


Summary
Identifying characteristics of disciplined surgeons is important for public safety. A database of all physicians disciplined by a Canadian provincial medical regulatory authority (College of Physicians and Surgeons) between 2000 and 2017 was constructed, and comparisons between surgeons and other physicians were undertaken. Of 1100 disciplined physicians, 174 (15.8 %) were surgeons. Obstetrics and gynecology was the specialty with the most disciplined surgeons (57 of 174 [32.8%]), followed by general surgery (48 of 174 [27.6%]). The overall disciplinary rate for surgeons was higher than for other physicians (12.59, 95 % confidence interval [CI] 10.69–14.83 v. 9.85, 95 % CI 8.88–10.94 cases per 10 000 physician-years, p = 0.013). Even after adjusting for surgeon age, sex, international medical graduation and years in practice, surgeons remained more likely than other physicians to be disciplined for standard of care issues (55.6%, 95% CI 46.6–64.2 v. 38.7%, 95% CI 32.6–45.2, p < 0.001).
Physician discipline through self-regulation is important for the medical profession to ensure patient safety and improve quality of care. Estimated rates of disciplinary action against licensed physicians ranges from 0.3% to 2.8%.1 Although disciplinary rates are low, any misconduct has the potential to compromise patient safety and quality of care. In Canada, provincial medical regulatory authorities, known as the Colleges of Physicians and Surgeons (CPS), govern standards of professional practice, and rulings of physician discipline are publicly available. We designed a national database using CPS data to compare surgeons with other physicians, and to determine areas of practice that could benefit from closer evaluation and targeted preventive strategies.
Canadian physicians disciplined between Jan. 1, 2000, and Dec. 31, 2017, were identified from the CPS. Relevant demographic information was collected, including sex, type of practice licence, location of medical training (Canadian/US-trained versus international medical graduate [IMG]), and medical specialty. Information on the offenses and penalties incurred was also collected. The Canadian Institute of Health Information was used to identify the total number of practising physicians in the country during the study period.2
Unadjusted comparisons between surgeons and other physicians were undertaken using χ2 and Student t tests for categorical and continuous variables, respectively. For the primary analyses, we identified 11 types of offenses and 8 types of penalties, and created indicator variables for each. These were used as the outcome for logistic regression. Generalized estimating equations were selected to estimate the percent of cases with a given offense/penalty for surgeons compared with other physicians, while allowing for covariate adjustment (gender, year of study, years in the profession, and IMG status). Secondary analyses of yearly and aggregate disciplinary rates were performed using negative binomial regression. We report cases per 10 000 physician years with 95% confidence intervals (CIs). The threshold for statistical significance was α = 0.05. Statistical analyses were performed using R software, version 3.1.2.
Disciplinary findings
From 2000 to 2017, there were 1269 disciplinary cases involving 1100 different physicians. There were 199 disciplinary cases attributed to 174 surgeons, and 1070 disciplinary cases attributed to 926 other physicians (Figure 1 and Table 1). Nineteen (11%) surgeons underwent multiple disciplinary proceedings. Over the study period, surgeons accounted for 15.7% of all disciplined physicians, despite accounting for just 12% of all physicians with a licence to practise in Canada (p < 0.001).
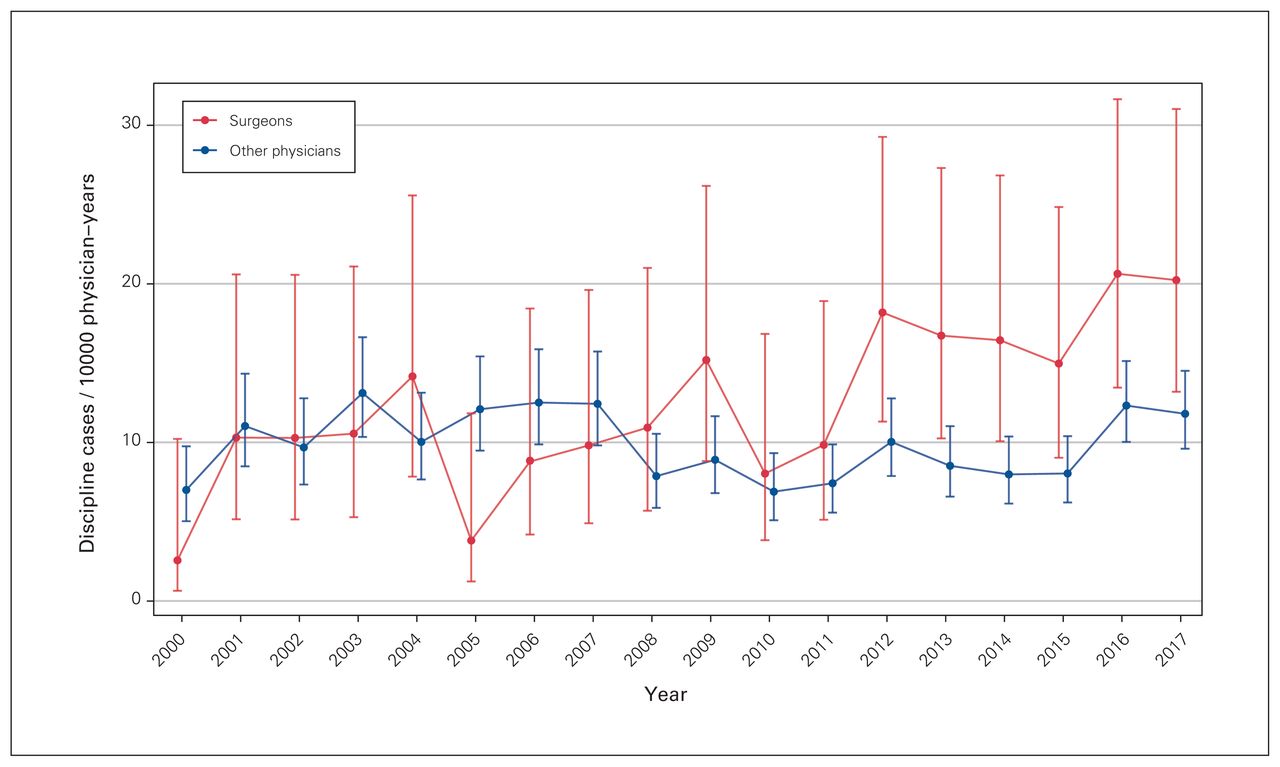
Disciplinary rates for all cases by year, for surgeons compared with other physicians. Error bars denote 95 % confidence intervals.
