


Abstract
Background: Frequently occurring in adolescents, osteosarcoma is the most common primary malignant bone disease, with a reported 15% of patients who present with metastasis. With advances in imaging and improvements in surgical care, an updated analysis is warranted on the outcomes of pediatric patients with osteosarcoma.
Methods: We completed a retrospective review of pediatric patients who presented with osteosarcoma between 2001 and 2017, using The Cancer in Young People in Canada (CYP-C) national database. Data on 304 patients aged younger than 15 years were analyzed.
Results: The proportion of patients who presented with metastasis was 23.0%. The overall 5-year survival (OS) for patients who presented with metastasis was 37.4%. Overall survival and event-free survival (EFS) were lower in these patients than in patients with localized disease (hazard ratio [HR] 4.3, p < 0.0001 and HR 3.1, p < 0.0001). For patients who presented with metastatic disease, the OS for those undergoing an operative intervention was 44.1% compared with 17.6% for those who did not undergo resection (p < 0.0001).
Conclusion: The proportion of patients who presented with metastatic osteosarcoma in our population is higher than previously reported. Overall outcomes of patients with metastatic disease have not changed. Our data reaffirm a role for surgical resection in patients with metastasis with a need to explore new treatment strategies to improve the overall prognosis of these patients.
Osteosarcoma is the most common primary malignant bone disease, typically affecting patients aged 20 years or younger. The incidence of osteosarcoma is estimated at 4–5 cases per million people. It has a bimodal age of presentation, with the highest peak in adolescents aged 10–19 years, and a second peak in the seventh decade of life.1,2 Osteosarcomas are typically responsive to chemotherapy, resistant to radiotherapy and most commonly metastasize to the lungs. Improvements in survival for patients with osteosarcoma were apparent after the introduction of cisplatin-based systemic chemotherapies to treatment regimens in the 1980s.3 Further advances in imaging, chemotherapy protocols, surgical expertise and engineering have resulted in improvements in both local and systemic tumour control. For patients aged younger than 15 years, improvements in treatment over time have been achieved with an increase in 5-year overall survival (OS) from 40% (1975–1978) to 68% (1987–1990), with notably minimal improvements in 5-year OS in the last 3 decades.4 This plateau in patient survival is apparent in studies using longitudinal, multi-centre databases.1,4 However, there is a subset of patients for whom survival has continued to improve. A 2010 analysis of the Surveillance, Epidemiology, and End Results (SEER) program database of the National Cancer Institute identified improvements in survival for all patients with high-grade disease over the preceding 2 decades.1 The authors of the SEER study argue that this improved survival is owing to the use of more specific intensified chemotherapy regimens for patients with an aggressive disease. Although survival has improved over previous decades, patients with metastatic and recurrent disease continue to have poor outcomes.1,4
The current treatment regimen for patients with osteosarcoma involves neoadjuvant multi-agent chemotherapy, with the goal of addressing micro-metastases, inducing primary tumour necrosis and facilitating complex surgical planning. Neoadjuvant chemotherapy is followed with wide surgical resection with either a limb salvage reconstruction, or other ablative surgery such as amputation or rotationplasty.5–9 Localized control is then followed by an adjuvant multi-agent chemotherapy. Event-free survival (EFS) and OS are more likely in patients who achieve a higher degree (> 90%) of histologic necrosis in response to neoadjuvant chemotherapy.10,11
The presence of metastatic disease is an independent indicator of poor prognosis, and is typically managed aggressively with multi-agent chemotherapy, surgical resection of metastatic sites and the use of palliative radiotherapy.12–14 The overall prevalence of metastatic disease at the time of osteosarcoma diagnosis is commonly reported to be about 15%.15,16 The studies that have provided this estimate are from small to moderate-size populations from the previous 30–40 years.16 With the evolution of imaging technology, it is possible to detect smaller metastatic lesions earlier in their course. The ability to accurately detect metastatic disease early may change our understanding of the prevalence of metastases at diagnosis and provide opportunities to further improve care. Studies have confirmed that the removal of surgically resectable disease in patients with distant metastases is beneficial for overall survival.17,18 However, these repeated procedures come with a risk of severe complications and strain on patients and their families.19,20 Understanding the rates of success of repeated surgical resections in metastatic osteosarcoma would be informative for comprehensive patient care.
