


Abstract
Background: The purpose of this study was to report the radiographic wear rates from a previous randomized controlled trial of first-generation highly crosslinked versus conventional polyethylene in total hip arthroplasty (THA) at a minimum of 13 years’ follow-up.
Methods: Patients returned for radiographic imaging and radiostereometric analysis (RSA). Radiographs were reviewed for the presence of osteolysis or component loosening. Femoral head penetration (which includes both wear and creep) was measured using RSA. We compared Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), 12-Item Short Form Health Survey (SF-12) and Harris Hip Scores (HHS) with preoperative values.
Results: There was 1 revision in each group. There was no difference in WOMAC, SF-12, or HHS outcome scores between the highly crosslinked and conventional polyethylene groups (all p ≥ 0.13). Wear rate was lower with crosslinked polyethylene than conventional polyethylene (0.04 ± 0.02 mm/year v. 0.08 ± 0.03 mm/year, p = 0.007).
Conclusion: First-generation crosslinked polyethylene demonstrates greater wear resistance than conventional polyethylene after 13 years of implantation. Crosslinked polyethylene continues to outperform conventional polyethylene into the second decade of implantation.
Highly crosslinked polyethylene was introduced for total hip arthroplasty (THA) with the goal of increasing wear resistance and improving implant longevity.1 Between November 1999 and October 2001, 100 consecutive patients from our institution were enrolled in a prospective randomized controlled trial.2 Patients were divided into 2 groups (of 50 patients each) and received either a conventional polyethylene liner (Trilogy, Zimmer Inc.) or a first-generation highly crosslinked polyethylene liner (Longevity, Zimmer Inc.). Patients and research staff were blinded to the intervention. The liners all had a 10° lip and an outer diameter of 48–58 mm. Both groups received a cemented collared femoral stem with a 28 mm diameter cobalt-chrome femoral head (VerSys, Zimmer Inc.) and a cementless tri-spiked acetabular cup (Trilogy, Zimmer Inc.). The operations were performed through a modified lateral approach by 1 of 5 experienced high-volume (> 100 cases per year) arthroplasty surgeons.
Results for this cohort were previously reported after a mean follow-up of 6.8 years. Age at surgery (mean 72 years) and body mass index (BMI; mean 29.7) was identical between groups. The male:female ratio was 14:36 in the conventional polyethylene group and 17:33 in the highly crosslinked polyethylene group. At the time of the previous report, 1 patient was lost to follow-up in each of the groups, and there were 2 deaths in the conventional group and 7 in the highly crosslinked group. There were no differences between the 2 polyethylene groups for the Harris Hip Score (HHS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), or 12-Item Short Form Health Survey (SF-12). The mean steady state femoral head penetration rate for the first 5 years postimplantation (excluding bedding-in) was lower in the highly crosslinked group than the conventional group (0.003 ± 0.027 mm/year v. 0.051 ± 0.022 mm/year, p = 0.006).
Although there have been a number of reports evaluating the wear resistance of highly crosslinked polyethylene at short-to mid-term follow-up,3–11 there have been few reports exceeding 10 years’ implantation time and even fewer that were part of a prospective, randomized controlled trial. The purpose of the present study was to evaluate wear for first-generation highly crosslinked polyethylene at a minimum of 13 years’ implantation, updating our previous report at a longer term follow-up.
Methods
Patients who had been enrolled in the prospective randomized controlled trial were eligible for inclusion. We reviewed charts to identify cases of revision or death. We attempted to contact all other patients to determine the status of their hip and, where possible, schedule them for a follow-up visit, including radiographic evaluation.
Patient recruitment for the long-term follow-up was extremely challenging owing to the age of the patients. After recruiting 16 patients — 8 in each polyethylene group — we performed a post hoc power calculation based on the measured total head penetration. We determined that we had sufficient power (81.6%) to measure a significant difference with an α of 0.05 and elected to stop recruiting patients to the clinic for wear measurement. Our institutional review board approved the study, and all participants provided informed consent.
At the time of the latest follow-up, patients completed the clinical outcome scores from the original study: the HHS, WOMAC and SF-12. Each patient also underwent conventional radiographic imaging. We reviewed the anteroposterior and lateral view images for signs of osteolysis. The presence of lesions (if any) was noted.
