


Abstract
Background: The role of physician assistants (PAs) in surgical care in Canada is expanding. Similarly, the acute care surgery (ACS) model continues to evolve, and PAs are increasingly being considered as members of ACS teams. However, their exact impact and contribution has not been well studied. Our study describes the contribution of a PA who worked full time on weekdays on an ACS team in a Canadian academic tertiary hospital.
Methods: To quantify the PA’s contributions, an ACS database was created in September 2016. Data on the number of ACS patient encounters, the number of ACS surgical consults, the number of ACS admissions, the PA’s involvement in the operating room, the number of PA patient encounters and the number of multidisciplinary meetings were prospectively collected. We report data for 365 consecutive days from Dec. 30, 2016, to Dec. 29, 2017.
Results: The ACS team had 11 651 patient encounters during the year, with a mean of 31.92 per day. The mean number of surgical consults per day was 5.89, and a mean of 2.08 surgical procedures were performed per day. The PA was involved in 53.5% of all patient encounters, despite working only during daytime hours on weekdays. Multidisciplinary meetings were conducted by the PA 94.9% of the time. Alternate level of care patients were seen by the PA 96.2% of the time. The PA was directly involved in 2.0% of the operating room procedures during the study period.
Conclusion: Integrating a PA on an ACS team adds value to patient care by providing consistency and efficient management of ward issues and patient care plans, including multidisciplinary discharge planning, timely emergency department consultations and effective organization of the ACS team members.
The physician assistant (PA) role has been well established in the United States since the 1960s; however, it is a relatively new position in Canadian health care. The Canadian PA role initially emerged within the military in 1984.1 The first PA civilian training programs were established in 2008 at McMaster University and the University of Manitoba. Since then, an additional program has been developed at the University of Toronto. In the US, more than 100 000 PAs practise in virtually every aspect of medicine,1 including family practice, emergency medicine, internal medicine, orthopedics, pediatrics, oncology, neurosurgery and general surgery.2 This contrasts with the Canadian context, where the approximately 500 practising Canadian PAs are mainly working in primary care and emergency medicine and only more recently have started working in surgical specialties.1
Although PA training programs are accredited and PAs undergo a national certification process, PAs in Ontario are currently unregulated. The Canadian Association of Physician Assistants (CAPA) states, “The PA’s scope of practice is determined on an individual basis and formally outlined in a practice contract or agreement between the supervising physician(s), the PA and often the facility or service where the PA will work. …The PA’s activities may include conducting patient interviews, histories, physical examinations; performing selected diagnostic and therapeutic interventions; providing medical orders and prescriptions; and counselling on preventive health care.”1
Signing of medical orders and prescriptions by PAs falls within the scope of practice outlined by CAPA. However, as with all patient care provided by PAs, supervising physician(s) must authorize the PA to provide controlled acts that the physician is authorized to perform, including provision of medical orders and prescriptions, via delegation. 3 Medical orders and prescriptions delegated through a medical directive may be signed by a PA, with the exception of orders for prescriptions for narcotics, controlled drugs or targeted substances.4
There is a drive to increase the number of PAs practising in Canada. This has been stimulated by the restrictions imposed on resident duty hours and the resulting unmet needs of the health care system. Some studies have examined the combined effects of PAs and nurse practitioners (NPs) on the deficit produced by the reduction in resident duty hours; PAs and NPs are referred to interchangeably as physician extenders,5 nonphysician practitioners,6,7 advanced practice providers8 or mid-level providers.9
Study results unanimously agree that the addition of physician extenders to the health care team reduces resident workload.5–9 A recent systematic review also found that the addition of PAs and NPs decreased patient length of stay and resident workload, while increasing resident sleep time and improving resident operating time.5 Surveys in the surgical setting indicate that most residents report spending less time on administrative and noneducational tasks, with no impact on their opportunities to perform key aspects of cases in the operating room.5,8 The addition of PAs and/or NPs has been shown to be positive overall, and residents have indicated that the addition of more PAs and/or NPs would enhance their training experience.8 Canadian studies have found that in certain roles, PAs can save their supervising physicians up to 200 hours of work per year.10 Furthermore, they have contributed to increases in surgical throughput, reductions in time to in-hospital consultation, decreases in hospital length of stay, reductions in resident workload, decreases in the number of late hospital discharges, reductions in wait times, a 50% reduction in the number of patients not seen in the emergency department, and increases in surgical productivity by more than 35%.10–14
The acute care surgery (ACS) model has emerged in the last decade as a means of addressing the care of emergency general surgery (EGS) patients who require complex, timely and often multidisciplinary care.15 The ACS service, because of patient volumes, the acuity and complexity of patient needs and a rotating roster of surgeons, requires greater capacity and stability to succeed. The addition of physician extenders, such as PAs, can improve patient care as well as provide the support required by staff surgeons and allied health members, which is increasingly compromised because of resident shortages. In addition, physician extenders can facilitate multidisciplinary conferences, provide timely responses to acutely ill patients, coordinate with other services and facilitate patient flow.
