


Abstract
Four-dimensional computed tomography (4DCT), or dynamic CT, is an emerging modality with a wealth of orthopedic applications for both clinical practice and research. This technology creates CT volumes of a moving structure at multiple time points to depict real-time motion. Recent advances in acquisition technology and reduction in radiation dosage have allowed for increased adoption of the modality and have made imaging of joint motion feasible and safe. Musculoskeletal 4DCT has been used primarily to investigate wrist motion; however, the utility of 4DCT has been shown in other areas, including the shoulder, elbow, hip, knee and ankle. Imaging these joints through a full range of motion provides new insight into dynamic phenomena such as instability, impingement and joint kinematics. Although 4DCT has not yet been widely adopted in orthopedic practice and research, future use has the potential to enable a deeper understanding of musculoskeletal conditions and to improve patient care.
Computed tomography (CT) has advanced substantially since its introduction in the 1970s. The first CT scanners had limited resolution (matrix size 80 × 80), higher radiation (17 mSv for a 6-slice CT head), and time-consuming scanning and processing times (35 min).1 However, improvements in hardware and imaging-processing techniques have led to the ubiquitous use of CT in the medical field, including musculoskeletal health. Reduced ionizing radiation dosage, rapid image-acquisition speeds and vastly improved image resolution have made CT the gold standard for diagnosis and treatment planning in many musculoskeletal conditions.2 Multirow detector CT, introduced in 1999, allowed the capture of multiple image slices at once through the use of adjacent detector rows along the gantry axis to detect a single radiographic source.3 The gantry could complete a full rotation in 0.8 seconds, and the field of view was 20 mm along the axis of rotation. Gradual improvements in the technology reduced the time required for gantry rotation and increased the number of detector rows from 4 to 320.4 These modern scanners can image a 160-mm field of view along the axis of rotation in less than 0.3 seconds, and further improvements are ongoing.5
Development of 4-dimensional computed tomography
With the introduction of wide field of view detector arrays and ultrafast gantry rotation, the use of 4-dimensional CT (4DCT), also known as dynamic CT or kinematic CT, has increased over the last decade. By repeating the acquisition of the same volume with a single gantry rotation at multiple time points, a kinematic volume is created of the patient’s position at each time point. This process is depicted in Video 1 (available online at https://youtu.be/Zu470Xe0hAY). Although the dynamic technique has been technically possible since the advent of multirow detector CT, small fields of view made it impractical. Furthermore, slower gantry rotations made the images subject to motion artifact, and higher radiation dosages made the practice unsafe for human participants. Recent techniques allow clinicians and researchers to capture large volumes in real time, with radiation exposure below that of routine chest radiography, depending on the anatomic region and acquisition protocol.6,7
Nonmusculoskeletal applications
Some of the first applications of 4DCT were in radiation oncology, especially for thoracic and abdominal tumours, where lesions are shown to move with respiration. Quantifying this motion with 4DCT can allow for precise delivery of therapeutic radiation to the lesion.8 Four-dimensional CT can also evaluate dynamic structures such as the heart by imaging the entire heart through the cardiac cycle to investigate flow and valvular disease, and may be of utility in cases in which echocardiography is technically challenging or for patients with magnetic resonance imaging (MRI) contraindications.9 Vascular disease has been investigated with 4DCT and has provided more information than conventional CT angiography, including the response of aneurysms to the cardiac cycle, giving new insight into disease progression risk.10 With an increasing body of evidence for the safety and utility of 4DCT in these fields, the technology is being adopted more widely.11 Clinicians and researchers are realizing that 4DCT provides insight into dynamic phenomena not previously possible to image.
Musculoskeletal applications
In the musculoskeletal field, questions regarding joint kinematics, instability and impingement have all been addressed with 4DCT.
