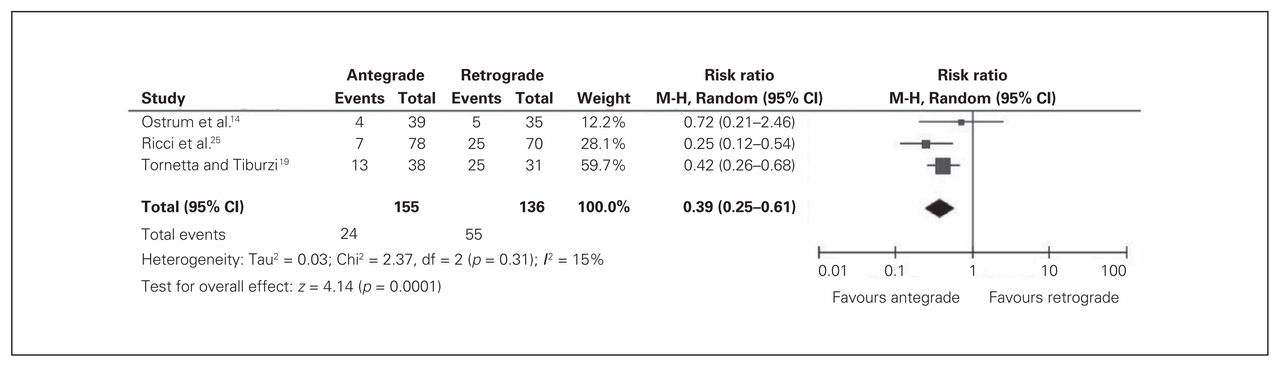
Trials comparing knee pain in patients treated with antegrade or retrograde nailing of the femur. CI = confidence interval; M-H = Mantel-Haenszel.

Trials comparing hip/thigh pain in patients treated with antegrade or retrograde nailing of the femur. CI = confidence interval; M-H = Mantel-Haenszel.
Reoperations and dynamization
There were no significant differences in rates of reoperation (RR 1.0, 95% CI 0.57–1.72, p = 0.98, I2 = 5%) or dynamization (RR 0.6, 95% CI 0.19–1.65, p = 0.30, I2 = 12%) in studies comparing antegrade with retrograde nailing (Table 4).
Functional outcomes
The studies that reported functional outcomes used different tools for assessment. Therefore, the results could not be pooled. Three studies4,8,9 comparing trochanteric with piriformis nailing reported postoperative functionality (Table 5). None of the studies found significant differences. Archdeacon and colleagues24 reported significant differences in hip range of motion (ROM; p = 0.025) favouring trochanteric nailing. Three studies16,17,20 that examined outcomes after antegrade or retrograde IM nailing reported postoperative functional outcomes (Table 4). Murray and colleagues17 reported that the Knee Injury and Osteoarthritis Outcome Scores were significantly worse (p = 0.005) in the retrograde group (Table 4).
Mortality and complications
Reported deaths in both comparisons were found to be nonsignificant (Table 4 and Table 5).
