


Abstract
Background: Although uncommon, pneumothorax is a potentially serious complication following open reduction and internal fixation (ORIF) of clavicle fractures. In many centres it is routine practice to obtain postoperative chest radiographs following ORIF of clavicle fractures to assess for iatrogenic pneumothorax. Given the need to contain health care costs, the low sensitivity for detecting small pneumothorax and a desire to decrease patient radiation exposure, the practice of ordering chest radiographs following ORIF of clavicle fractures may be unnecessary.
Methods: All patients undergoing ORIF of clavicle fractures with plate and screw fixation at Kingston Health Sciences Centre between April 2009 and June 2020 were identified from the Discharge Abstract Database (inpatient) and National Ambulatory Care Reporting System (outpatient) using relevant Canadian Classification of Health Intervention procedure codes. Charts were manually reviewed to confirm diagnosis and procedure, and patients with preoperative pneumothorax were excluded. The frequency of postoperative chest radiograph and pneumothorax detection were calculated.
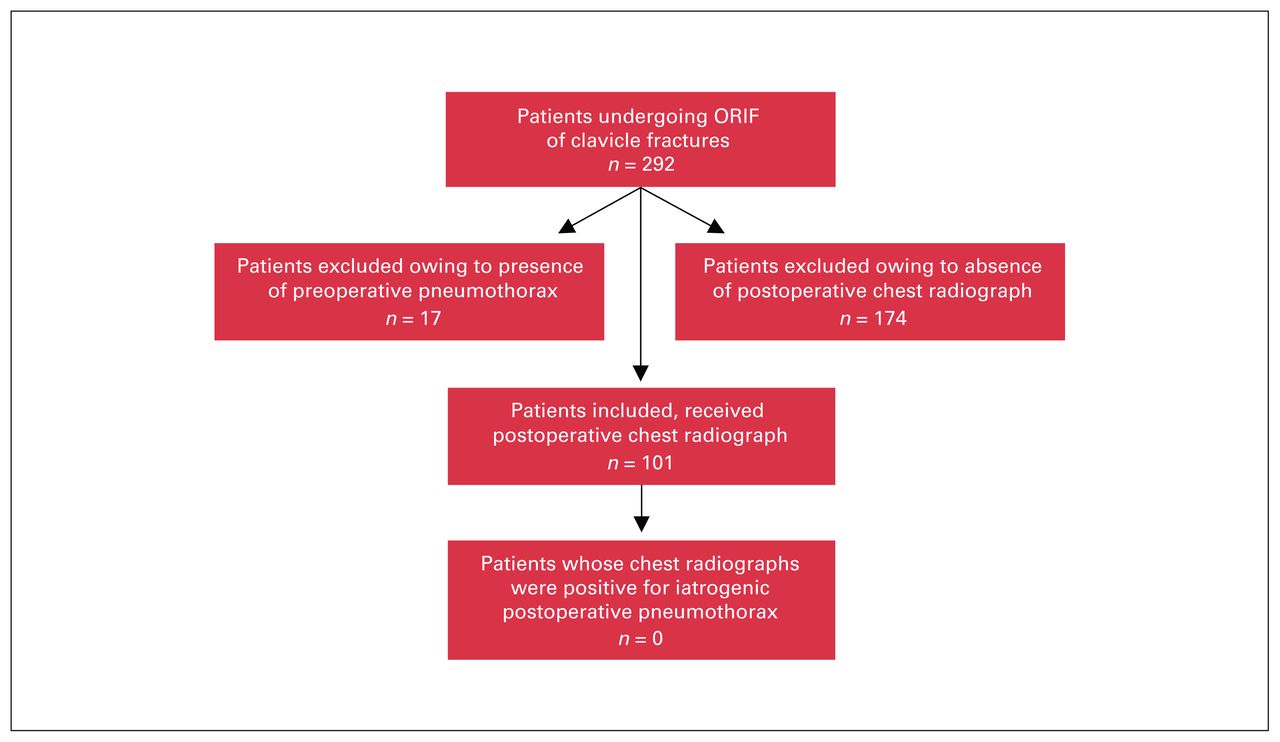
Results: Among the 292 patients who underwent ORIF of clavicle fractures during the study period, 17 were excluded for having a pneumothorax on preoperative chest radiograph. Of the remaining 275 patients, 101 (36.7%) had postoperative chest radiographs, of whom none were found to have postoperative iatrogenic pneumothorax.
Conclusion: Since 2009, the rate of routine postoperative chest radiography following ORIF of clavicle fractures is 36.7% at our centre. During this time period, none of the 101 patients who had postoperative chest radiographs had a postoperative iatrogenic pneumothorax. To our knowledge, this is the largest series of patients available, and our findings confirm those of several smaller studies. Owing to the low rate of postoperative iatrogenic pneumothorax, we conclude that postoperative chest radiography is unnecessary following ORIF of clavicle fractures.