Shoulder girdle
Four-dimensional CT has been used to image the sternoclavicular and acromioclavicular joints, as well as scapulothoracic motion in order to investigate shoulder instability and impingement. In the sternoclavicular joint, Hislop-Jambrich and colleagues12 described visualization of translation of the medial clavicle posteriorly to abut the trachea with arm range of motion in a patient who experienced an intermittent choking sensation. Four-dimensional CT revealed this compression, which was not evident on conventional CT or MRI, which led to the decision to perform surgical stabilization, with a good outcome. 4DCT has also been used as a diagnostic tool to measure the degree of sternoclavicular joint instability based on translation during arm range of motion.13 This information was used to recommend surgical versus conservative treatment with successful outcomes.13
The acromioclavicular joint has also been imaged dynamically. Dyer and colleagues14 reported that cases of persistent pain with seemingly low-grade injuries could be attributed to unexpectedly large translations with glenohumeral joint range of motion, giving a more accurate prognosis for functional impairment with and without reconstructive surgery of the joint. Four-dimensional CT has provided normative data on uninjured acromioclavicular joint motion and has also been able to detect pathologic motion in patients with uncertain diagnosis, such as instability versus arthrosis, on conventional CT.14,15
Clinicians have also used 4DCT to investigate snapping scapula syndrome. In the case of impingement of the scapula on the posterior ribs, preoperative 4DCT has allowed clinicians to determine the precise point of impingement to minimize unnecessary bone resection and to ensure the site of pathology is addressed.16
These clinical applications of 4DCT improved diagnosis and prognostication, and informed surgical planning throughout the shoulder girdle.
Elbow
To our knowledge, there is only 1 study investigating the elbow with 4DCT. Goh and Lau17 used 4DCT to image the ulnohumeral joint. The technology showed impingement of osteophytes on the coronoid process and olecranon, preventing both terminal flexion and terminal extension. These findings highlight the advantage 4DCT has over conventional CT to confirm restrictions in motion due to impingement, rather than capsular fibrosis or adhesions, as is common after elbow injuries. As the technology evolves, further 4DCT investigations are warranted in the elbow.
Hand and wrist
Carpal motion has been investigated with 4DCT in numerous studies. Given that subtle changes can be responsible for functional limitations and severe symptoms, standard imaging methods including MRI often lack the required sensitivity for diagnosis.18 Normal carpal kinematics and postsurgical changes have been described.18–20 Figure 1 shows the use of 4DCT to quantify motion at the trapeziometacarpal joint with thumb flexion. The entire sequence is depicted in Video 2 (available online at https://youtu.be/GY01x01RnXg). Mechanical symptoms (including the catching or clunking seen in trigger lunate syndrome) and instability (such as in scapholunate instability) have also been identified on 4DCT.21–24 In these conditions, the mechanical cause of symptoms was detected only on dynamic imaging, without which appropriate treatment is challenging. The complexity of the carpal joints, coupled with the small field of view required and minimal radiosensitivity, make wrist disorders an ideal application for 4DCT, and clinical indications for 4DCT continue to expand and evolve.