This retrospective analysis provides a national review describing the proportion of pediatric patients (aged younger than 15 years) with osteosarcoma who present with metastatic disease at the time of initial diagnosis. We further aimed to describe patient outcomes and characterize surgical management, including a comparison of the number of operations undertaken to overall outcomes.
Methods
The Cancer in Young People in Canada (CYP-C) program, launched in 2009 (data collection began in 2001), is a collaborative database among all 17 pediatric cancer centres across Canada.21 We obtained data on patients aged younger than 15 years who were diagnosed with osteosarcoma in Canada between 2001 and 2017. We extracted data on demographic information, location of the primary tumour, tumour histologic subtypes, presence and location of metastasis, number of surgical interventions, use of adjuvant treatment and survival data. Survival data included EFS (defined as time from presentation to disease recurrence or death) and OS. Comparisons between patients who present with localized versus metastatic disease were made. Two-sample t tests were used for normally distributed variables to compare the differences between groups. A Mann–Whitney U test was used on non-normally distributed continuous variables. Fisher exact and χ2 tests were used for comparing categorical outcomes. Event-free survival and OS were analyzed using the log-rank test. Column numbers of less than 5 were rounded up to 5, in accordance with the CYP-C guidelines to ensure anonymity. Data supporting the findings of this study are available from the CYP-C.21
Ethics approval
Ethics approval was obtained from the Health Research Ethics Board of Alberta, Cancer Committee (HREBA.CC-17-0456).
Results
Patient demographics
We identified 304 pediatric patients with osteosarcoma between 2001 and 2017. Of these patients, 234 presented with localized disease and 70 presented with metastatic disease. The proportion of patients who presented with metastatic disease was 23.0% and this proportion changed over time. Between 2001 and 2008, 18% of patients presented with metastatic disease compared with 28% of patients between 2009 and 2017. Table 1 shows the age, gender distribution, ethnicity, location of primary disease and morphological subtypes of disease among the groups. When comparing demographics between patients who presented with localized versus metastatic disease, there were no significant differences identified (Table 1). The mean age of patients at presentation was 11.0 years. Among the patients who presented with metastatic disease, 70% had isolated lung metastases (26% unilateral and 44% bilateral, Table 2).
Demographic and clinical characteristics of the study cohort
Location of metastatic disease on presentation
Patient survival
Overall survival and EFS were compared between patients who presented with localized and those who presented with metastatic disease. As expected, OS was significantly decreased in patients who presented with metastatic disease compared with patients with localized disease (Figure 1A, hazard ratio [HR] 4.3, p < 0.0001). The 5-year OS for patients who presented with metastatic disease was 37.4% compared with 76.3% for patients with localized disease. The median survival of patients who presented with metastatic disease was 2.17 years. Similarly, 5-year EFS was significantly decreased in patients who presented with metastatic disease compared with localized disease (Figure 1B, 66% v. 31.2%, HR 3.1, p < 0.0001).

Outcome of patients who presented with localized versus metastatic disease. (A) Overall survival. (B) Event-free survival.
Number of operative interventions and outcomes
We extracted data on the number of operative oncologic interventions and reconstructive procedures each patient received (Table 3). When comparing outcomes, reconstructive procedures completed in isolation were not included as oncologic operative interventions. Most patients (67%) underwent 1–2 oncologic operations during their treatment course. The proportion of patients undergoing 0, 1–2, or 3 or more oncologic operations was compared between patients who presented with metastatic disease and those who presented with localized disease. There was a significant difference between the groups; patients who presented with metastatic disease were more likely to have either no or 3 or more operative oncologic interventions than patients with localized disease (26% and 23% v. 11% and 11%, respectively, p = 0.0001).
Number of surgeries performed per patient
Overall survival was compared among patients undergoing 0, 1–2, and 3 or more operative interventions regardless of localized or metastatic disease at presentation (Figure 2A). The 5-year OS for patients having no surgery, or needing at least 3 surgeries, were 49.7% and 49.8%, respectively. In comparison, patients undergoing 1–2 operative interventions had a significantly higher 5-year OS of 76.2% (p < 0.0001).

