


Abstract
Background: Minimally invasive sacroiliac joint (MISIJ) fusion is a surgical option to relieve SIJ pain. The aim of this systematic review and meta-analysis was to compare MISIJ fusion with triangular titanium implants (TTI) to nonoperative management of SIJ dysfunction.
Methods: We searched MEDLINE, Embase, and the Cochrane Central Register of Controlled Trials. We included prospective clinical trials that compared MISIJ fusion to nonoperative management in individuals with chronic low back pain attributed to SIJ dysfunction. We evaluated pain on visual analogue scale, Oswestry Disability Index (ODI) score, health-related quality of life (HRQoL) using the 36-Item Short Form Health Survey (SF-36) physical component (PCS) and mental component summary (MCS) scores, patient satisfaction, and adverse events.
Results: A total of 8 articles representing 3 trials that enrolled 423 participants were deemed eligible. There was a significant reduction in pain score with MISIJ fusion compared with nonoperative management (standardized mean difference [SMD] −1.71, 95% confidence interval [CI] −2.03 to −1.39). Similarly, ODI scores (SMD −1.03, 95% CI −1.24 to −0.81), SF-36 PCS scores (SMD 1.01, 95% CI 0.83 to 1.19), SF-36 MCS scores (SMD 0.72, 95% CI 0.54 to 0.9), and patient satisfaction (odds ratio 6.87, 95% CI 3.73 to 12.64) were significantly improved with MISIJ fusion. No significant difference was found between the 2 groups with respect to adverse events (SMD −0.03, 95% CI −0.28 to 0.23).
Conclusion: Our analysis showed that MISIJ fusion with TTI shows a clinically important and statistically significant improvement in pain, disability score, HRQoL, and patient satisfaction with a similar adverse event profile to nonoperative management in patients with chronic low back pain attributed to SIJ dysfunction.
Sacroiliac joint (SIJ) dysfunction is a degenerative condition that is considered a major cause of low back pain.1 About 15%–30% of cases of low back pain in patients presenting in the outpatient setting are attributed to the SIJ dysfunction.2,3 The condition is often associated with impaired physical function and psychological distress, resulting in a substantial effect on health-related quality of life (HRQoL).4 The diagnosis of SIJ dysfunction is difficult, as the clinical presentation often mimics that of other conditions of the lumbar spine or the hip joint. The proactive physical examination tests that provoke pain originating from the SIJ can differentiate SIJ dysfunction from other causes of low back pain.5
Nonoperative measures represent the first line of management for SIJ dysfunction and include medical therapy, physical therapy, intra-articular injections, and radiofrequency ablation.6–8 When nonoperative management fails to relieve symptoms, SIJ fusion is a surgical option. Open SIJ fusion, developed in the early 1920s, showed modest to good efficacy in relieving chronic SIJ pain.9 However, open SIJ fusion is a demanding procedure for both the treating physician and the patient; it has been associated with a long hospital stay, substantial blood loss, and a high complication rate.10,11 The introduction of minimally invasive SIJ (MISIJ) fusion heralded a reduction in postoperative complications with greater efficacy than the open technique.12,13 Currently, MISIJ fusion is replacing the open technique for chronic, nontraumatic SIJ pain, accounting for more than 90% of SIJ fusion procedures.14 Triangular titanium implant (TTI) is currently the most widely used system for MISIJ fusion. The evidence on the efficacy of SIJ fusion using a TTI system was initially obtained from case series15–21 and combined multicentre analysis.22 Recently, 3 clinical trials assessing the efficacy of a TTI system have been published.23–25 To our knowledge, no systematic review of prospective clinical trials has been conducted. As such, the aim of this systematic review and meta-analysis was to compare MISIJ fusion using TTI with nonoperative management for SIJ dysfunction with respect to pain, disability, and HRQoL.