This study focuses on the emergence of the PA role on an ACS team in a Canadian academic tertiary care hospital. It also provides a method of quantifying the involvement of the PA in a particular health care setting, which may be used to support the emergence of the PA role throughout the Canadian health care system.
Methods
Establishment of the physician assistant role on an acute care surgery service
The ACS service at St. Joseph’s Healthcare Hamilton (Charlton Campus), an academic tertiary care centre in Hamilton, Ontario, affiliated with McMaster University, was established in 2012. The ACS team is responsible for the care of all patients undergoing nonelective surgery, including performing consultations in the emergency department for surgical patients, conducting daily ward rounds on all ACS patients and completing urgent and emergency procedures as needed. The PA role was implemented on the ACS team in November 2014 and was occupied by the same PA (A.L.) until September 2019.
The ACS team comprises several team members who rotate on the service. It is always overseen by a staff surgeon, but other team members vary on the basis of the availability of surgical residents. This variability has increased in recent years. Clinical clerks and PA students can be part of the ACS team. The staff surgeon is responsible for the ACS team 24 hours a day, 7 days a week, for 1-week blocks (with the exception of 2 overnight, 14-hour “relief” periods). The staff surgeon takes over the team on Friday mornings at 7 am and hands over to the next staff surgeon at 7 am the following Friday. There is no dedicated daytime operating time available to the ACS service, but emergent cases are placed on the emergency list available to all surgical services. Residents typically rotate on the team for 1- or 2-month blocks. Clerks who rotate through the service are usually part of the team for 2 weeks. Because of the constant rotation of staff, residents and students, as well as gaps in resident coverage, we felt that it was imperative to have a constant team member to help improve continuity of patient care. Given the frequent changes in other team members, the PA emerged as a point person for communication with other staff and departments. Efforts were also made to increase the research agenda of the ACS team after implementation of the PA role and the hiring of an ACS-focused surgeon in 2016.
At the time of our study, the PA worked daytime hours from 7 am to 3 pm on Monday, Tuesday and Thursday, from 7 am to 5:30 pm on Wednesday (to participate in resident teaching rounds and morbidity and mortality rounds) and from 7 am to 12:30 pm on Fridays. The PA was a consistent member of the ACS team and did not rotate. The PA had medical directives that allowed for autonomous but supported completion of clinical and medical orders. The role of the PA changed over time on the basis of the needs of the ACS service and the development of medical directives. For example, the PA was initially involved in more operating room procedures; however, it was found to be more effective for the team to have her focusing on consults and ward work.
Database development
The role of the PA on the ACS team continuously adapted to the needs of the team and ACS inpatients. To quantify the involvement of the PA, we created an ACS database in September 2016. We report data for 1 year of the PA service, from Dec. 30, 2016, to Dec. 29, 2017. We chose this period because data collection methods were refined after the initial few months of data were analyzed.
