


Abstract
Background: Delay of emergency surgery contributes to morbidity and mortality, and physiologic status affects outcomes of patients requiring emergent surgery. Our purpose was to determine whether delays to emergent surgery in children were associated with increased major morbidity or mortality in a risk-adjusted population.
Methods: We performed a retrospective review of class 1 (≤ 60 min to operating room) surgical procedures from July 11, 2011, to July 30, 2016, at BC Children’s Hospital, Vancouver. Data sources included the operating room database, patient charts, American Society of Anesthesiologists classification, Neonatal Acute Physiology (SNAP II) and Pediatric Risk of Mortality (PRISM III) scores, time from booking to operating room and outcome. Patients were classified as being at low or high risk for death. We defined major morbidity as unintended loss of an organ, limb or function related to surgery, and delay to surgery as more than 60 minutes from booking to in room. We used the χ2 test for univariate analysis and logistic regression for multivariate analysis.
Results: There were 384 cases (367 patients), 223 high-risk and 161 low-risk. The median age was 4 years (range 0 d–18 yr). Overall, 184 cases (47.9%) were delayed. Major morbidity occurred in 94 cases (24.5%), and 28 patients (7.6%) (all in the high-risk group) died. The mean time to the operating room was 1.46 hours for patients with major morbidity/mortality and 1.17 hours for those without. After adjustment for risk level, multivariate analysis showed delay to surgery to be associated with 85% increased odds of morbidity and/or mortality (adjusted odds ratio 1.85, 95% confidence interval 1.20–2.94) compared to no delay.
Conclusion: Delay to emergent surgery was associated with a significant increase in major morbidity and/or mortality. Children who require emergency surgery need their care prioritized by not only operating room teams but also hospitals and government; otherwise, they will continue to experience unintended consequences.
The primary objective of the Canada Health Act is “to protect, promote and restore the physical and mental well-being of residents of Canada and to facilitate reasonable access to health services without financial or other barriers.”1 Ensuring timely access to emergent surgical intervention has been recognized as a priority worldwide, with several countries implementing systems to collect data, benchmark and improve outcomes in this high-risk patient population.2
Well-established evidence shows that protected time for emergency operating rooms with teams available 24 hours a day, 7 days a week improves emergency surgery access and patient outcomes while decreasing costs.3–5 This model has been inconsistently adopted in Canada. In a review of the literature on emergency surgery, the authors stated, “Canada does not appear to be as advanced as the United Kingdom or the United States in terms of its approach to emergency surgery and focuses more on improving elective surgery.”2 Despite increased resources being directed at improving access for Canadians needing elective surgery, not only have some elective wait times increased, but evidence of preventable death in adults awaiting urgent surgery is mounting.6,7 Urgent and emergency surgery patients have been an “ignored and fragmented patient population” in Canada8 who are experiencing adverse outcomes owing to barriers in accessing surgical care.7
There is very little published literature on outcomes related to delays for children awaiting emergency surgery. In 2016, we published a 3-year retrospective audit of all emergency operations at our tertiary pediatric hospital.9 Most of the 4668 procedures were performed after daytime working hours, and patients requiring a class 1 (within ≤ 1 h) operation were the most likely to have their procedure delayed, with only 59.2% getting to the operating room within 1 hour from booking. The aim of the current study was to determine whether, in a risk-adjusted pediatric class 1 population, delays to surgery were associated with increased morbidity and/or mortality.
Methods
With research ethics board approval (CW11-0274/H11-0276), we performed a retrospective review of all emergent class 1 operations at BC Children’s Hospital, Vancouver, from July 11, 2011, to July 30, 2016. We used data from the Operating Room Scheduling Office System, which is a prospective operating room database. Data collected included booking time, in-room time, incision time, date of surgery, procedure class, duration of surgery, surgeon and service, as well as patient diagnosis and demographic characteristics. We reviewed the electronic medical record and the hospital chart to collect information on pre-maturity, congenital heart disease and American Society of Anesthesiologists (ASA) classification.