Overall survival stratified by the number of surgical resections and disease on presentation. (A) Overall survival of all patients stratified based on the number of resections. (B) Overall survival of patients with localized disease on presentation stratified based on the number of resections. (C) Overall survival of patients with metastatic disease on presentation stratified based on the number of resections. (D) Overall survival of patients who presented with 3 or more resections comparing local with metastatic disease.
Five-year OS was compared between patients who presented with localized disease and underwent 1–2 resections and those who underwent 3 or more surgical resections (Figure 2B). The 5-year OS for patients with localized disease who had 1–2 operations was 82.6% compared with 39.3% for those requiring 3 or more operations (p < 0.0001). A similar comparison was made in patients who presented with metastatic disease (Figure 2C). The 5-year OS was not significantly different (47.4% for patients having 1–2 resections v. 36.6% for those having 3 or more, p = 0.17). Figure 2D compares patients who presented with metastatic disease and those who presented with localized disease and underwent 3 or more surgical resections. The 5-year OS was not significantly different between groups (39.3% for localized disease at presentation v. 36.5% for metastatic disease at presentation, p = 0.77).
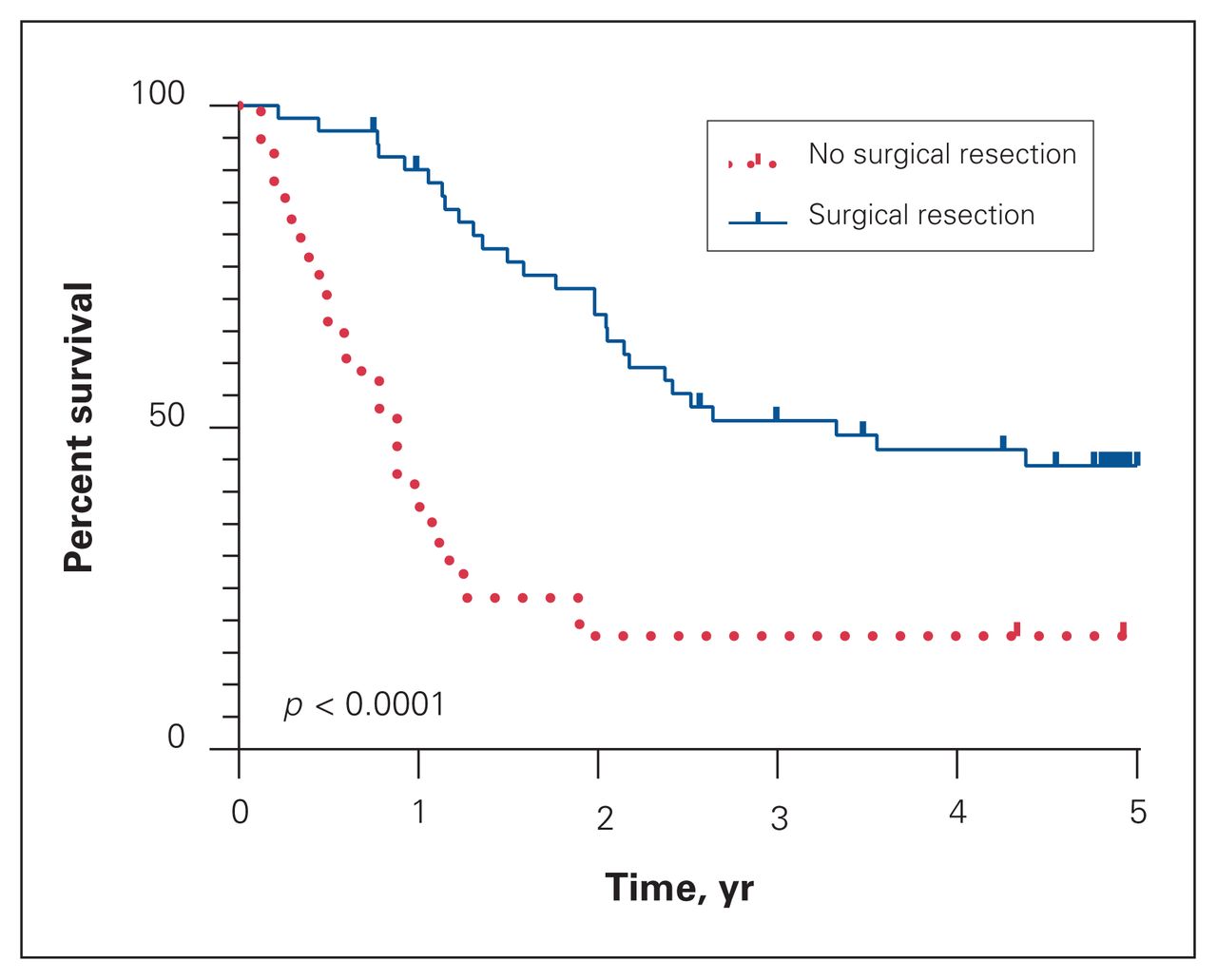
Survival was compared between patients who presented with metastatic disease who underwent a surgical resection and those who did not undergo a resection. The 5-year OS was significantly higher in patients who had a surgical resection than in those who did not (Figure 3, 44.1% v. 17.6%, p < 0.0001).
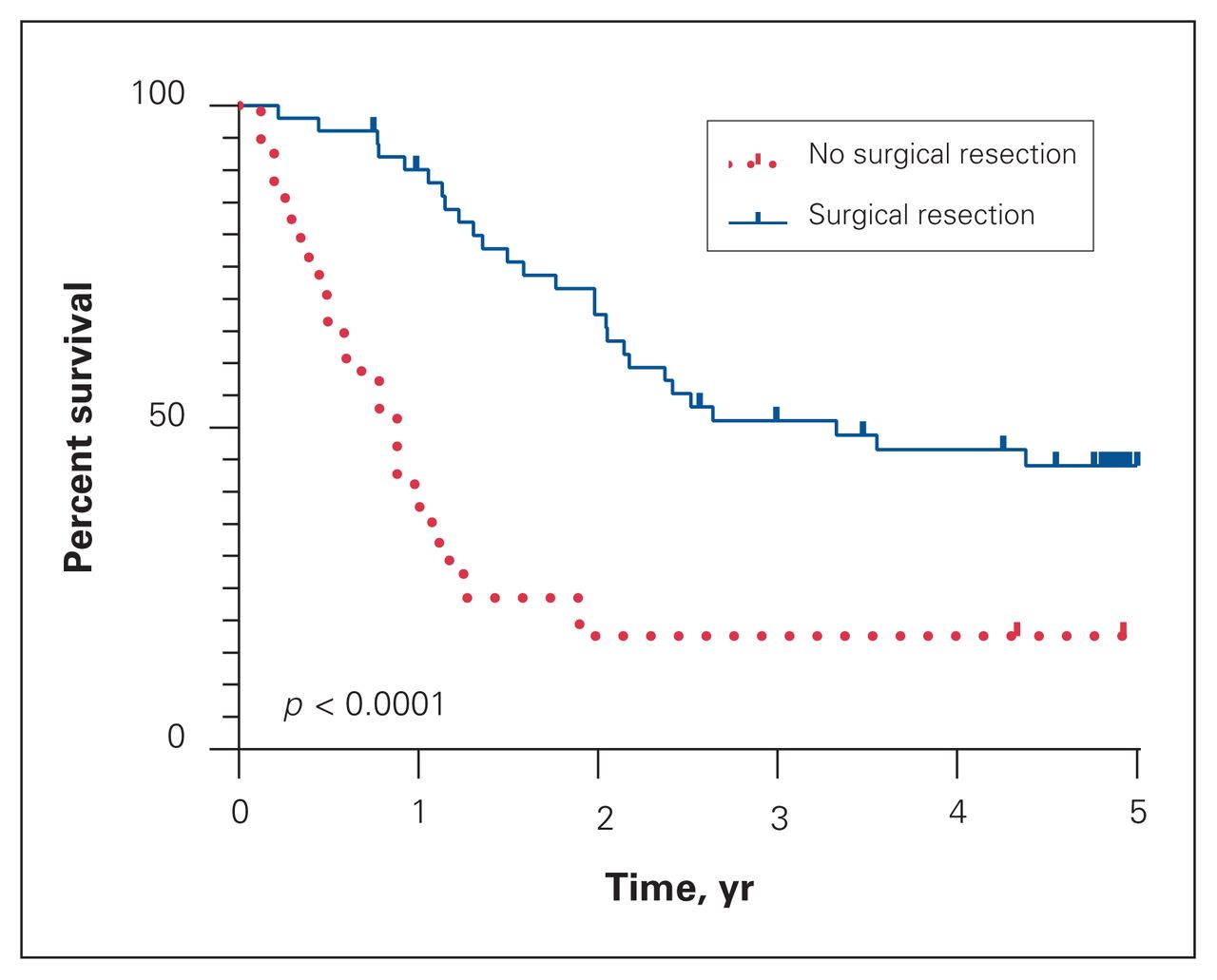
Overall survival of patients who presented with metastatic disease that underwent surgical resection compared with no surgical resection.