The following data were collected daily: total number of ACS patients, total number of consults (day and night), total number of admissions, total number of operating room procedures, total number of patient encounters and total number of PA patient encounters. Data on the total number of multidisciplinary meetings and the care of alternate level of care (ALC) patients (patients with lengthy hospital stays) were collected during weekday daytime hours. The data were collected daily by the PA and supplemented by information from the residents on the ACS team for a total of 365 consecutive days. The on-call resident was responsible for collecting data at night and relaying it to the PA at morning handover. Weekend data collection was done by the junior resident on call. All data were entered into a database by the PA. A patient encounter was defined as a patient seen on rounds, an operation or a consult. For example, if on a given day there were 20 ACS patients, with 2 operating room procedures and 3 consults, the total number of ACS patient encounters that day would be 25. Multidisciplinary meetings (typically held twice weekly, on weekdays) were held with allied health providers and focused on communicating care plans and disposition planning. Allied health providers included the nursing manager, charge nurse, social worker, occupational therapist, physiotherapist, dietitian and pharmacist. The meetings were led by the PA, and ACS surgical patients were discussed at these meetings.
Results
The ACS team was responsible for a mean of 31.92 patient encounters per day, with a total of 11 651 patient encounters in the 1-year study period (Table 1). The mean number of surgical consults per day was 5.89. The mean number of operating room procedures performed each week was 14.63, with a daily mean of 2.08 procedures.
Activities performed by the ACS team during the study period
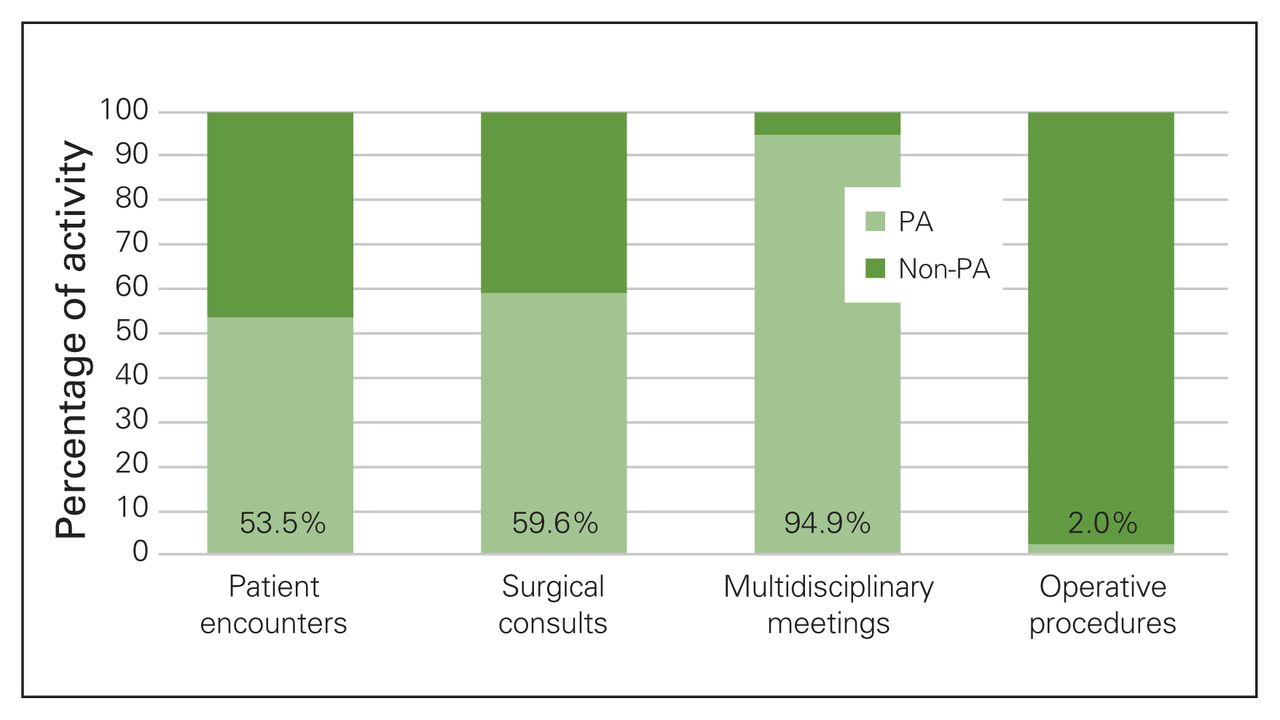
The PA’s working hours, as previously described, equated to 23.8% of the total ACS working hours in a week. During the study period, the PA worked 22.4% of the working hours, when statutory holidays and vacation are taken into account. Despite this, the PA was directly involved in 6231 patient encounters (Table 2). This represents 53.5% of the total number of patient encounters (Fig. 1). Multidisciplinary meetings were conducted by the PA 94.9% of the time. Alternate level of care patients were seen by the PA 96.2% of the time. The PA was directly involved in only 2.0% of the total number of operating room procedures during the study period.