We used the validated scores for Neonatal Acute Physiology (SNAP II) and Pediatric Risk of Mortality (PRISM III) scoring systems to calculate mortality risk.10,11 Scores are calculated based on the most abnormal values in the 24 hours preceding surgery. The SNAP II score includes mean blood pressure, lowest temperature, partial pressure of oxygen/fraction of inspired oxygen, serum pH, seizures and urine output; a score less than 20 is indicative of a low risk of death (< 5%). The PRISM III score is typically used for the pediatric population in the intensive care unit and includes systolic blood pressure, diastolic blood pressure, heart rate, respiratory rate, partial pressure of oxygen in arterial blood/fraction of inspired oxygen, partial pressure of carbon dioxide, Glasgow Coma Scale score and pupillary reaction, as well as laboratory parameters; a score less than 6 is considered indicative of a low risk of death (< 5%). If laboratory variables used to calculate the SNAP II or PRISM III score were not available, a normal value was assigned. We considered SNAP II scores of 20 or more, and PRISM III scores of 6 or more to be indicative of a high risk for death. Patients were classified as being at high risk for death based on the appropriate mortality scoring and/or by an ASA classification of 3 or higher.
We calculated the duration from the time of booking to in room to determine whether the patient received surgical care within target. Cases for which booking time was not recorded were excluded.
For all patients, we collected time from booking to incision. For patients who died, data were also collected on the presence of active bleeding, shock and/or increased intracranial pressure. Time from surgery to death was measured. We collected major morbidity and mortality outcomes.
We defined procedure-specific major morbidity as the unintended loss of a portion of a limb or organ, or a permanent deficit in the function of a limb or organ associated with class 1 booking (e.g., loss of a testicle in surgery for testicular torsion would be a major morbidity, but loss of the appendix for appendicitis would not). Morbidities such as surgical site infections and urinary tract infections were not considered as procedure-specific major morbidities for this study. We assessed morbidities both per operation and per patient. To protect confidentiality for patients who died and had a delay to surgery, we revised patient diagnoses and procedures to a more generic description (e.g., the terms “brain tumour” and “craniotomy” were used instead of the specific site or type of brain tumour, and “intestinal perforation” and “laparotomy, intestinal resection” were used instead of anatomic location or reason for intestinal breach). If the date of death was not documented, we used the date of the last encounter as a surrogate. We calculated mortality on a per-patient basis.
In our institution, nursing staff is available nights and weekends in house (1 team), with a second team at home on call. Anesthesiology may have trainees in house, but this is variable, and attending anesthesiology staff have an expected maximum response time of 15 minutes to the hospital for cases after regular working hours. There is a second anesthesiologist on call nights and weekends as well. There is also a dedicated cardiac nursing team with an anesthesiologist available for emergent cardiac surgery patients. Most surgical residents and fellows are on home call, as are staff surgeons. Staff surgeons also have an expected maximum response time of 15–20 minutes for emergencies when on call. Typically, there is no back-up call for staff surgeons.
There is no “emergency room” for emergent cases during regular daytime hours at our institution. There is an “open access” room 4–5 days a week for urgent cases. This room is booked at 1000 the day prior. On weekdays, all nursing teams and anesthesiologists are assigned operating rooms. Thus, typically the only way for emergent cases to be completed during the day is if an elective or “open access” procedure finishes early, or a case is cancelled or bumped. These decisions are made by the anesthesiologist in charge.
Statistical analysis
The results are reported as median and range, or mean and standard deviation (SD). We performed descriptive, univariate logistic regression (unadjusted odds ratios [ORs]) and multinomial logistic regression (adjusted ORs). The results are based on univariate logistic regression, multivariate logistic regression and χ2 tests. We performed analyses using SPSS version 21 (IBM Corp.).