Methods
This systematic review was performed according to a prespecified protocol registered at PROSPERO (CRD42021288388). The reporting of this review is in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) checklist.26
Data sources and study selection
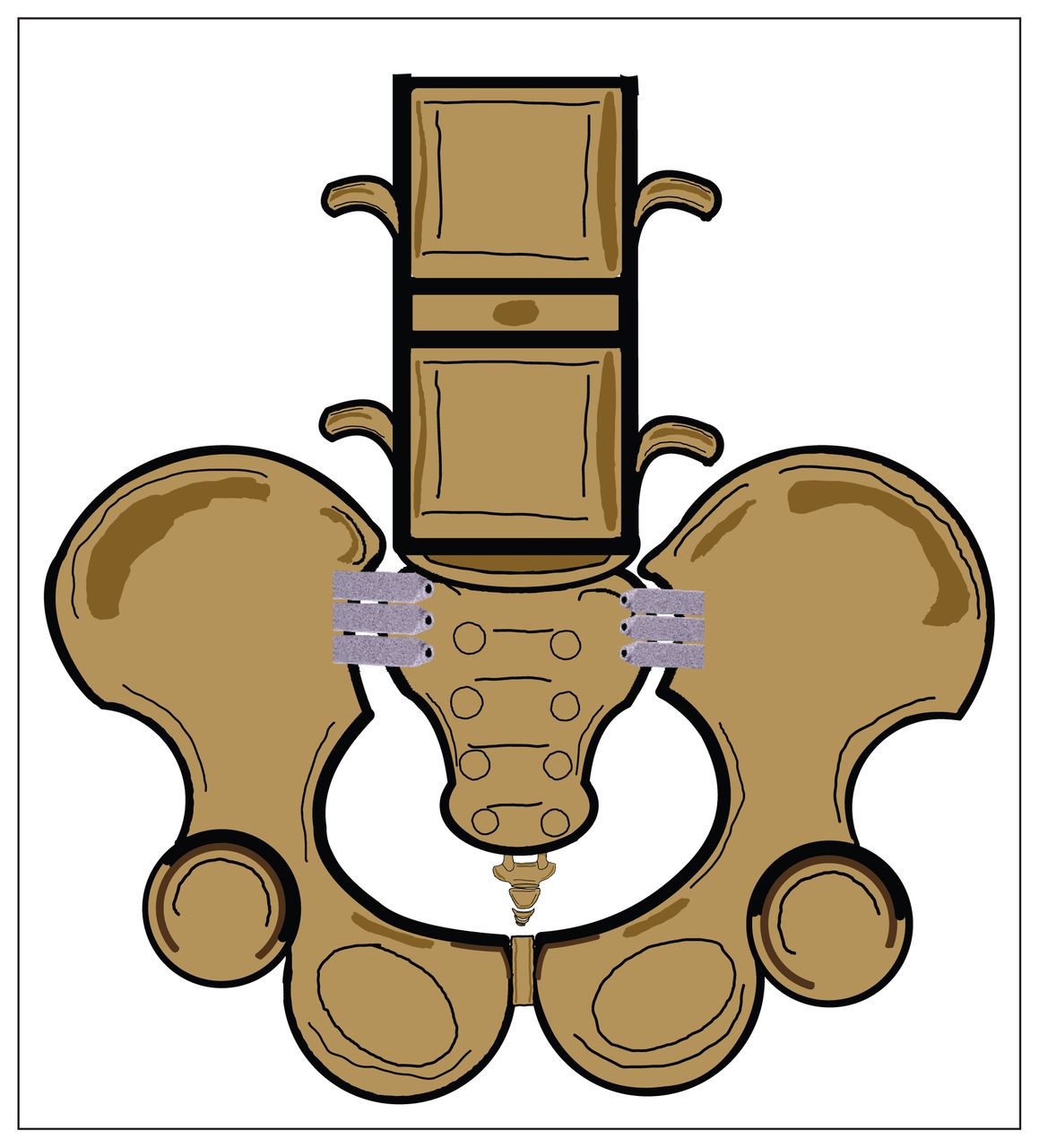
We searched MEDLINE, Embase, and the Cochrane Central Register of Controlled Trials (CENTRAL) from inception to April 2023. To be eligible for inclusion, studies had to meet the following criteria: the study design was a prospective clinical trial; the population included adult patients with a confirmed diagnosis of SIJ dysfunction; the intervention group underwent MISIJ fusion with TTI (Figure 1); the comparison group received nonoperative management of SIJ dysfunction; the study reported outcomes including pain on visual analogue scale (VAS), Oswestry Disability Index (ODI) score, HRQoL using the 36-Item Short Form Health Survey (SF-36) and EuroQoL (EQ-5D), patient satisfaction, opioid use and adverse events; and the study was published in English. We excluded trials studying low back pain attributed to causes other than SIJ dysfunction or trials in which MISIJ fusion involved devices other than TTI. We searched the references and citations of the included trials for relevant studies. The search terms used can be found in Appendix 1, available at canjsurg.ca/lookup/doi/10.1503/cjs.004523/tab-related-content. Three independent pairs, in duplicate, screened titles, abstracts, and full texts. We resolved disagreements by discussion and consensus, or arbitration by a third reviewer when needed.