Femoral head penetration due to wear was measured by radiostereometric analysis (RSA), using the validated centre index method.12 Patients underwent a standard supine RSA examination with simultaneous, bilateral calibrated radiograph exposures. The 3-dimensional difference between the current location of the femoral head and the original location of the femoral head (at the time of the index procedure, before any wear occurred) was calculated as the total femoral head penetration. We calculated the femoral head penetration rate on a per-patient basis by dividing the total femoral head penetration by the implantation time.
Statistical analysis
We used t tests to compare demographic data, clinical outcome scores and wear measurements between the groups. We considered results to be significant at p < 0.05 for all statistical tests.
Funding
No external source of funding was received for this follow-up study. Financial support for the original study was provided by Zimmer Inc., to support the salaries of a research nurse (who enrolled patients and gathered outcome data) and a research technician (who performed the radiographic wear analysis).
Results
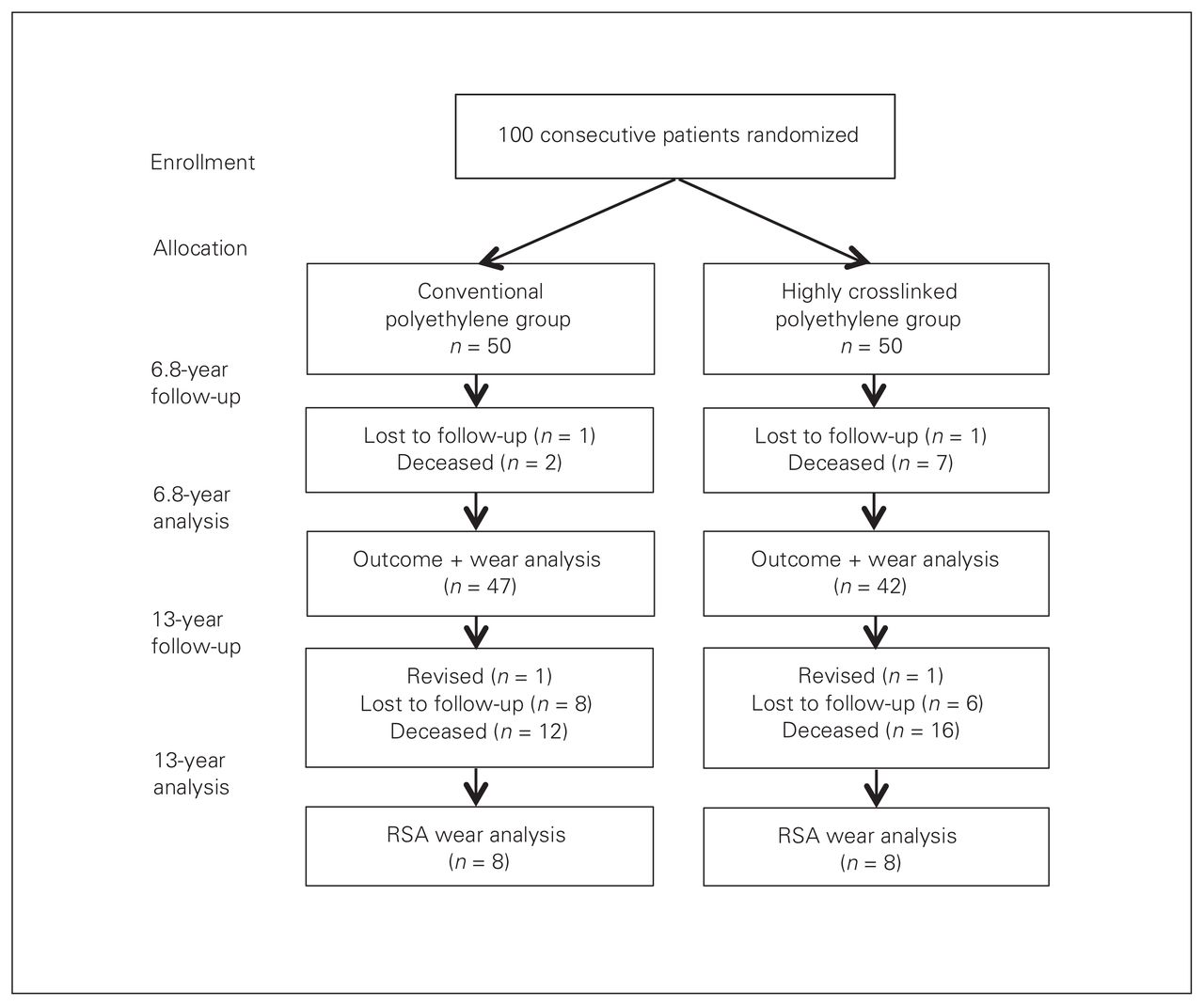
After a minimum of 13 years, 29 patients from the original study had died, and 14 patients were lost to follow-up. This left 57 patients eligible for follow-up, and of these 2 patients were revised and 55 patients were alive without revision (Fig. 1). One revision occurred in each of the conventional and highly crosslinked polyethylene groups. In both revision cases, the reason for revision was loosening of the femoral stem. The revised patient in the conventional polyethylene group was a woman whose impant was revised at 5.5 years, and the patient in the highly crosslinked group was a man whose implant was revised at 6.5 years. Among the 16 patients who returned to clinic for RSA wear measurement after 13 years, we observed no differences in any demographic characteristics between the conventional and highly crosslinked polyethylene groups. There were 2 men and 6 women in the conventional polyethylene group, and 1 man and 7 women in the highly crosslinked polyethylene group. The mean duration since implantation was 13.6 years (range 13–15 years, p = 0.89 between groups). The mean age at the time of the procedure was 67.5 years (range 56–77 years, p = 0.85 between groups), which was younger than that of the full original cohort of 100 patients (mean 72 years). The mean BMI was 28.4 (range 23–35, p = 0.24 between groups).