Results
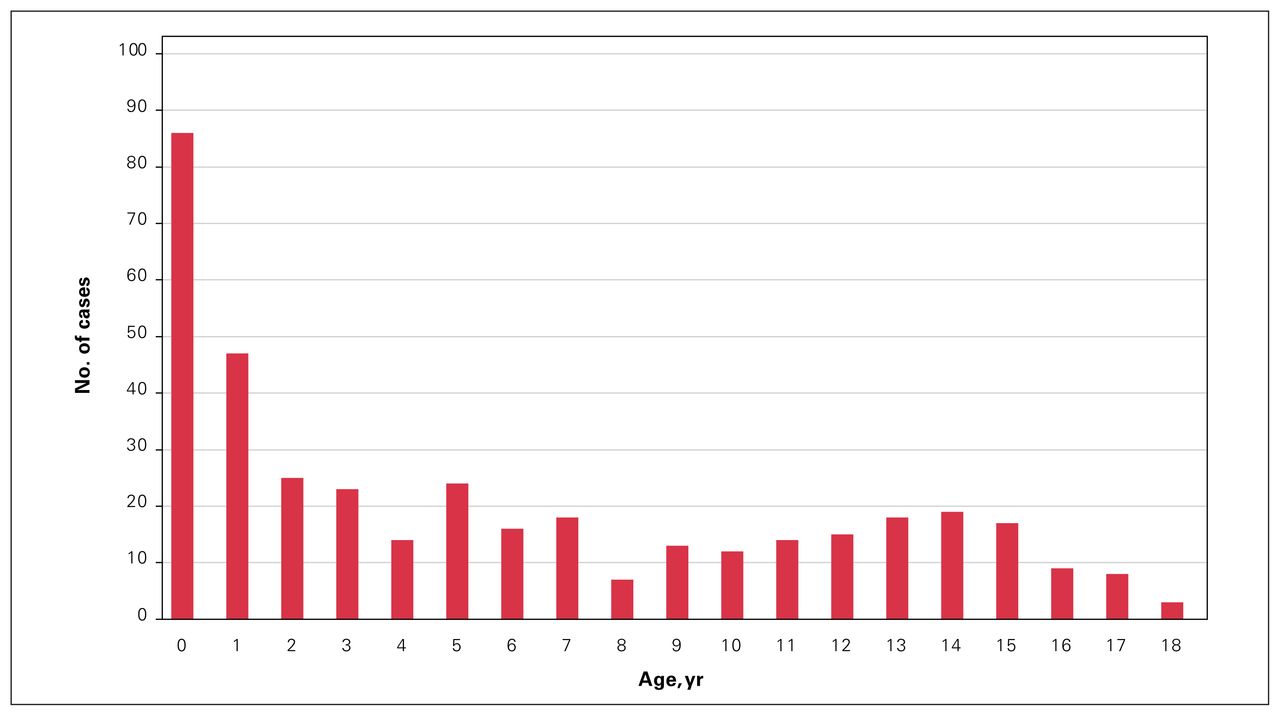
During the study period, there were 384 surgical procedures in 367 patients. The median age was 4 years (range 0 d–18 yr); 135 patients (36.8%) were infants aged 1 year or younger (Figure 1). The most common surgical services were general surgery, neurosurgery and otolaryngology (Figure 2). Prematurity was a comorbidity in 31 patients (8.4%), congenital heart defects in 49 (13.4%) and both in 9 (2.4%). Of the 384 procedures, 223 (58.1%) were classified as high risk, and 161 (41.9%) were classified as low risk. Of the high-risk group, 117 (52.4%) were in the operating room within 1 hour from booking, compared to 83 (51.6%) in the low-risk group. The overall median and mean times from booking to in room were 1.67 hours (range 0 h–18.8 h) and 2.07 hours (SD 1.46 h), respectively, for the high-risk group, and 1.33 hours (range 0.12 h–4.75 h) and 2.08 hours (SD 1.72 h), respectively, for the low-risk group.

Distribution of cases by age.