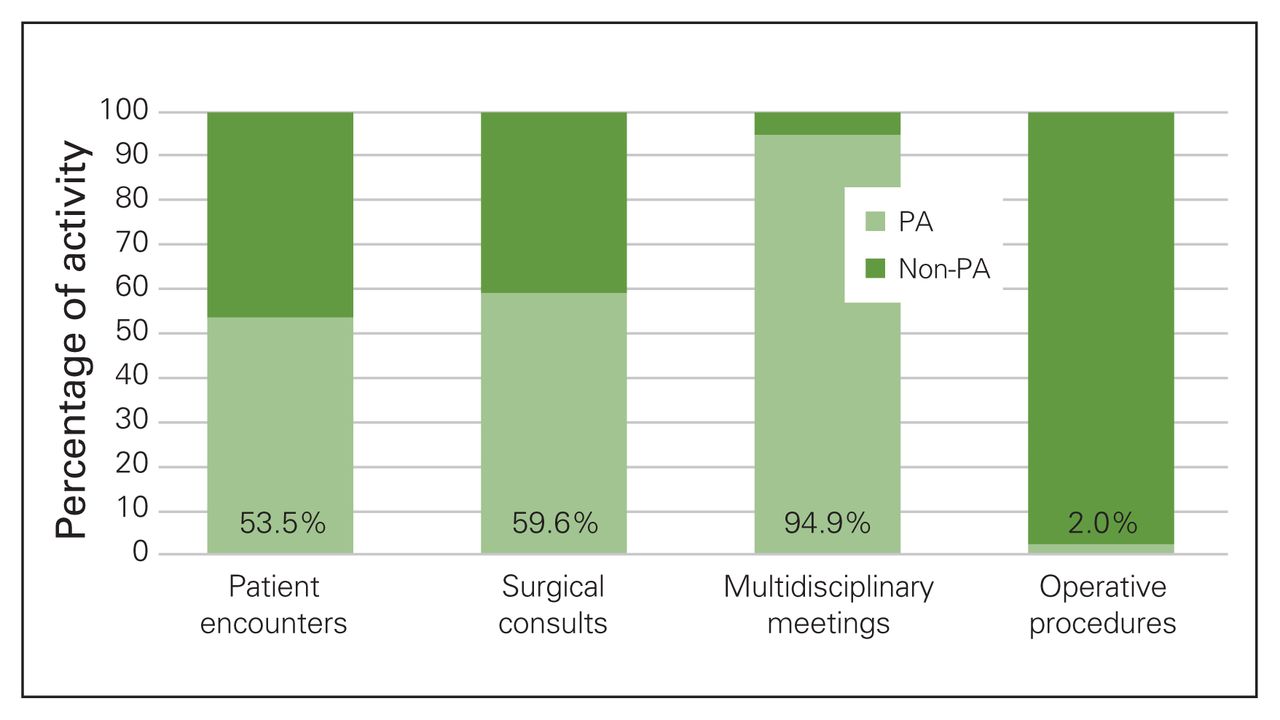
Percentage of activity performed by the physician assistant (PA) compared with other members of the acute care surgery (ACS) team in the 1-year study period. The value reported for multidisciplinary meetings indicates the percentage of ACS-led meetings that were led by the PA. The value reported for operative procedures indicates the percentage of procedures attended by the PA.
