


Summary
Competency-based education (CBE) is currently being implemented by the Royal College of Physicians and Surgeons of Canada across all residency programs. This shift away from time-based residency is proposed to be the answer to maximize training opportunity in the era of work hour restrictions and growing concerns regarding accountability in medical education. A Web-based survey was conducted to obtain feedback from Canadian general surgery residents on their experience and perception of competence within core procedures, as well as attitudes toward CBE. A total of 244 residents completed the survey. For most procedures, more than 50% of residents felt they could perform the procedure with no guidance after completing 11–30 cases. Generally, residents were welcoming of CBE; however, medium-sized programs reported some concerns regarding inadequate exposure to cases and risk of training less well-rounded surgeons. This is valuable resident feedback for programs to consider during the implementation process.
Competency-based education (CBE) is currently being implemented by the Royal College of Physicians and Surgeons of Canada (RCPSC), using the Competence By Design (CBD) framework, across all residency programs in Canada. Implementation of CBE curricula presents noteworthy challenges in the specialty of general surgery. These include the need for new technologies and assessment tools, the lack of supportive resources and infrastructure, the reductive nature of assessments, and the wide scope of procedures that residents must be able to perform competently by the time they transition to independent practice.1 Program directors in the United States created a list of 121 procedures that general surgery residents are expected to perform independently upon graduation.2 Of these procedures, residents reported that 83 were performed less than 5 times on average, and 31 were performed less than once during residency training.2 In a Canadian study, 90% of general surgery residents felt comfortable with basic laparoscopic procedures (appendectomy, cholecystectomy) at the end of their training, but only 8% felt comfortable with more advanced procedures, such as laparoscopic right hemicolectomy.3
A Web-based, multicentre, cross-sectional survey was sent to general surgery residents training at all 17 Canadian institutions between June 1 and Aug. 17, 2015, to assess their experience and perception of competence within core procedures as well as their attitudes toward CBE and the current curriculum (Appendix 1, available at canjsurg.ca). Participants were asked to rate their perceived competence in 9 common general surgery operations: laparoscopic appendectomy, elective laparoscopic cholecystectomy, open right hemicolectomy, mastectomy, Hartmann procedure, sentinel lymph node biopsy (SLNB), low anterior resection (LAR), and open and laparoscopic inguinal hernia repair. A de novo 4-point rating scale was proposed; the Perceived Procedural Competence Scale was used to describe the amount of guidance residents felt they needed for each procedure, ranging from needing guidance for most of the procedure to being ready for independent practice.
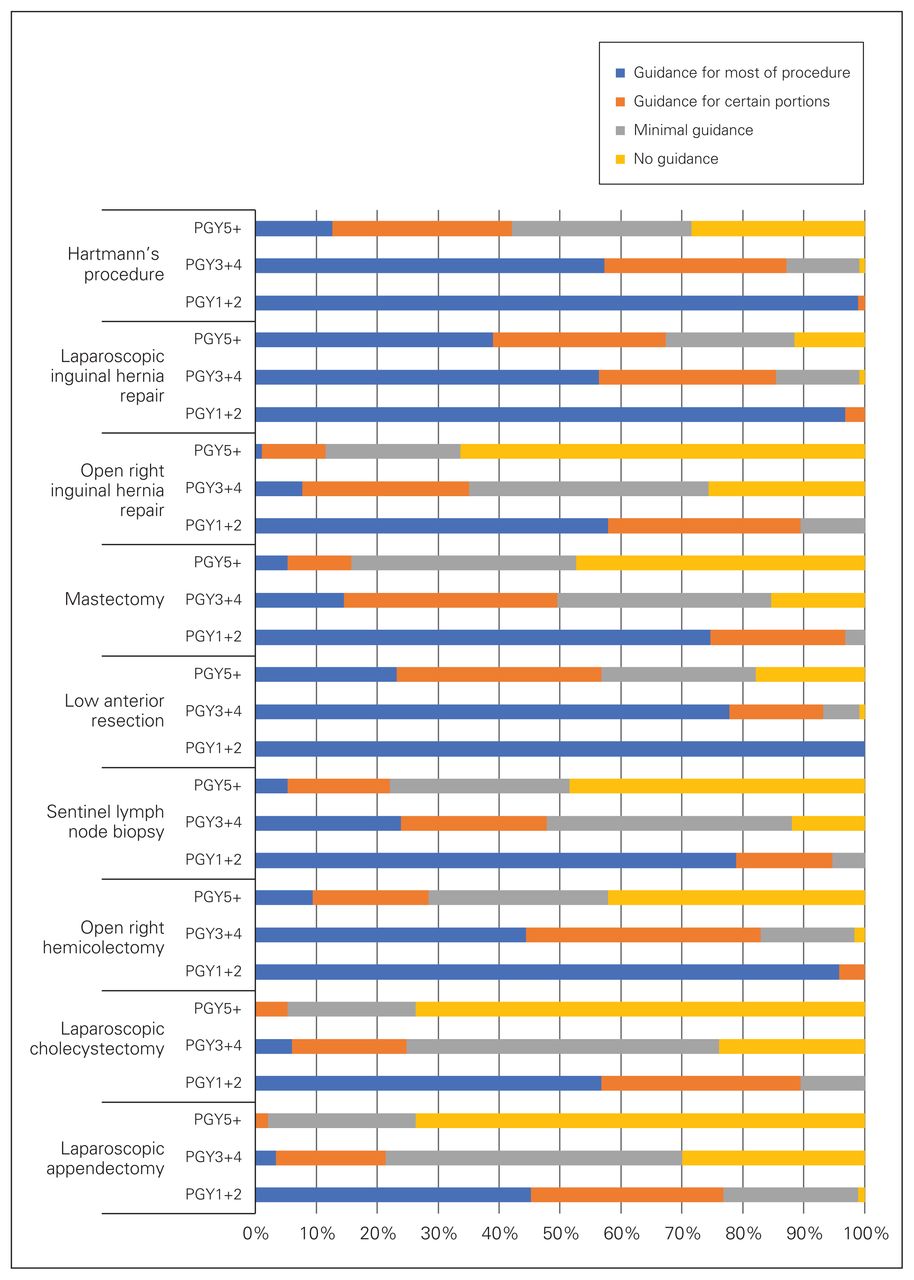
A total of 244 residents completed the entire survey for a response rate of 41.1%. Results showed that laparoscopic appendectomies and cholecystectomies were the procedures that residents reported the most experience performing. Perceived competence for 50% of residents was achieved with 11–30 procedures for elective laparoscopic cholecystectomy, mastectomy, inguinal hernia repair, LAR, laparoscopic inguinal hernia and a right hemicolectomy (Figure 1). Perceived competence was also 11–30 cases for Hartmann procedure, open right hemicolectomy, LAR, and laparoscopic inguinal hernia repair; however, more than 50% of residents completed these procedures fewer than 10 times, indicating that several residents are not meeting case volume numbers where perceived competency is reported. Junior residents (postgraduate year [PGY] 1–2) performed 1–10 cases of laparoscopic appendectomy, laparoscopic cholecystectomy and open inguinal hernia repair. More than 60% of junior residents did not perform any bowel and breast cases. Senior residents (PGY 3–4) and chief residents (PGY5) completed 31–50 cases of laparoscopic appendectomy, laparoscopic cholecystectomy and open inguinal hernia repairs. Senior and chief residents reported performing 1–10 cases of right hemicolectomy, Hartmann procedure, LAR, mastectomy, SLNB, and laparoscopic inguinal hernia.