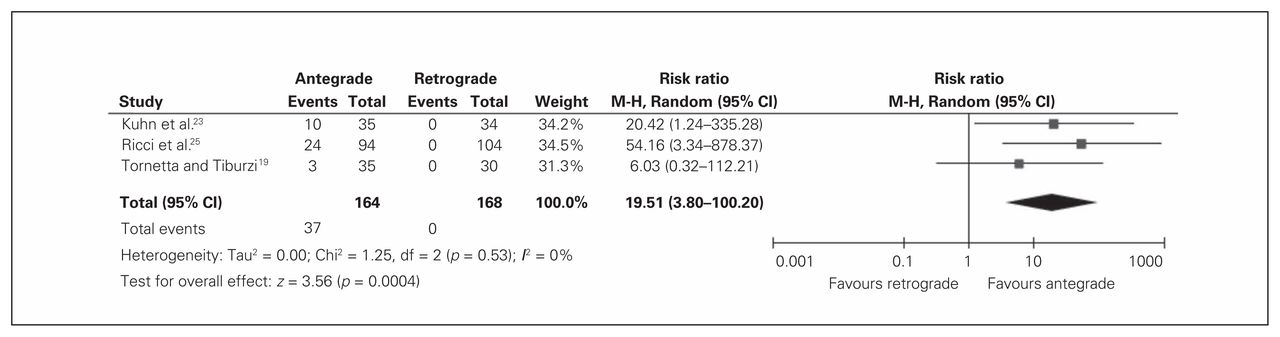
Radiographic evidence of heterotopic ossification (HO) around the hip was reported in 3 studies19,23,25 comparing antegrade and retrograde nailing (Table 4). There was a significantly greater risk of HO with antegrade nailing than with retrograde nailing (RR 19.51, 95% CI 3.80–100.20, p < 0.001, I2 = 0%) favouring retrograde nailing (Fig. 5); however, only 1 study23 reported on symptomolgy associated with HO. Of the 10 patients who had radiographic evidence of HO, only 1 had associated symptoms.

Trials comparing heterotopic ossification around the hip in patients treated with antegrade or retrograde nailing of the femur. CI = confidence interval; M-H = Mantel-Haenszel.
For the remainder of the complications, each study reported different outcomes, which could not be statistically pooled. Within the studies comparing antegrade with retrograde nailing, Ostrum and colleagues14 reported that a Trendelenburg gait was present in all 39 patients treated with antegrade nailing and absent in the 35 patients treated with retrograde nailing. Differences between antegrade and retrograde treatment groups in other reported complications were not significant14,15,17,22,23,25 (Table 4).
In studies examining trochanteric versus piriformis nailing, Stannard and colleagues9 reported greater HO of the hip in the piriformis group. This difference was not significant (p = 0.10; Table 5).
Discussion
The results of this systematic review and meta-analysis suggest that retrograde nailing is favourable over antegrade nailing in terms of hip pain and HO of the hip. However, the results also are in favour of antegrade nailing with respect to knee pain. Moreover, there was level-II14 evidence showing Trendelenburg gait, favouring retrograde nailing, and level-III17 evidence showing significant differences in knee function and ROM, favouring antegrade nailing. The only significant difference in the trochanteric versus piriformis pooled data was operative duration, which favoured trochanteric entry. There was also level-I evidence showing significant differences in hip ROM, favouring trochanteric nailing.
Studies show that the incidence of postoperative knee pain after retrograde nailing can be as high as 70%.7,29 Our study revealed that a statistically greater number of patients undergoing retrograde nailing than antegrade nailing experienced knee pain. The etiology of this pain has been attributed to events such as concomitant patellar or ligamentous injury from the initial trauma, sepsis of the knee joint, distal locking screws, quadriceps atrophy, or protruding nails.7,25,29,30 This may also explain the finding of Murray and colleagues,17 who showed that both knee function and ROM were significantly lower in patients treated with retrograde nailing. None of the studies had long enough follow-up to show an increased incidence of knee osteoarthritis (OA) with retrograde nailing. In the absence of a prominent nail within the knee joint or septic arthritis, the risk of knee OA is likely minimal; however, the long-term incidence of OA following retrograde nailing remains unknown. It is important to note that none of the studies reviewed in this meta-analysis reported any occurrence of septic arthritis.