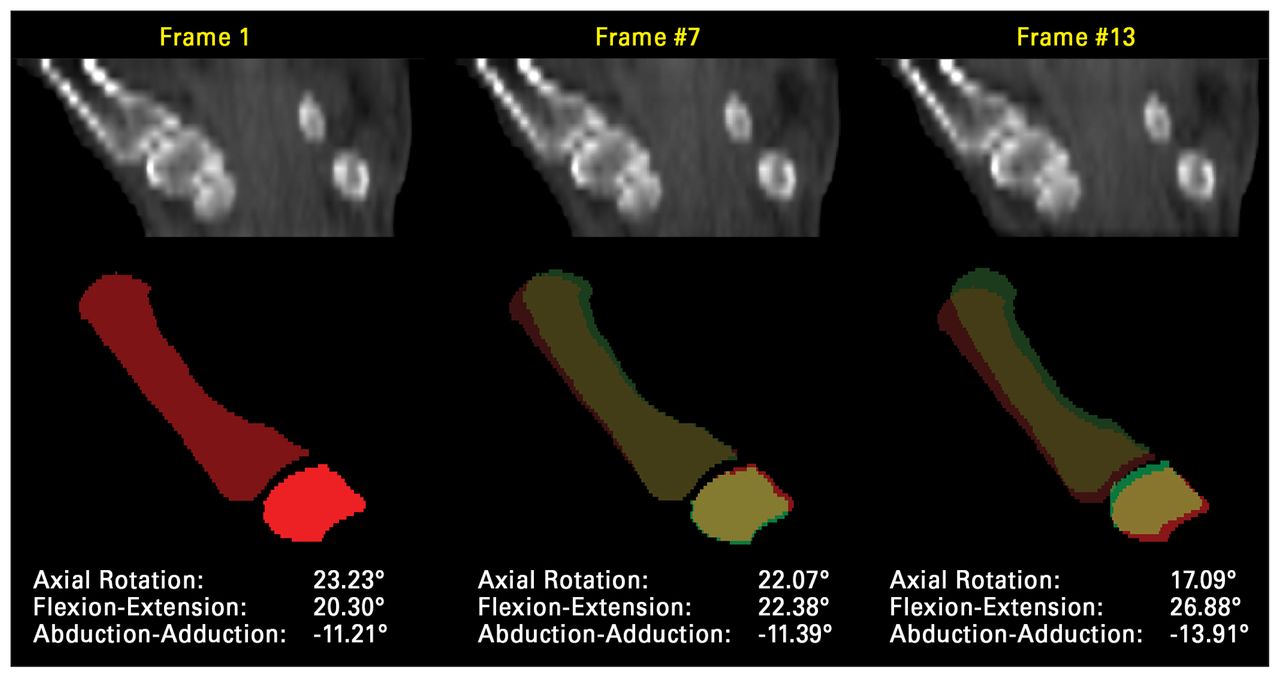
Coronal 4-dimensional computed tomography (4DCT) images showing relative position of the trapeziometacarpal joint at 3 positions of progressive thumb adduction. Three-dimensional bony models can be registered to 4DCT volumes to quantify changes in relative positions during motion.
Hip
There has been limited 4DCT examination of the hip joint, in part owing to the high effective radiation dosage from proximity to radiosensitive tissues and higher energy required for radiologic exposure.2,25 However, Wassilew and colleagues25 investigated femoroacetabular impingement and found that 4DCT predicted the location of cam and pincer–type impingement on the femur and acetabulum more accurately than traditional radiography or MRI, when compared to gold-standard surgical hip dislocation. These findings show the benefits of 4DCT to allow surgeons to accurately plan minimally invasive interventions to remove the sites of impingement via hip arthroscopy, thus minimizing arthroscopy times and morbidity while improving localization of the required resection. Further use of 4DCT for understanding hip disorders should follow as newer image-reconstruction methods and hardware are developed to reduce radiation exposure to the patient.
Knee
Several investigators have developed 4DCT acquisition protocols to analyze patellar tracking through knee range of motion to investigate patellofemoral pain syndrome and the nebulous cause of patellar maltracking and subluxation.26–28 Four-dimensional CT is well suited to investigate patellar tracking though knee range of motion in this patient population. Tanaka and colleagues29 reported that the tibial tubercle–trochlear groove distance varied significantly with the knee flexion angle, which was nonuniform on conventional imaging. Their results showed that 70% of symptomatic patients would qualify for tibial tubercle osteotomy with the knee flexed to 30° based on accepted tibial tubercle– trochlear groove thresholds, versus only 24% of patients with the knee flexed at 0°. With dynamic imaging, quantitative and repeatable measures of instability and maltracking are possible, which help to identify the cause of patellofemoral pain, stratify patients and select surgical candidates.28–31
Foot and ankle
Several investigators have quantified subtalar joint motion, and recent work has expanded into the distal tibiofibular joint. In the subtalar joint, 4DCT has shown motion changes between healthy ankles and those with chronic instability symptoms or stiffness.32 Dynamic imaging of the subtalar joint with the application of external stress throughout a range of motion gives an objective measure of the cause of instability.32 Four-dimensional CT can also measure patient response to therapy, and motion patterns can be linked to specific injury patterns for precise treatment.33 Motion at the distal tibiofibular joint, or syndesmosis, has also been reliably quantified with 4DCT.34 Figure 2 shows physiologic changes in syndesmotic distances with ankle range of motion, which are important to appreciate when assessing reduction. Understanding physiologic motion at this joint is crucial for developing surgical repair techniques after ligamentous injury. Imaging throughout active range of motion can also enable comparison of fixation methods in order to further elucidate causes of residual functional impairment.