Clavicle fractures make up about 2%–4% of all fractures, with an incidence of 64 per 100 000 in the general population and a preponderance of injuries in male patients (70%–80%), most commonly as a result of road traffic incidents, including motor vehicle collisions and bicycle injuries.1–3 Historically, the majority of clavicle fractures have been treated nonoperatively.4 However, non-operative management has come into question in recent years, with cited nonunion rates as high as 24%.5 Interestingly, a meta-analysis of 15 randomized controlled trials found no difference in the risk of secondary operation between nonoperative and operative patients, although there was a 40% improvement in functional outcome scores in patients who received operative compared with nonoperative treatment.6 Currently accepted indications for open reduction and internal fixation (ORIF) of midshaft fractures include open fracture, substantial shortening (> 2 cm), displacement (> 100%), or comminution and symptomatic nonunion.7–9 The overall frequency of surgical intervention for clavicle fractures is dependent on clinical site, with numbers between 1% and 12% reported.10,11
The clavicle has several surrounding structures that may be damaged following acute fracture or during surgical intervention, including the subclavian artery, brachial plexus and internal jugular vein. Furthermore, the apex of the lung lies posterior to the medial third of the clavicle. Owing to this proximity, pneumothorax, although uncommon, is a possible complication of clavicle fracture. We identified several published English-language case reports detailing such incidences.12–21 The proximity of the clavicle to the apex of the lung also means that an iatrogenic pneumothorax induced perioperatively during ORIF of clavicle fractures is possible. Three case reports were identified from 2014 to 2020 where a definitive iatrogenic pneumothorax was found following ORIF of clavicle fractures.22–24 Currently, it is common practice in many centres to obtain a postoperative chest radiograph following ORIF of clavicle fractures to rule out iatrogenic pneumothorax, although studies offer limited support for this practice; to date a single study involving 89 patients has been performed and found no instances of postoperative iatrogenic pneumothorax.25 We aimed to determine whether routine postoperative chest radiography to identify iatrogenic pneumothorax following ORIF of clavicle fractures is a useful practice.
Methods
All patients undergoing ORIF of clavicle fractures with plate and screw fixation at our level I trauma centre between April 2009 and June 2020 were identified from the Discharge Abstract Database (inpatient) and National Ambulatory Care Reporting System (outpatient) using relevant Canadian Classification of Health Intervention procedure codes. We manually reviewed patient charts to confirm clavicle fracture diagnosis and receipt of ORIF. Patient demographics and clinical characteristics including age, laterality of injury, treatment setting and mechanism of injury were recorded. Patients with preoperative pneumothorax were excluded. The frequency of postoperative chest radiography and pneumothorax detection were calculated. We obtained institutional ethics approval (IRB 00001173).
Results
Patient characteristics are reported in Table 1. Between April 2009 and June 2020, a total of 292 clavicle fractures treated with ORIF were identified from the databases. Among the 292 patient charts reviewed, 17 were excluded for the presence of pneumothorax on preoperative chest radiographs. Of the remaining 275 patients, 101 (36.7%) received postoperative chest radiographs, of whom none were found to have pneumothorax. Importantly, manual review of the data set showed postoperative chest radiographs were obtained for patients who underwent surgery for both traumatic and atraumatic indications. A summary of the exclusion process can be found in Figure 1. One patient with polytrauma and multiple ipsilateral proximal rib fractures was found to have pneumothorax 24 hours after surgery on a chest radiograph obtained for chest pain and shortness of breath. However, immediate postoperative radiographs had been negative for pneumothorax, suggesting a delayed pneumothorax associated with rib fracture.14,26,27