Resident-perceived competence for 9 common general surgery procedures. PGY = postgraduate year.
Compared with junior residents, chief residents reported that quantifying the number of performed procedures is not an adequate measure of competency. With CBE, each resident will need to demonstrate competence in specific procedures before transition to independent practice. This will potentially eliminate some of the variability in exposure to the breath of surgical procedures by different residents.
Large programs (> 37 residents) were most in favour of implementation of CBE, whereas medium-sized programs (26–36 residents) were most concerned about risk of training less well-rounded surgeons and poor exposure to cases. This concern may arise from the fact that medium-sized programs reported being the most satisfied with their current curriculum. Compared with participants in larger programs, those in small programs (< 25 residents) felt that their academic half-days did not have clear objectives and did not provide essential information. Residents from small and large programs also reported there were too many noneducational activities. Addressing these concerns could ease resident fears about CBE implementation and help frame this transition in a positive light. During their CBE implementation in orthopedic surgery, the University of Toronto prioritized reducing repetitive activities and placing more focus on educational activities relating to residents’ milestones, which was well received.4
Numerous evaluation and assessment methods are currently used by residency programs to track resident progress. In Canada, the main standardized performance evaluations for general surgery residents are the Interim Evaluation Reports (ITER) and the Final In-Training Evaluation Report (FITER)/Comprehensive Competency Report (CCR). A recent Canadian publication outlined the lack of assessment methods for specific general surgery skills such as endoscopy.5 In our survey, residents did not think their assessments were informing them of their competency, and they felt that a greater number of assessments in the operating room would be beneficial. Seventy-five per cent of participants believed they would not be able to finish their residency in less than 5 years. Eighty-seven per cent were receptive to taking the RCPSC exam in their fourth year of residency, allowing their last year to be rich in hands-on experience to facilitate a smoother transition to practice. When asked about the importance of written exams, chief residents rated them as less important than the junior residents. Senior residents provided a significantly higher rating than junior residents with regards to the importance of having assessors in the operating room, observing cases performed by residents.
Conclusion
The implementation of CBE introduces an opportunity to improve assessments and inform faculty of the needs of learners. In a CBE program, formative assessments of resident performance are completed multiple times per week and include assessments of performance in the operating room. However, 2 of the perceived barriers to frequent assessments include faculty buy-in and assessment burnout.1 Broad support from staff and consensus regarding definitions of competency for each procedure will be needed and have been shown to facilitate faculty engagement during transitioning to CBE.4 Postimplementation, it would be pertinent to evaluate how attitudes toward the CBE curriculum have changed and whether residents are satisfied with the new assessment methods.
Footnotes
This paper was presented at the Canadian Surgery Forum.
Funding: The study was funded internally by the Department of Surgery, Queen’s University.
Competing interests: None declared.
Contributors: All authors contributed substantially to the conception, writing and revision of this article and approved the final version for publication.
- Accepted November 5, 2020.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
In this issue

{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.