Axial 4-dimensional computed tomography images showing syndesmotic reduction in plantar flexion (left) and dorsiflexion (right) as measured by the anterior (AN), middle (MN) and posterior (PN) syndesmosis distances.
Challenges and future directions
Continuous advancements are being made to 4DCT. It is expected that increasing availability and understanding of 4DCT will lead to an expansive scope for research and application in clinical practice.11 Advances in field of view can be achieved through increasing the number of detector rows or increasing detector size.4 However, the latter method would decrease axial resolution. Optimal acquisition protocols need to be determined to minimize radiation dosage and motion artifact without sacrificing resolution and the ability to track motion as desired.
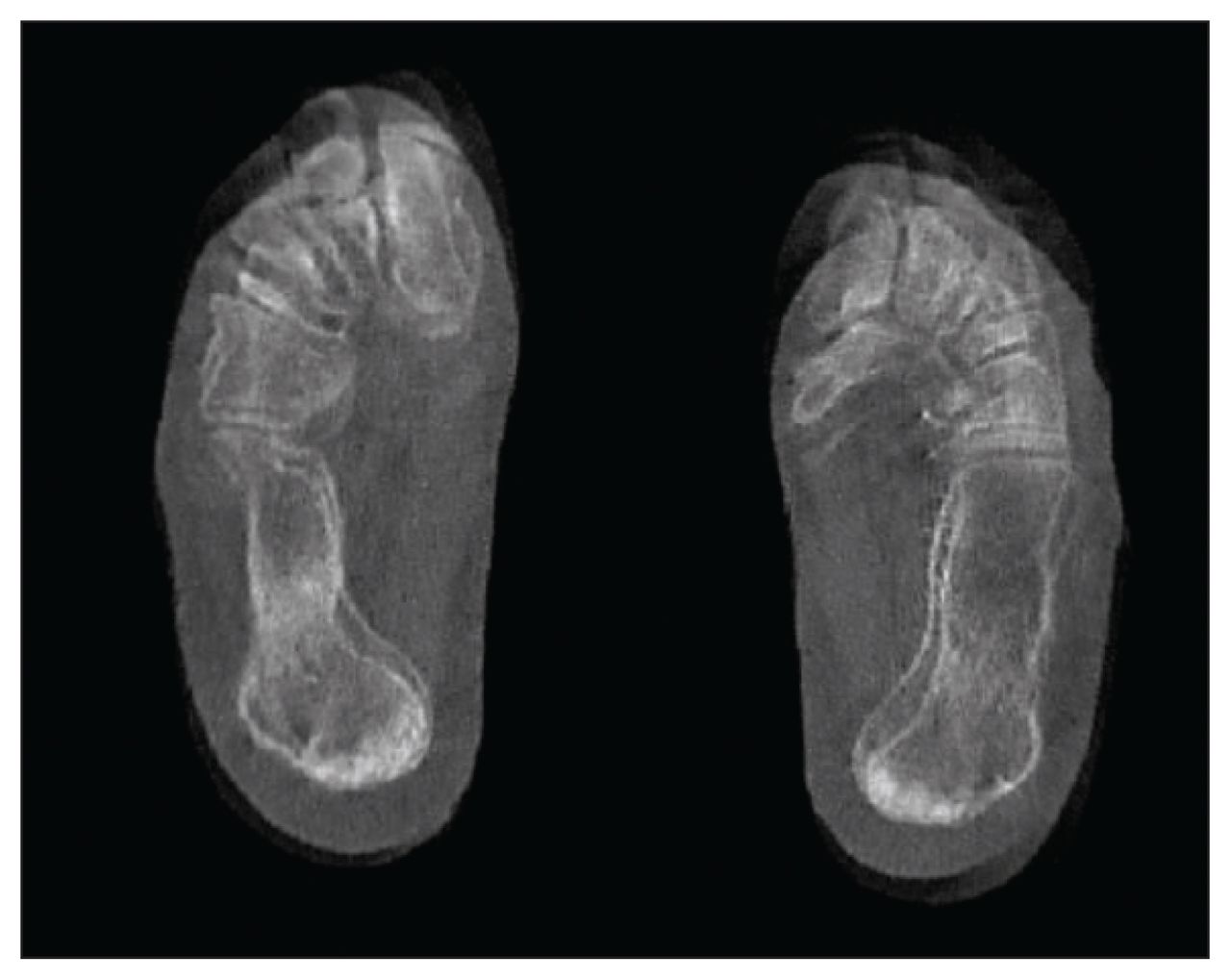
Motion artifact is another challenge (Figure 3). Recommendations have been made to design protocols to limit artifact by orienting the plane of motion optimally, and promoting smooth patient motion through training, external cues or custom devices to constrain range of motion or even simulate weight-bearing conditions.35–37 These recommendations regarding positioning and speed are not always feasible, however, as this motion must be achievable within the confined CT gantry, and some phenomena are observed only under particular conditions. Half reconstruction methods use only one-half of a gantry rotation to create an image, compared to a full rotation of projections. In dynamic applications, this serves to decrease motion artifact and reduce radiation exposure.35 Other advancements such as implementation of scanners with dual radiologic source technology and increased gantry rotation speeds can also reduce motion artifact.35