Patient recruitment, allocation and follow-up. RSA = radiostereometric analysis.
Femoral head penetration was on average 58% greater in the conventional polyethylene group (p = 0.013). The total femoral head penetration (Fig. 2) in the conventional polyethylene group was 1.046 mm (range 0.549–1.428 mm) and 0.622 mm (range 0.361–1.037 mm) in the highly crosslinked polyethylene group. Converted to a yearly penetration rate (which included the bedding-in period), the rate was again twice as high in the conventional polyethylene group (p = 0.007). The penetration rate (Fig. 3) was 0.077 mm/year (range 0.040–0.106 mm/year) in the conventional polyethylene group and 0.042 mm/year (range 0.027–0.079 mm/year) in the highly crosslinked polyethylene group.

Total femoral head penetration (in millimetres). The grey zone extends from the lowest amount of conventional polyethylene head penetration to the highest amount of highly crosslinked polyethylene head penetration, demonstrating overlap between the 2 groups.

Femoral head penetration rate (in millimetres per year). The grey zone extends from the lowest amount of conventional polyethylene head penetration to the highest amount of highly crosslinked polyethylene head penetration, demonstrating overlap between the 2 groups.
The presence of osteolysis was noted in only 1 patient, who was in the conventional polyethylene group. The patient was a man aged 55.6 years at the time of the procedure, with a BMI of 24.9. His RSA examination at 13.7 years revealed a total femoral head penetration of 1.4 mm, for a wear rate of 0.104 mm/year. The osteolytic lesion was noted surrounding the acetabular cup.
There was no difference in the HHS, WOMAC, or SF-12 clinical outcome scores between the highly crosslinked and conventional polyethylene patients who returned for RSA wear analysis (Table 1). There was also no difference in the clinical outcomes scores between the highly crosslinked and conventional polyethylene patients who had returned to clinic between 7 and 13 years after the index procedure but who were not available for the RSA wear analysis (Table 2).