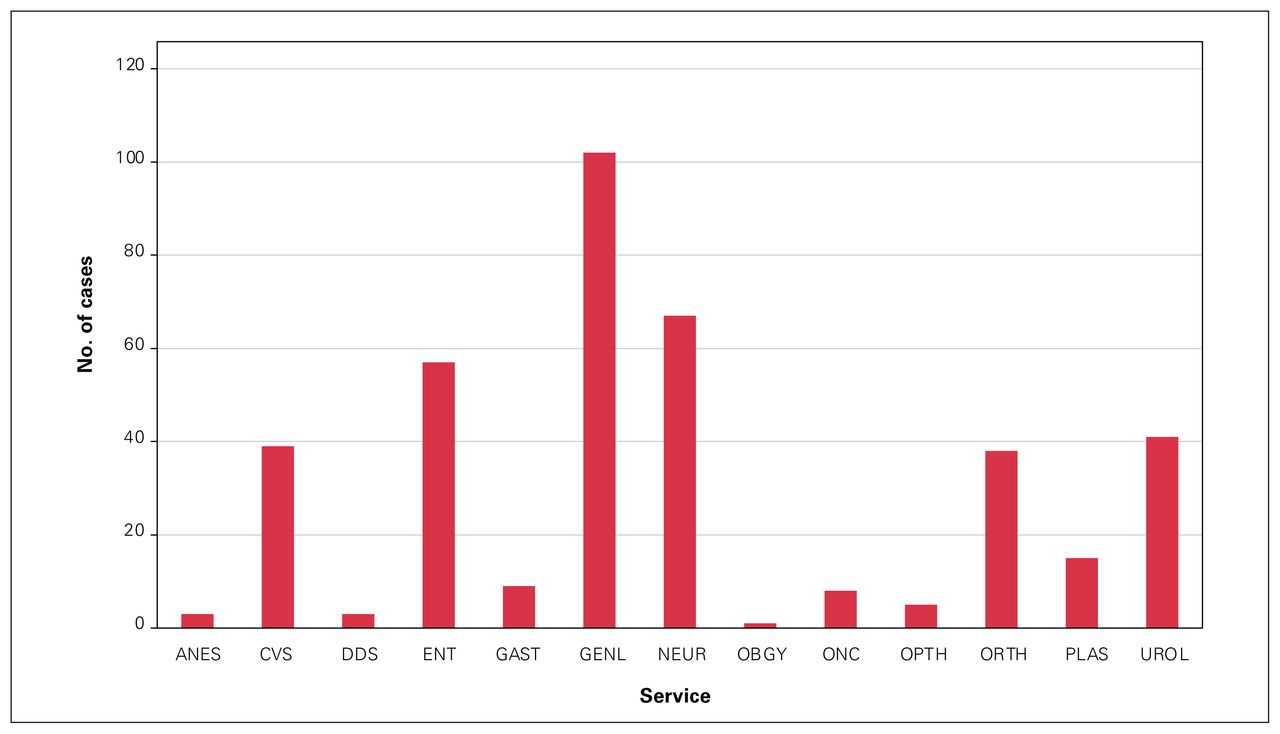
Distribution of cases by surgical service. ANES = anesthesiology; CVS = cardiac surgery; DDS = dentistry; ENT = otolaryngology; GAST = gastroenterology; GENL = pediatric surgery; NEUR = neurosurgery; OBGY = obstetrics and gynecology; ONC = oncology; OPTH = ophthalmology; ORTH = orthopedic surgery; PLAS = plastic surgery; UROL = urology.
Major morbidity occurred in 94 cases (24.5%), and 28 patients (7.6%) died; the latter were all in the high-risk group (Figure 3). Compared to the low-risk cases, the high-risk cases had more than twice the odds (OR 2.15, 95% confidence interval [CI] 1.34–3.45) of morbidity and/or mortality. Having a history of prematurity was associated with increased mortality (p = 0.04); however, congenital heart disease was not (p = 0.2). The high-risk category was significantly associated with mortality (p = 0.003). Patients who had a major morbidity and/or who died had greater median and mean times to the operating room (1.05 h, range 0 h–13.67 h, and 1.46 h, SD 1.51 h, respectively) than patients with no major morbidity and/or mortality (0.88 h, range 0.08 h–18.80 h, and 1.17 h, SD 1.38 h, respectively). The median and mean time from booking to incision were 1.05 hours (range 0.25 h–15.25 h) and 1.46 hours (SD 1.76 h) for those who experienced major morbidity and/or died, versus 0.85 hours (range 0.22 h–19.32 h) and 1.14 hours (SD 1.45 h) for those who did not. These corresponding values for patients who did not survive versus those who did were 1.83 hours (range 0.3 h–4.88 h) and 1.82 hours (SD 0.98 h) versus 1.43 hours (range 0.22 h–19.32 h) and 1.78 hours (SD 1.61 h), respectively. After adjustment for risk level, multivariate analysis showed time to the operating room of more than 1 hour to be associated with 85% increased odds of morbidity and/or mortality (adjusted OR 1.85, 95% CI 1.20–2.94) compared to time to the operating room within 1 hour. There was no association between morbidity or mortality and time from booking to incision (p = 0.1).