Baseline characteristics of disciplined surgeons and other physicians (2000–2017)
Most surgeons disciplined were male (92.5%) and independent practitioners (97.7%). On average, disciplinary action for surgeons occurred 31.4 years after medical school graduation. Obstetrics was the most frequently disciplined surgical subspecialty (57 of 174 [32.8%]), followed by general surgery (48 of 174 [27.6%]) (Table 2). The proportion of surgeons disciplined in both of those specialties was higher than the proportion of those specialists with a licence to practise in Canada during the study period (Table 3).
Baseline characteristics of disciplined surgeons, by specialty (2000–2017)
Proportion of disciplined surgeons, by specialty (2000–2017)
Disciplinary rates of surgeons have exceeded that of other physicians consistently since 2008 (Table 4). The overall disciplinary rate for surgeons was higher than for other physicians (12.59, 95% CI 10.69–14.83 v. 9.85, 95% CI 8.88–10.94 cases per 10 000 physician-years, p = 0.013).
Disciplinary rates for surgeons versus other physicians, by year (2000–2017)
After adjustment, surgeons were more likely than other physicians to be disciplined for standard of care issues (55.6%, 95% CI 46.6–64.2 v. 38.7%, 95% CI 32.6–45.2, p < 0.001) (Table 5). Surgeons were less likely than other physicians to be disciplined for sexual misconduct (p = 0.001), inappropriate prescribing (p = 0.021), or conviction of a crime (p = 0.015). They were also less likely to have their licence revoked (8.5%, 95% CI 5.0–14.2 v. 14.4%, 95% CI 10.4–19.5, p = 0.039).
Disciplinary differences among surgeons & other physicians in Canada (2000–2017)
Discussion
We report disciplinary findings for all disciplined physicians across Canada between the years 2000 and 2017. This study period and national scope of assessment was sufficiently large to capture events of misconduct, which are relatively infrequent in nature. We subcategorize disciplinary action against surgeons by specialty, and therefore contribute to the limited data on disciplined surgeons. Our analyses not only examined the risk associated with specialty, but also considered the confounding effects of years in practice, sex, age, and international medical education.
Nearly all disciplined surgeons were male; whereas three-quarters of Canadian surgeons are male,2 male surgeons accounted for 92.5% of all disciplined surgeons in the country during the study period. This is consistent with previous studies that reported that male physicians had higher disciplinary rates than female physicians.1,3 Notably, our observation that disciplined surgeons are more likely to be male lost significance when we adjusted for years since graduation from medical school, suggesting that this finding may be confounded by age. Historically, the field of surgery was male dominated, and consequently, male surgeons in our cohort tend to be older than their female counterparts.
Disciplinary action against physicians was more common later in practice. The average number of years from medical school graduation until surgeon discipline was 31.4 years. As surgeons age, it is important to acknowledge potential concerns regarding burnout, cognition, dexterity, familiarity with new practice standards or communication style.4 Future research should aim to elucidate why older surgeons receive more disciplinary action.
Surgeons were also most likely to be disciplined for standard of care issues. This may be explained by the nature of the surgeon–patient relationship, which is often centred around a procedure. This differs from the longer-term therapeutic alliance that is common in other specialties.5 Since the surgeon–patient relationship is centred around a procedure, it is possible that complications of a surgery are more readily perceived as a reflection of a surgeon’s quality, rather than a recognized risk or adverse event.
Our findings must be interpreted in the context of a few limitations. First, published accounts of disciplinary action may underestimate true incidence rates of physician discipline, as only physicians found guilty after disciplinary investigation are captured. Second, our primary analysis on disciplinary offenses and penalties compared surgeons and other physicians. We were unable to further stratify by surgical specialty owing to the rarity of events.
Future research should delineate whether disciplinary rates differ by residency experience, open compared with minimally invasive procedures, and community compared with tertiary practice. Further qualitative research may supplement this work and identify themes and patterns regarding standard of care issues that cannot be captured through a quantitative approach.
Conclusion
Our novel, national database of physician discipline showed that surgeons are disciplined at higher rates than other physicians and more frequently for standard of care issues.
Footnotes
↵* These authors contributed equally to this manuscript and are considered to be co-first authors.
Competing interests: None declared.
Contributors: All authors contributed substantially to the conception, writing and revision of this article and approved the final version for publication.
- Accepted December 16, 2021.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
In this issue

{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.