Axial 4-dimensional computed tomography images showing that substantial motion artifact occurs in the forefoot during ankle plantar flexion and dorsiflexion if the tibia remains stationary. Motion artifact can be minimized by holding the area of interest in a fixed position and moving the body or limb relative to that area of interest.
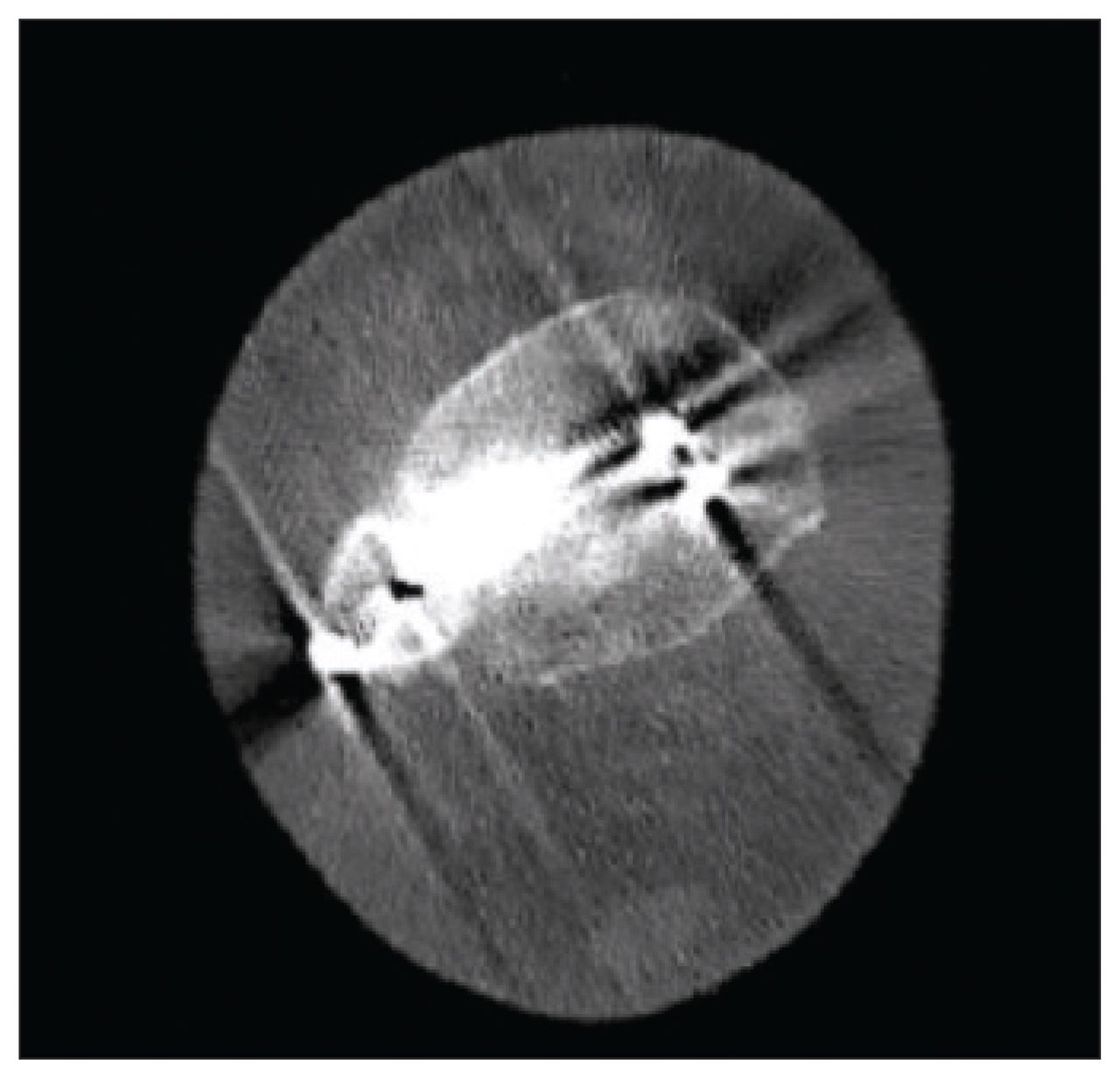
Metal artifact from implants also poses substantial challenges for image interpretation and processing in the investigation of postsurgical motion (Fig. 4). To our knowledge, no studies have incorporated metal suppression via dual-energy CT into dynamic protocols, likely because dual-energy CT would decrease the temporal resolution and increase the radiation dosage. As a result, metal artifact reduction is currently limited to postprocessing algorithms and manual correction, which requires increased user time and may reduce the accuracy of results.

Axial 4-dimensional computed tomography images showing an ankle with metal implants after open reduction internal fixation of an ankle fracture. The metal artifact disrupts image-processing routines and obscures the anatomy.
Concerns regarding radiation exposure continue to limit the adoption of 4DCT as well. In general, the more proximal the area to be imaged, the higher the effective radiation dosage.2 Improvements continue to be made in radiologic source hardware and iterative reconstruction techniques to lower the dosage produced by the source while still maintaining image quality.38
Finally, 4DCT produces large data sets that result in substantial image-processing time and effort. Qualitative analysis of motion is possible, and multiple manufacturers and software packages provide the ability to visualize 3-dimensional reconstructions at each time point. However, quantitative analysis requires further postprocessing, with segmentation of individual bones and registration of these bones across time points. Currently, there are limited commercially available software packages that can semi-automate measurement and analysis protocols. More work is required to make versatile tools available for ease of use and clinical implementation.