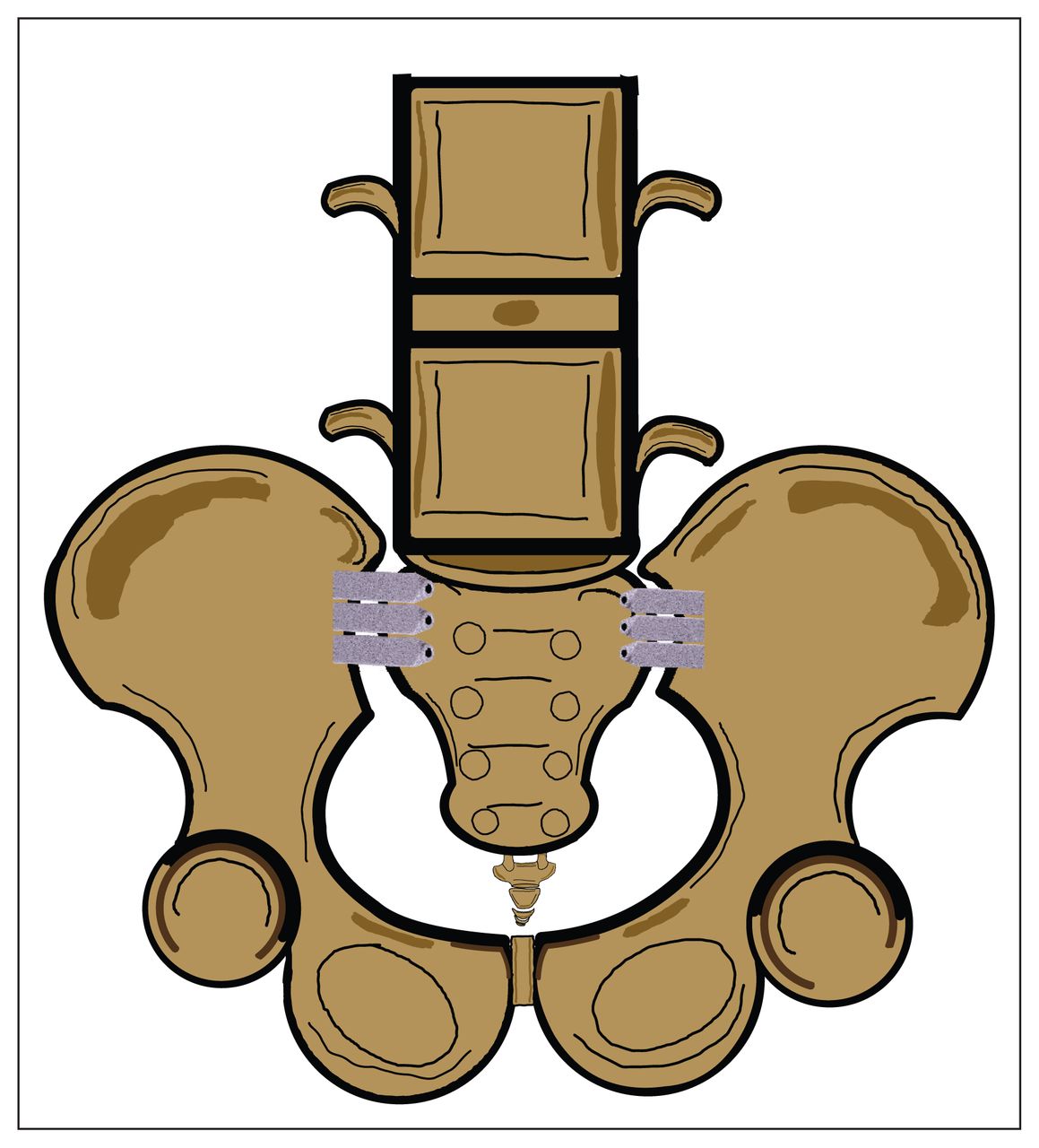
Illustration of minimally invasive sacroiliac joint fusion with triangular titanium implants.
Data extraction and risk of bias
Three independent pairs of reviewers extracted data, in duplicate, using a predesigned data abstraction form. Reviewers extracted the following data: name of the first author, year of publication, trial registration number, number of participants in each arm, gender, mean age, mean body mass index (BMI), ambulatory status, history of prior lumbar fusion, SIJ dysfunction diagnostic criteria used in each trial, and the desired outcomes reported by each trial. Disagreements were resolved by discussion and consensus or using a third reviewer if needed. Reviewers used the modified Cochrane Collaboration assessment tool to assess the risk of bias of eligible studies and classified studies into the following categories: high risk of bias, some concerns, or low risk of bias.27
Meta-analysis
We performed the meta-analysis in RevMan (Review Manager) version 5.3 (Cochrane Collaboration) using the random-effects model with inverse variance for the continuous and dichotomous outcomes. We used 95% as a confidence level and p < 0.05 as a threshold for statistical significance.