Adjuvant treatment
Appendix 1, Table S1, available at www.canjsurg.ca/lookup/doi/10.1503/cjs.008220/tab-related-content, describes the proportion of patients receiving neoadjuvant or adjuvant chemotherapy, radiation therapy or both. In total, 88% of patients received neoadjuvant/adjuvant therapy (75% chemotherapy alone, 3% radiation alone and 10% chemotherapy and radiation). Cisplatin and doxorubicin-based chemotherapy regimens were the most common first-line therapy used, with etoposide and ifosfamide also delivered in many cases throughout individual treatment courses. In patients who received radiation therapy, survival was poor, with a median survival of 3.6 months from the beginning of treatment (Appendix 2, Figure S1, available at www.canjsurg.ca/lookup/doi/10.1503/cjs.008220/tab-related-content).
Discussion
Given advances in imaging technology, surgical care and systemic therapy over time, an updated review of the presentation and outcomes of patients with osteosarcoma is necessary. In this retrospective population-based study, 23% of patients presented with metastatic disease and had a 5-year OS of 37.4%. Patients who presented with a localized disease had a 5-year OS of 76.3%. Patients who presented with metastatic disease and were able to undergo a surgical resection showed favourable survival compared with those who did not have surgery, as expected (5-year OS of 44.1% v. 17.6%, respectively). Across this entire patient population, the median number of surgical procedures for oncologic resection was 1. In this population, 88% received neoadjuvant/ adjuvant therapy.
Previous studies have reported on the proportion of pediatric patients who presented with metastatic osteosarcoma compared with localized disease. Meyers and colleagues17 assessed 342 patients with osteosarcoma of whom 18% presented with metastatic disease. Other studies have reported a range of proportions, from 11.4% to 18%.16,22,23 Within the CYP-C study population, the proportion of patients who presented with metastatic disease was higher than in the literature. The proportion of these patients also increased with time (18% between 2001 and 2008 v. 28% between 2009 and 2017). This may be because of improvements in imaging resolution and an expanded ability to detect microscopic disease. In concordance with other studies, bilateral pulmonary metastases was the most common pattern of advanced disease in our cohort (Table 2).23
In our study, survival outcomes were similar to those of previously published cohorts. Patients with isolated localized disease had a 5-year OS of 76.3% compared with 37.4% in patients with metastatic disease. The Cooperative Osteosarcoma Study Group (COSS) showed a 5-year OS of 33% in patients aged 20 years or younger who presented with metastatic disease.12 Similarly, Janeway and colleagues22 reported on collective 5-year OS outcomes of 75% for patients with localized disease compared with 36% for patients with metastatic disease. Given the lack of improvement in outcomes over several decades, identifying new therapeutic strategies for patients with localized and metastatic osteosarcoma must be prioritized.