Conclusion
Four-dimensional CT technology remains in its early stage but has promising clinical and research applicability in numerous areas, including assessment of diagnosis, prognosis and surgical outcome for many musculoskeletal disorders. As the technology evolves and is adopted more widely, it can be applied to joint kinematics and the quantification of instability, maltracking and impingement. Future work should focus on improving image quality and patient safety to enable wider adoption. Consequently, novel uses of 4DCT should improve the diagnosis and treatment of a wide variety of musculoskeletal conditions.
Footnotes
Competing interests: Prism Schneider reports research grants from the Canadian Institutes of Health Research, the Orthopaedic Trauma Association and Johnson & Johnson, outside the submitted work. She has received consulting fees and honoraria for presentations and educational events from Amgen. She is a member of Osteoporosis Canada’s Scientific Advisory Council. No other competing interests were declared.
Contributors: M. Wong and P. Schneider designed the study. C. Wiens and M. Kuczynski acquired the data, which S. Manske analyzed. M. Wong wrote the manuscript, which C. Wiens, M. Kuczynski, S. Manske and P. Schneider critically revised. All authors gave final approval of the article to be published.
Funding: Michael Kuczynski received funding for doctoral work for this study from the Natural Sciences and Engineering Research Council of Canada (NSERC PGS-D) through the University of Calgary.
- Accepted June 8, 2021.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.