Outcome based on mortality risk and delay to operating room. *Two patients had 2 class 1 operations, and 1 patient had 5 class 1 operations. They were categorized as having a delay of more than 1 hour if any of their operations were delayed.
Most deaths occurred in infants who required general surgical, neurosurgical or cardiac surgical intervention; their median age was 0.4 years. Of the 28 patients who died, 18 experienced delays in transport to the operating room (Table 1).
Pediatric patients with delayed class 1 surgery who died
Discussion
In our study, class 1 emergency surgery patients were able to access the operating room within the target window only 52% of the time. Patients at high risk for death were significantly more likely to experience major morbidity and/or death than those at low risk. Furthermore, in risk-adjusted analysis, delay to the operating room was independently associated with a significant increase in major surgical morbidity and/or mortality. The results of this study have been shared with our operating room teams and leadership to explore possible solutions.
Evidence showing that delays to emergency surgery among adults are associated with adverse outcomes has been mounting for more than 2 decades in North America.5,7,12 Emergency access to the operating room during daytime hours when elective procedures are performed may pose a challenge. In the adult population, many centres now have dedicated operating rooms during the day-time for emergency operations to improve access and outcomes. In Canada, general surgery has led these efforts, and acute care surgery teams have been in place in many hospitals for more than a decade.13 Evidence from these centres has shown that this approach has improved timely surgical access for this critical group of patients without elective operations being cancelled, with potential cost savings to the health care system.13–16 Separation of surgical teams for elective surgery and emergency surgery has been shown to minimize disruptions and optimize efficiency for both patient groups.4 Having daily emergency lists improves access, and, in hospitals where use is a concern, half-days have been an effective alternative.4,17,18 Running rooms later into the evening or protecting time on the end of rosters are other approaches.17 At present, there is still no protected emergency time at our centre. Emergent cases currently go into the first available room, often disrupting the flow of the booked schedule and resulting in the cancellation or postponement of elective procedures.
An important component of implementing any strategy for the care of patients who require emergency surgery is to use an evidence-based classification system.5 At the time of this study, our centre used a 4-class system: class 1 (within ≤ 1 h), class 2 (within ≤ 6 h), class 3 (within ≤ 24 h) and class 4 (within ≤ 72 h), with no defined category for immediate procedures. Furthermore, there was no auditing of case classifications to ensure they were congruent with the patient’s diagnosis and status. It is recognized that, for some specific diagnoses, such as active bleeding, increased intracranial pressure and unresponsive shock secondary to conditions such as abdominal compartment syndrome, each passing minute between diagnosis and incision increases mortality risk.5,12 Looking at time to incision as an independent predictor of adverse outcomes, Clarke and colleagues12 found a 1% increase in mortality among patients with trauma for every 3-minute delay to laparotomy for intra-abdominal bleeding. Arguably, with a more robust prioritization system in place, perhaps some of our patients would have been classified differently, and this may have facilitated an expedited time to the operating room, with improvement in outcomes.