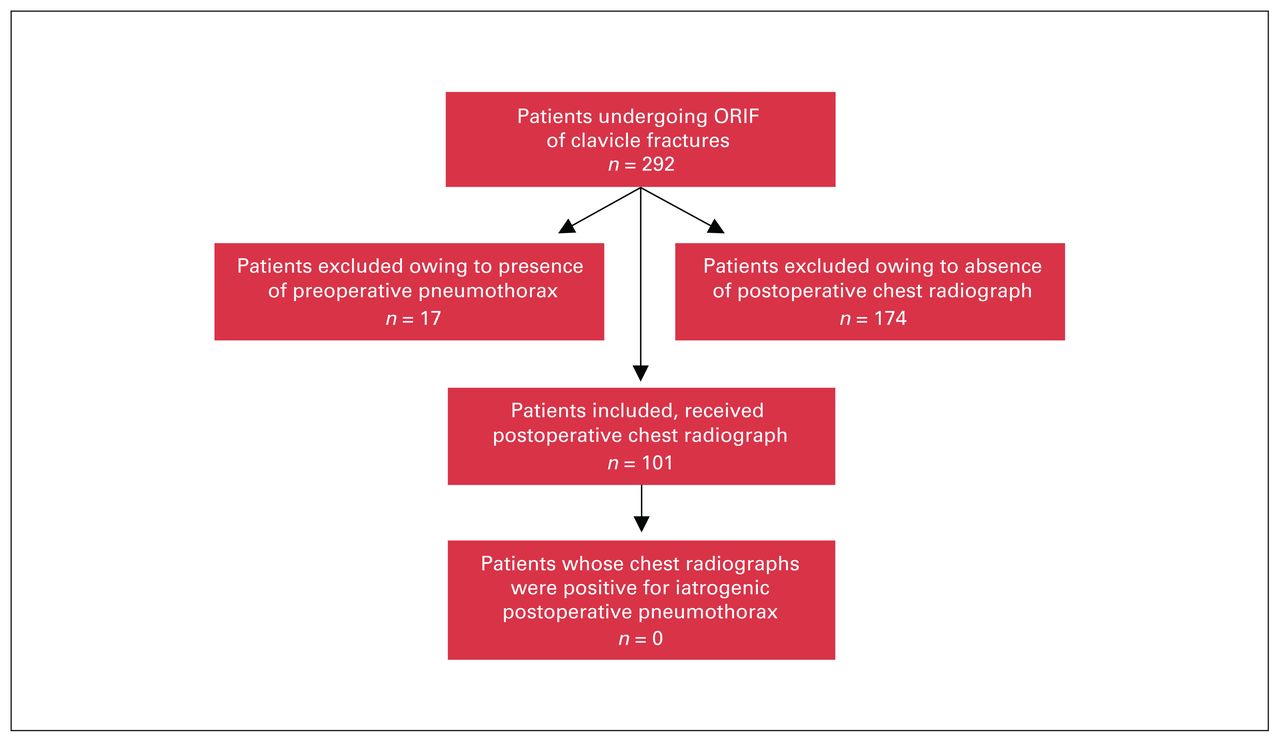
Flow diagram for inclusion and exclusion of patients. ORIF = open reduction and internal fixation.
Baseline patient characteristics
Discussion
Since 2009, the rate of routine postoperative chest radiographs following ORIF of clavicle fractures is 36.7% at our centre. In a similar study published in 2019, 86.8% of patients at another institution underwent postoperative chest radiography.25 This difference (36.7% v. 86.8%) may be explained by a difference in fiscal policy between American and Canadian institutions. Indeed, Americans spend nearly twice as much per capita on health care, a trend that has sparked the birth of the Choosing Wisely campaign, established in 2012.28,29 This initiative by the American Board of Internal Medicine aims to reduce costs by identifying unnecessary medical tests and procedures and reducing their use. A Canadian Choosing Wisely campaign was started in 2014 and aims for increased fiscal responsibility among medical practitioners.30 With this in mind, we aimed to explore whether chest radiographs following ORIF of clavicle fractures continued to be useful at our institution.
During the study period, none of the 101 patients who underwent ORIF of clavicle fractures and received postoperative chest radiographs had postoperative pneumothorax. To our knowledge, this is the largest series of patients available, and our findings confirm those of 2 smaller studies.25,31 Shubert and colleagues25 found no iatrogenic pneumothorax in a series of 89 patients undergoing ORIF of clavicle fractures. A second series (n = 76), presented at the Orthopedic Trauma Association general meeting in 2015, found no postoperative pneumothorax in patients who did not have preoperative pneumothorax, lung injury or rib fracture (0/23).31 One large study of 1350 patients reported a pneumothorax rate of 1.2% following ORIF of clavicle fractures, but did not distinguish between preoperative and postoperative pneumothorax.32 Similarly, a published query of the National Surgical Quality Improvement Program database identified no patients with postoperative pneumothorax.33 Given the subtle, often subclinical nature of pneumothorax, this database query may not have been appropriately powered to identify instances of pneumothorax, and a manual chart review approach is likely to achieve more accurate results. Estimates of the sensitivity of chest radiographs for pneumothorax vary between 20% and 29%, which further reduces the usefulness of this procedure as a routine test following ORIF of clavicle fractures.34,35
Limitations
This study has several limitations, most notably relatively small numbers. However, to our knowledge, it is the largest data set available to date, and this clinical question does not lend itself well to larger database examinations. The practice of ordering postoperative chest radiographs following ORIF of clavicle fractures was not universal, as it reflected surgeon preference rather than institutional policy. Manual review of patient charts did not show any complications associated with missed pneumothoraces in patients who did not undergo postoperative radiography of the chest.
Conclusion
Patients undergoing ORIF of clavicle fractures are at very low risk of iatrogenic pneumothorax. This study provides evidence for the discontinuation of routine postoperative chest radiographs following ORIF of clavicle fractures. Although chest radiographs are not a particularly expensive diagnostic procedure, in the spirit of Choosing Wisely, any investigation that does not offer demonstrable benefit should not be pursued routinely. We conclude that the practice of obtaining postoperative chest radiographs following ORIF of clavicle fractures is unnecessary and should be abandoned.
Footnotes
Competing interests: None declared.
Contributors: J. Hobson and S.M. Mann designed the study. S.M. Mann acquired the data, which J. Del Papa analyzed. J. Del Papa wrote the article, which J. Hobson and S.M. Mann reviewed. All authors approved the final version to be published.
- Accepted May 24, 2023.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use) and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue

{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.