Activities performed or attended by the PA in the study period
After the PA joined the ACS team, there was an overall improvement in the satisfaction scores of residents on the ACS rotation, and an improvement in their satisfaction with the balance between service load and the opportunity to achieve their educational objectives and personal learning goals (e.g., time spent in operating room, ability to attend academic half-day). This feedback was received from resident meetings and from in-person discussions with residents after they completed their ACS rotation. Multiple factors may have contributed to this trend in resident evaluation; objective assessment of these factors is warranted in future research. Nonetheless, the contributions of the PA and her impact on residents at our site are highlighted by her receipt of the Resident Award for Excellence following the study period. The resident evaluation system changed over the course of the implementation of the PA role and there were insufficient numerical data available to include in our analysis.
Although the impact of the PA on the satisfaction of patients, staff and allied health providers was not assessed, formal and informal feedback was requested. It was overwhelmingly positive. A registered dietitian stated, “The PA … [is] present throughout patients’ entire admission. The PA is knowledgeable of the patient’s entire medical course and therefore can provide valuable information to help make informed decisions on medical plans, discharge plans and goals of care discussions. The PA is able to act as a strong advocate for patients and family members’ concerns as they have an in-depth understanding of the patients’ medical state, course in hospital, social situation and outstanding issues. The PA is easily accessible on the unit for allied health members to ask questions to, clarify information and overall gain a better insight on the patient and medical plan. Allied health members’ care orders are now signed within a timely manner, making care plans more efficient. For instance, diet orders and tube feed orders are signed quicker allowing patients to receive nutrition faster.”
The charge nurse on the surgical ward, who has been in the role for 11 years, also shared the effects she observed. “Since our PA has come aboard, much of our daily rounding [and] needs of the patient are addressed. … [She] is our ‘go to person’ that we can relay our patient concerns to. If it is not in her scope of practice to make the decision, she will be in contact with her senior to get the issue resolved. This process has proven to be very valuable on our unit. … [The PA]’s role in assisting with discharges has been a HUGE asset, especially in assessing needs for the patients and safely returning them home. At this time I could not imagine working without our PA.”
Discussion
The number of general surgery residents has been decreasing over time.2,16–18 This is because of several factors, including decreasing availability of spots for general surgery trainees at McMaster and nationally, as well as the adoption of work-hour restrictions over the past decade.16–18 In addition, off-service resident programs that previously required general surgery rotations are opting not to participate in general surgery rotations, possibly as a result of the move toward more specialized training and the shift toward competency-based training.
Owing to the dwindling number of available residents, coverage of the ACS service at our site is not consistent. Physician extenders, such as PAs, have been suggested as candidates to address such shortages.2,19,20 Physician extenders have been found to reduce the workload of surgery house staff and improve patient care.2,5,8 Our experience, as demonstrated in this study, has been consistent with these findings. Compared with NPs, who are trained in the nursing model using a patient-centred approach, PAs are educated in the medical model using a disease-centred approach based on the CanMEDS competencies.21,22
The current study assessed the integration and productivity of a PA on an academic ACS service. Integration of the PA at our centre with front-line staff was found to be smooth. Medical directors served as enablers to successful integration. Following the study period, increased experience and clinical exposure allowed the PA to consistently work from 7 am to 3 pm Monday to Friday. The PA worked collaboratively with the ACS team to manage patient cases and complications. As she developed the necessary communication skills through experience, the PA independently led some ALC discussions, with involvement of the staff surgeon for more complex cases. Because she adhered to the Ontario College of Pharmacists’ guidance on PA prescribing through medical directives, the PA at our centre did not experience any pushback for medication orders or from pharmacies receiving her prescriptions.4
Our experience suggests that the PA supports resident learning by providing hospital-specific knowledge to learners, acting as a consistent point of liaison with members of the general surgery faculty and helping residents to navigate relationships with other departments and members of the multidisciplinary team. The PA on the ACS team helped residents to achieve their ACS learning objectives. Residents were frequently involved in the workup and consultation of ACS emergency cases, and residents, particularly those in their first year of training, felt supported by the PA in this process. During daytime operating room procedures, the PA provided coverage of the ACS service, allowing for increased involvement of residents in the operating room. As with staff, the day-to-day role of residents on the ACS service is fluid, and when they are present they are an integral part of the team. During periods with no resident coverage, the PA helped to fill some of these gaps.