Multiple surgical resections were undertaken in the context of recurrent or residual disease. For patients who presented with localized disease who required 1–2 operative resections, 5-year OS was 82.6%, compared with 39.3% for those patients requiring 3 or more operations (Figure 2B). For patients who presented with metastatic disease, the 5-year OS for those requiring 1–2 operations, and those requiring 3 or more operations were 47.4% and 36.6%, respectively (Figure 2C). This compares favourably to patients with metastatic disease who did not have a surgical resection (5-year OS of 17.6%). The poor outcomes of patients requiring multiple operative interventions reflects an aggressive tumour biology with multiple interventions undertaken for initial metastases, rapid growth or metastatic spread of previously localized disease. However, although patients undergoing 3 or more surgeries would be expected to have a more aggressive disease either at presentation or recurrence, survival for patients undergoing multiple operations likely underestimates the mortality rate associated with the highest risk cases. Survivorship bias is reflected in these data as those patients who survive to undergo 3 or more surgeries would likely not have had aggressive and rapidly progressive disease. This likely explains a near 100% early survival rate for the first 2 years in this patient population that subsequently decreases after 2 years.
Despite these caveats, the opportunity to achieve meaningful survival even after multiple surgeries supports the current practice of operative removal of metastatic disease when possible (Figure 3).17 Within the population of patients requiring 3 or more surgeries, there was no difference in outcomes between patients who presented with localized disease and those who presented with metastatic disease (Figure 2D). Understanding how patient outcomes are related to the number and frequency of operative interventions provides a prognostic indicator that can be useful when counselling patients.
Within this study, we examined the proportion of patients receiving systemic therapy. Nearly all patients received neoadjuvant or adjuvant chemotherapy with cisplatin and doxorubicin as first-line agents followed by etoposide and ifosfamide in most cases, particularly in cases of disease recurrence.3,24,25 Radiation therapy was delivered primarily for palliation of patient symptoms, and the median survival for patients undergoing radiation treatment was 3.6 months after delivery of treatment (Appendix 2, Figure S1). Osteosarcoma is known to be relatively radiation resistant, and patients receiving radiation for their disease have a worse prognosis than those who do not require radiation.1 These data provide valuable information for patient prognosis once radiation therapy is needed for symptom control.
Limitations
The strengths of this study include the use of an in-depth, multi-centre population-based database. The CYP-C is comprehensive and includes data on demographics, diagnostics, time to treatment and other details such as relapse and complications. The effects of selection and referral bias are therefore limited. To our knowledge, this is the first population-based study to describe a relationship between the number of operative interventions aimed at disease resection and survival, providing valuable information on patient prognosis. A significant limitation of our study is the retrospective nature of our analysis. Also, the CYP-C database does not include adolescents (aged younger than 15 years). Information regarding tumour histology and resection margin status was not available and these data may have affected our results.
Conclusion
Our study shows the proportion of pediatric patients who presented with metastatic compared with localized osteosarcoma in our population was higher than that in the reported literature. When comparing the data from the CYP-C database with previously published results, the overall outcomes of patients with localized or metastatic disease have not changed significantly over time. Our data reaffirm a role for surgical resection in patients with metastatic disease in the modern era and provide prognostic information stratified by the number of operative resections required. According to our results, there remains a need to identify new adjuvant treatment strategies to improve the overall prognosis of pediatric patients with osteosarcoma.
Acknowledgements
The authors gratefully acknowledge the contributions of study participants, the participating pediatric oncology centres, members of the Cancer in Young People in Canada (CYP-C) Management and Steering Committees, the Pediatric Oncology Group of Ontario (POGO) and the five POGO Hospital Partners.
Footnotes
Submitted/presented at the 2020 Canadian Orthopaedic Association (COA) Annual Meeting and the 2019 Connective Tissue Oncology Society (CTOS) Annual Meeting.
Competing interests: None declared.
Data sharing: Restrictions apply to the availability of these data, which were used with permission for this study. Application for data release can be made through CYP-C at http://www.c17.ca/index.php?cID=7.
Funding: The CYP-C is fully funded by the Public Health Agency of Canada.
Disclaimer: Data used in this publication are from the Cancer in Young People in Canada Surveillance Program and are used with the permission of the Public Health Agency of Canada. The analyses and interpretation presented in this work do not necessarily reflect the opinions of the federal government of Canada. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
- Accepted October 20, 2021.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.