Clinical outcome scores for patients with a latest follow-up of at least 13 years
Clinical outcome scores for patients with a latest follow-up of at least 7 years (therefore exceeding the previous follow-up report)
Discussion
A large number of patients were deceased or lost to follow-up at 13 years. This is a result of the original inclusion criteria for the trial, which preferentially selected older patients owing to concerns surrounding the longevity of the then new crosslinked polyethylene material. The patients who did return at 13 years were all among the youngest patients enrolled in the original study, with a mean age of 65 years at the time of the procedure versus 72 years for the overall group. Other patients who were not lost to follow-up or deceased, but who did not return for the 13-year follow-up, tended to be the oldest patients and were unable or unwilling to come back to the clinic.
There was no difference in clinical outcomes or survival between the conventional and highly crosslinked polyethylene groups. This may be in part because of the selection of older patients at the time of the index procedure, as these patients are likely to be less demanding of their implant. The average wear rate in the conventional group was well below the osteolysis threshold.13 The majority of studies reporting on survival at 5 or more years have found no difference between conventional and highly crosslinked polyethylene, as was the case in the present study.9 Other studies have found a greater revision rate in the conventional polyethylene group.4 The most recent report of the Australian Orthopaedic Association National Joint Replacement Registry (2014) has 13-year data, reporting a 9.0% revision rate for metal on conventional polyethylene and a 4.6% revision rate for metal on highly crosslinked polyethylene.14 Therefore the results of the present study may be applicable only to this implant and to the elderly patient population studied.
Most notably, polyethylene wear was significantly different between the 2 groups. The conventional group demonstrated twice the total femoral head penetration and femoral head penetration rate of the highly crosslinked group. The better performance by highly crosslinked polyethylene is consistent with virtually all other studies of wear in hip arthroplasty at mid to long-term follow-up. The femoral head penetration rate for highly crosslinked polyethylene in this study (mean of 0.042 mm/year, including the beddingin period) falls within the middle of the range of previously reported wear rates and is in fact exactly the same as the average found in a systematic review of 28 studies of first-generation highly crosslinked polyethylene.1,3,9 The average rates for both highly crosslinked and conventional polyethylene in this study fell below the commonly accepted osteolysis threshold of 0.100 mm/year. Only 1 patient showed any signs of osteolysis: a patient with a conventional polyethylene implant and a mean wear rate just above the osteolysis threshold at 0.104 mm/year.
Limitations
The primary limitation of this study is that only 16 patients returned to clinic for complete RSA wear analysis at 13 year; however, this number provided adequate statistical power to detect a significant difference. As described earlier, the number of patients still living and available for follow-up was related to the original study design, in which older patients were preferentially included in the trial. The difficulty of bringing back patients for long-term follow-up is well understood. Acknowledging the limitations with respect to radiographic follow-up, we were able to account for 86 of the 100 enrolled patients, with 14 patients lost to follow-up. This is one of the very few prospective randomized trials reporting long-term follow-up on highly crosslinked polyethylene.
Conclusion
Like most institutions, ours has entirely switched to the use of highly crosslinked polyethylene for total hip arthroplasty. This first-generation highly crosslinked polyethylene appears to continue to do well at 13 years, with half of the femoral head penetration rate as conventional polyethylene. Though survival is currently equivalent between the 2 groups in this study (with 1 revision per group), this has not been the case when comparing the long-term results between other cohorts of conventional and highly crosslinked polyethylene groups at more than 10 years’ follow-up treated at our institution.15 The hope would be that the decreased wear rate in this highly crosslinked group could potentially translate to increased longevity in the second and third decade after surgery.
Footnotes
Competing interests: S. MacDonald reports royalties, consultant fees and research support from DePuy, A Johnson & Johnson Company; stock options from Hip Innovations Technology and JointVue; and research support from Smith & Nephew and Stryker. R. McCalden reports consultant and speaker fees from Smith & Nephew and research support from Smith & Nephew, Johnson & Johnson, Depuy and Stryker. D. Naudie reports financial or material support from DePuy, A Johnson & Johnson Company; royalties, financial or material support, speaker fees, and consultant fees from Smith & Nephew; and financial or material support, consultant fees and speaker fees from Stryker. No other competing interests declared.
Contributors: M. Teeter, S. MacDonald, R. McCalden and D. Naudie designed the study. M. Teeter, X. Yuan and L. Somerville acquired and analyzed the data. M. Teeter wrote the article, which all authors reviewed and approved for publication.
- Accepted December 2, 2016.
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.