It is possible that the addition of a PA teaches residents skills to be used in future practice, such as team building. 7,12 Residents have to establish effective communication lines with the PA and we agree with Dies and colleagues12 that this is a positive contribution to the CanMEDS competencies of communicator and manager.
Available literature suggests that a robust ACS model includes dedicated access to daytime emergency operating room time.23,24 At our site we do not have this access, but in the context of other Canadian programs that do, the addition of a physician extender can contribute to residents’ development of the CanMEDs medical expert competency by allowing them more time to operate. The long-term effects of PAs on resident education have yet to be definitively elucidated in the literature. There is no doubt, however, that given that residents are front-line health care providers, their education and satisfaction is essential to the quality of health care. As such, investments in resident education are important considerations for health care administrators.
The PA at our site identified multiple barriers to her work satisfaction, the most substantial being sustainability of funding for the position. Although patient volumes and workforce challenges with resident shortages make it clear that this type of position is needed, the position was not a hospital salaried position. Funding for the first year of the position was divided equally between the hospital and Health Force Ontario’s PA Career Start grant for employers hiring new PA graduates.25 In future years, the hospital continued to fund half of the PA’s earnings and the other half was funded by the group of general surgeons. The PA was on yearly contracts that were renewed on an annual basis with repeated discussion and negotiations around long-term funding for the position. Consensus on a long-term, salaried funding model would have added stability to the PA position and aided in job satisfaction. A sustainable, long-term funding model would alleviate the most significant barrier to growth of the PA profession in Canada.21,26 As demonstrated by the greater overall success in integrating PAs into the health care system in the US, regulation of PAs in Canada would also increase acceptance of PAs by hospital stakeholders, remove concerns around liability and expand the autonomy of PAs to reflect their level of training.22,27,28
Large variations in ACS patient volumes and workforce also contributed to decreased overall work satisfaction for the PA. The ACS data at our site over 5 years saw the overall ACS patient list vary widely, from 7 to 54 patients. This extreme variability, coupled with decreasing and variable resident coverage, made the management of patient volume challenging and contributed to PA burnout.
The PA on our service resigned from the position almost 5 years after joining the team. The reasons given in the exit interview were multifactorial but highlighted the PA satisfaction issues discussed above. Learning from our experience, and with further decreases in resident manpower, this has led to the addition to our ACS service of 3 hospital-funded positions for physician extenders, currently on annual contracts.
One of the challenges we have faced in building our ACS program is that there are many stakeholders who influence decisions around ACS, including hospital administrators, the multiple surgeons who rotate on the service, residency programs and residents. There has been rapid uptake of ACS services nationally over the past decade; however, it remains unclear what ACS resources and support are appropriate, and these vary widely across the country.
There is a need for much more Canadian research in ACS. Much of this work is being championed by the Canadian Collaborative on Urgent Care Surgery (CANUCS).15,23,29–31 Direction for future studies, particularly at centres introducing physician extenders on their ACS service (PAs, NPs, hospitalists), include objective assessment of the impact on ACS service efficiency and cost-effectiveness, patient outcomes, emergency department disposition times, resident learning, and satisfaction scores for residents, staff and allied health team members. These outcomes should be tracked and collected by a research team member rather than the already overburdened ACS team members (PA, residents, etc.), and work should ideally begin before the introduction of the role.