In many circumstances for surgical patients with complex conditions, the sicker the patient, the greater the difference between the time from booking to the patient entering the operating room, and the time from booking to incision. In the present study, we found no significant association between the time from booking to incision and mortality. However, the data did show that a number of patients at high risk for mortality had an “anesthetic time” (after arrival in the operating room and before incision) of more than an hour; the details about what this time was used for were not available. For some patients, particularly those at imminent risk of death, the anesthetic time may present in and of itself a risk to survival. However, for complex patients whose condition is stable (i.e., who are not actively bleeding, and do not have high intracranial pressure and/or unresponsive shock), in-room anesthetic preparation including ensuring appropriate access, volume status and product availability is crucial to optimizing the patient’s outcome. Surgery booking classification systems that differentiate patients who need an operation within minutes to prevent death and those who need to get to the operating room emergently within an hour, coupled with clear communication among the surgical, anesthetic and nursing teams, are crucial to efficient, safe surgical care.
Robust data capture of a surgical patient’s entire journey has shown other important components that influence outcomes. Process mapping has been used in emergency general surgery as well as cardiac surgery to isolate each segment of a patient’s experience, measure the times and look for significant variability between sequence and timing for different patients at each stage of their surgical journey.19,20 An emergency general surgery model of care is an organizational structure that provides protected operating time for surgical emergencies, as well as structures and processes designed to improve the care of patients with general surgical emergencies.21 Evidence from hospitals using the emergency general surgery model shows important benefits, including decreases in time to surgical evaluation, time to the operating room, length of stay, morbidity, mortality, cost and nighttime operating.15,22,23
Despite the compelling evidence of the benefit to patients, health care teams and health care systems of protecting surgical resources for adult urgent/emergent patients, there is very limited literature on the use of this practice for children.3 Our group previously reported significant increases in morbidity associated with repair of esophageal atresia/tracheoesophageal fistula and primary radical nephrectomy when performed after daytime working hours compared to within regular hours.24,25 It is not clear whether the increases in morbidity were related to factors associated with delay to operation or were secondary to system-related or fatigue-related factors. However, given the evidence, it seems clear that this group of children requires improved access and advocacy.
Although Canada is among the countries with the highest expenditure of health care dollars,26 its health care system ranks at the bottom in many outcomes, particularly those related to access for patients.26 The gravity of the crisis in access to surgical care in Canada is increasing: delays for patients who require elective surgery result in preventable deaths.6 Similarly, delays in emergency surgery are associated with an increased rate of preventable death.7 Urgent/emergency surgery and elective surgery seem to be in constant competition for a strained resource that is stretched beyond capacity, with patients ultimately paying the terrible price. Adults and children requiring emergency surgical care are arguably among the most vulnerable and least able to self-advocate of any patient in the entire health care system. The responsibility to advocate on their behalf and implement crucial changes for emergency surgical patients rests with each health care provider, administrator and the health authority, as well as the provincial and federal governments.
Evidence from other institutions has shown improvements in surgical access after internal audits and dissemination of results to the teams27; however, at our institution, despite multiple presentations of the current evidence and our own data, there have been challenges in realizing any substantial improvements. There have been some positive changes, however. A new evidence-based surgical prioritization system similar to that described by Kluger and colleagues5 has been adopted at our institution. There are now 5 priorities for urgent/emergent cases: E0 (immediate), E1 (< 1 h), E2 (< 6 h), E3 (< 12 h) and E4 (< 48 h). In addition, when our institution moved to a new hospital, in 2018, we carried out a prospective analysis of all emergency operations, collecting data on reasons for delay and whether the delay was deemed to have negatively affected patient outcome. Data for 12 months included more than 1300 cases, with an average of more than 4 urgent/ emergent (E0–E4) cases per day and 1–2 emergent (E0 or E1) cases per week. Not only were class 1 cases still most likely to be delayed, but also there was a significant association between procedure-specific major morbidity and delay to the operating room. The most common reason for delay was lack of an available operating room (unpublished data, 2018). These more recent data were similarly shared with the operating room teams and leadership, but no major organizational changes occurred. Given the persistent unacceptable proportion of E0 and E1 patients still experiencing a delay to surgery, it was felt that sharing the data for patients from 2011 to 2016 more widely would prompt our hospital, government and other pediatric institutions to address any organizational barriers to access for urgent and emergent surgery.