Whereas Ostrum and colleagues14 and Tornetta and Tiburzi19 reported no significant differences between antegrade and retrograde nailing in terms of blood loss, Ricci and colleagues25 found levels of estimated blood loss to be significantly lower in patients treated with retrograde than antegrade nails. They attributed this finding to the use of a tourniquet during retrograde nail insertion; however, tourniquet usage was not mentioned in the other included studies. Additional studies have also shown retrograde nailing to be associated with minimal blood loss,31 which may be a result of reduced operative duration and soft tissue dissection. Another important finding among studies in this comparison was the greater presence of HO around the hip in patients treated with antegrade than retrograde nailing. This has been attributed to the requirements of additional muscle dissection and reamings from the femoral canal deposited in the soft tissues around the hip.5,6,32 However, only 1 study reported on symptoms caused by the HO, and none of the studies reported that patients required excision of HO. Therefore, the increase in HO with antegrade femoral nailing is not likely to be clinically significant. Furthermore, antegrade nailing frequently causes injury to the gluteus medius and minimus muscles and the superior gluteal nerve, causing abduction weakness. 33 Weak abductors may be easily fatigued when challenged, consequently resulting in pain and a Trendelenburg gait.33,34 This is a possible explanation for the statistically greater numbers of patients experiencing hip pain in the antegrade than the retrograde nailing group and the finding of a Trendelenburg gait in all patients treated with antegrade nails in the study by Ostrum and colleagues.14
No differences in union, delayed/nonunion, malalignment or femoral shortening were observed between antegrade and retrograde nailing. Previous studies evaluating retrograde nailing also shown rates of healing that were comparable to those of anterade nailing.29,30 Differences in other complications were found not to be significant. However, this could be attributed to the small sample size and the fact that not all authors reported the same complications.
Our analysis showed differences in operative duration between trochanteric and piriformis nailing treatment groups, and 1 level-I study24 showed significant differences in hip ROM, favouring trochanteric nailing. Cadaver studies have shown that nailing through the piriformis fossa penetrated muscles and tendons of the hip abductors and external rotators, including the gluteus medius muscle. 35,36 Replacement of these contractile fibres in living patients can have consequences for muscle function, and choosing a more lateral entry point, such as the greater trochanter, may be beneficial both for hip function and ease of access for the surgeon.35,36
Limitations
Our study had several limitations. In order to reduce bias and heterogeneity in the results, it would have been best to use only level-I studies or RCTs. However, there is a paucity of such trials examining viable entry points for femoral nailing, perhaps owing to the difficulty in performing these studies in acute orthopaedic trauma patients. Although several of the included studies were randomized, blinding or randomization was often inadequate and included a relatively small number of patients. Combining the results of RCTs and lower level studies, as presented here, greatly reduces the external validity of the pooled analysis. Moreover, the studies examined different outcomes of interest and often reported these outcomes differently, which made it difficult to statistically pool data and decreased the available sample size for each outcome. There was also variation among studies in terms of surgical technique, which may have contributed to heterogeneity and bias. Finally, 8 of the 15 studies had a loss to follow-up greater than 10%. Despite these pitfalls, we were able to elucidate some key findings from the included studies, which may be a helpful starting point for more methodologically rigourous studies.
Conclusion
Our meta-analysis did not confirm superiority of either antegrade over retrograde nailing, or trochanteric over piriformis entry in IM nailing of the femur. The 15 included studies varied in quality and outcomes reported, and thus higher-quality studies are required to clearly establish any recommendations. We suggest that surgeons use their best judgment as to the choice of entry point based on surgeon comfort with the technique and on patient and fracture characteristics.
Footnotes
Presented in part at the Canadian Orthopedic Association Annual Conference in Ottawa, Ont., 2012
Competing interests: E. Schemitsch has been a paid consultant with Stryker, Smith and Nephew and Zimmer for work unrelated to the products mentioned in this article. No other competing interests declared.
Contributors: N. Hussain, E. Schemitsch, A. Sternheim and P. Kuzyk designed the study. N. Hussain, F. Hussain, C. Sermer and P. Kuzyk acquired the data, which all authors analyzed. N. Hussain, F. Hussain, C. Sermer, H. Kamdar and P. Kuzyk wrote the article, which all authors reviewed and approved for publication.
- Received December 1, 2016.
- Accepted August 18, 2016.
References

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.