Centres that are introducing a PA to their ACS team should seek support from medical directors, as this served as an enabling factor at our centre, allowing for greater acceptance of the PA on an administrative level. Ideally, detailed goals and objectives for the position should be laid out from the beginning, although flexibility in the role is vital for its success. Evaluation criteria for PA performance and outcomes should be identified at the outset, and rotation score sheets should be administered to residents before and after the addition of the PA to assess the impact of the addition and to identify areas for improvement. Although it is expected that PAs will build their knowledge and skills with experience, they would be better equipped with formal training upon recruitment, such as participating in a “surgical boot camp” with incoming residents (which exists at several programs) or attending resident surgical foundations teaching sessions.
Limitations
Our study was conducted at a single academic tertiary hospital and our findings therefore have limited generalizability. The results are also limited by the fact that our study involved a single PA, on the specialized ACS service, in a specified time period. Although it is impressive that our PA participated in most multidisciplinary meetings, we echo the note by Kang and colleagues that this activity must be interpreted with caution.8 Resident core competencies outlined in the CanMEDS Framework include interpersonal and communication skills as well as professionalism. Although our PA made a positive contribution by decreasing the workload of residents, they may have missed opportunities to develop administrative, professional and interpersonal skills.
Although data were collected by the PA in a thorough manner during working hours, the task of data collection after hours and on weekends was added to the extensive workload of the surgical residents. To ensure robustness of the data captured during the study period, any missing data were gathered from attending surgeon billing. Although data loss was possible, we believe that the process of data collection and verification was thorough enough that missed data would not be of sufficient magnitude to alter the study results.
This study also reflected some of the clinical and research challenges inherent to ACS. This service is difficult to measure because of the complexity of the patient population and the fact that the ACS service provides care for a combination of operative patients, nonoperative patients and admitted patients awaiting placement in long-term care. This is in addition to the administrative complexities that have given rise to the various ACS models adopted by different hospitals, as well as the fact that multiple surgeons run the service.
Conclusion
The integration of the PA on the ACS team of our busy academic hospital enhanced patient care and consistency of care and was instrumental in addressing care gaps due to resident shortages. Even though she worked only during daytime weekday hours, the PA was directly involved in 53.5% of patient encounters, 96% of encounters with ALC patients and 95% of multidisciplinary meetings. Over time, the role evolved to minimize PA involvement in the operating room in order to maximize resident operative exposure. As she gained experience, the PA was able to effectively manage the ACS team at times when the staff surgeon and surgical residents operated, performed other procedures such as endoscopy or were involved in academic training. With appropriate communication, knowledge of patient plans and medical directives, the PA was able to implement patient health care in a timely manner. This allowed for greater accessibility and consistency of care with less handover. The addition of the PA was an efficient and effective way to improve the ACS surgical service. Further research is required to objectively quantify the impact of a PA on hospital efficiencies, patient satisfaction, staff surgeon and surgical residents’ workload and satisfaction, and resident learning opportunities.
Acknowledgements
The authors thank the following people for their help and support in starting and supporting the ACS PA program at our hospital: Dr. Peter Lovrics (Head of Service, General Surgery, 2003 to 2015), Dr. Margherita Cadeddu (Head of Service, General Surgery, 2015 to present), Dr. David Russell (Chief of Staff, 2018 to present) and Mr. Phillip Valvasori (Manager, Medical Affairs and Patient Relations)
Footnotes
Presented at the Canadian Association of Physician Assistants Conference, Oct. 27–29, 2017, Ottawa, Ont; the Canadian Surgery Forum, Sept. 14–16, 2017; and the American Academy of Physician Assistants Conference, May 15–19, 2017, Las Vegas, Nev.
Competing interests: None declared.
Contributors: A. Lack and R. Nenshi designed the study. A. Lack, S. Lethbridge and R. Nenshi acquired the data, which all authors analyzed. A. Lack, M. Saddik and S. Lethbridge wrote the manuscript, which all authors critically revised. All authors gave approval of the final version for publication.
- Accepted December 16, 2019.
References
In this issue

{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.