There are now additional threats to this vulnerable patient population. Elective surgery recovery efforts in the shadow of COVID-19 have been underway across the country. These efforts have often included booking elective cases until the evening and possibly even during the night, as well as weekends.28 Although there has been important advocacy to prioritize children’s elective surgery during the pandemic,29 recovery efforts should not further marginalize infants and children who require emergent or urgent surgical care. The omicron variant forced shutdown of elective surgery in many provinces across Canada,30 and the threat of subsequent COVID-19 waves affecting surgical access looms. With expectations of staffing shortages added to the mounting burden of patients experiencing delayed surgical care,31 intentional protection of resources for emergency surgery for children must be initiated and sustained.
Limitations
Given our study’s retrospective nature, it is very difficult to ascertain the reasons for delay in patients’ getting to the operating room. The determination of whether delay was a potential factor leading to morbidity/mortality is challenging, especially in retrospect, without having input from the surgical team caring for the patient. Attributable morbidity and mortality is a more robust method and typically can be used when there is a relatively uniform population experiencing (or not) a specific event or exposure with the use of matched cohorts.32 To our knowledge, there is no way of determining attributable morbidity or mortality with such a heterogeneous population as in the current study. In addition, it is unknown whether some of the patients who arrived in the operating room within 1 hour should have undergone surgery sooner because of immediately life-threatening conditions (such as bleeding or increased intracranial pressure). It is widely agreed that these patients are at imminent risk of death and require surgery within minutes to save their lives.5,12 The SNAP II and PRISM III scoring systems are not typically used to predict mortality after surgery; rather, the scores are often calculated soon after birth and within hours of admission to the pediatric intensive care unit, respectively. Given this, we also used ASA classification of 3 or higher for patients whose risk level may not have been captured by the scoring systems. The ASA classification is a robust measure to stratify risk immediately before surgery, and a classification of 3 or higher has been shown to reliably predict increased postoperative morbidity and mortality.33 Furthermore, there were likely some patients who were not appropriately categorized and could have safely had their surgery delayed past the 1-hour time frame. The present study focused only on the time from booking to the patient entering the operating room, and the time from booking to incision; thus, all data on times and events from the patient’s initial assessment to booking were unknown and may have had a significant impact on the patient’s outcome.
We have gathered only a small portion of the patient journey, and to make fully informed, meaningful improvements, data from each step need to be collected. In addition, and importantly, we were unable to determine why patients were delayed to the operating room. At the time of the study, the operating rooms were in a building constructed in 1984, and lack of physical space was believed to be a major causative factor by many with whom these data were shared. Finally, the study data date back more than 5 years and relate to surgical access in our old hospital, which had only 7 operating rooms. The results may not be generalizable to the outcomes of patients in the new building, which has 11 operating rooms, or to other institutions with greater operating room capacity.
Conclusion
In our study, an unacceptable proportion of infants and children who were in a surgical crisis and at immediate risk for loss of a limb or organ, or death did not receive timely surgical care. At the federal and provincial levels, action must be taken to prioritize, be accountable to and advocate for emergency surgery patients. Our most vulnerable surgical patients are at great risk of experiencing barriers to surgical access; without commitment, measurement and accountability at all levels of health care, unintended harm will continue.
Acknowledgements
The authors thank Maryam Noparast for statistical support, and the Office of Pediatric Surgical Evaluation and Innovation at BC Children’s Hospital for their support of this project.
Footnotes
Presented at the 50th Annual Meeting of the Canadian Association of Paediatric Surgeons, Sept. 26–29, 2018, Toronto, Ont.
Competing interests: None declared.
Contributors: S.A. Butterworth, S. Kim and K. Afshar designed the study. S.A. Butterworth, I. Zivkovic and S. Kim acquired the data, which S.A. Butterworth and K. Afshar analyzed. S.A. Butterworth wrote the manuscript, which S.A. Butterworth, I. Zivkovic, S. Kim and K. Afshar critically revised. All authors gave final approval of the article to be published.
- Accepted August 23, 2022.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.