We report continuous outcomes (i.e., pain on VAS score, ODI score, SF-36 score, EQ-5D score, mean number of adverse events) as standardized mean differences (SMDs) with 95% confidence intervals (CIs). The dichotomous outcomes (i.e., patient satisfaction, medication use) are presented as odds ratios (ORs) with 95% CIs. We assessed heterogeneity using the χ2 test (p ≤ 0.1) or I2 test (≥ 50% indicates significant heterogeneity), and visually by inspecting forest plots. When 10 or more studies were included in a meta-analysis, we assessed publication bias by visual inspection of a funnel plot.28,29 We sought to perform a subgroup analysis based on different follow-up periods (i.e., 1, 3, 6, 12, and 24 months).
Quality of evidence
We used the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) approach to assess the quality of evidence.30 Reviewers assessed the quality of evidence for each outcome and classified the quality of evidence as high, moderate, low, or very-low.
Results
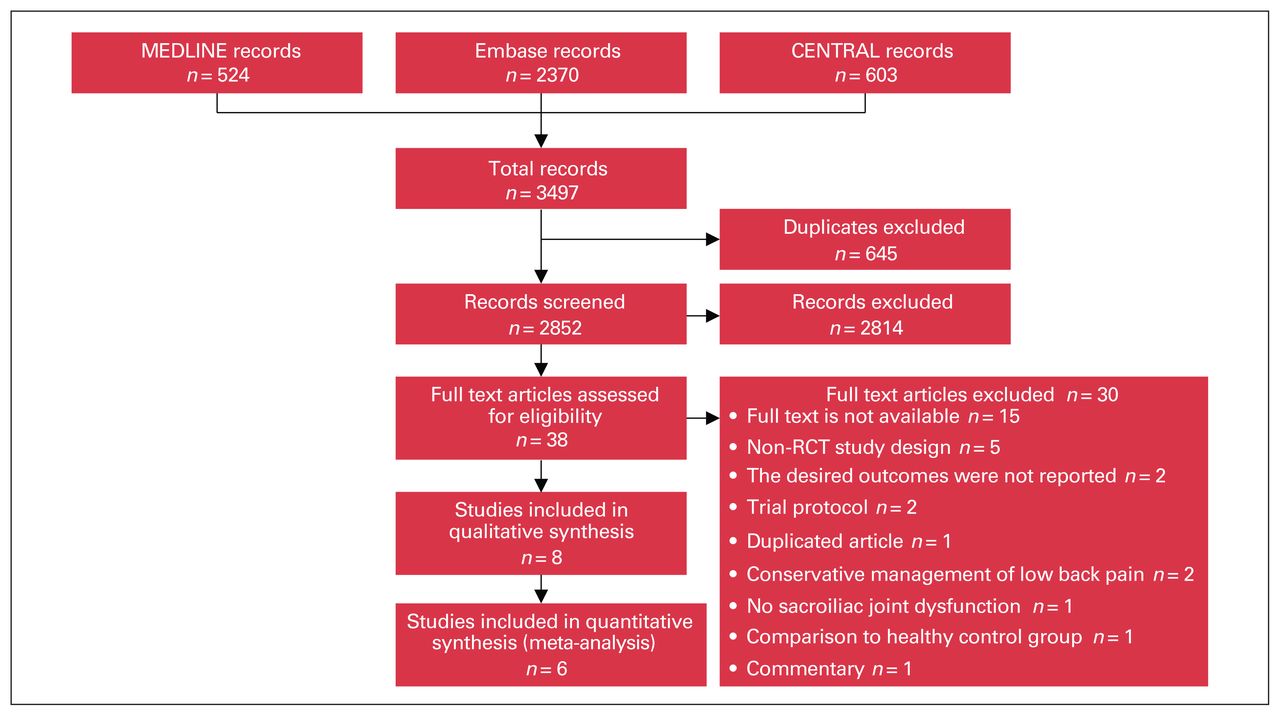
Our search identified a total of 3497 records (Figure 2). After removing the duplicates, 2852 titles were screened. Thirty-eight articles were eligible for full text review, of which 8 articles representing 3 trials met our eligibility criteria and were included in the review.23–25,31–35 The 8 articles were follow-up reports of the 3 original clinical trials. Of the 8 articles, 6 were included in the quantitative analysis, and 2 did not provide enough data for the analysis. 32,35 The findings of these 2 articles are reported narratively. The excluded studies, along with the reasons for exclusion, are summarized in Appendix 1, Table 1.
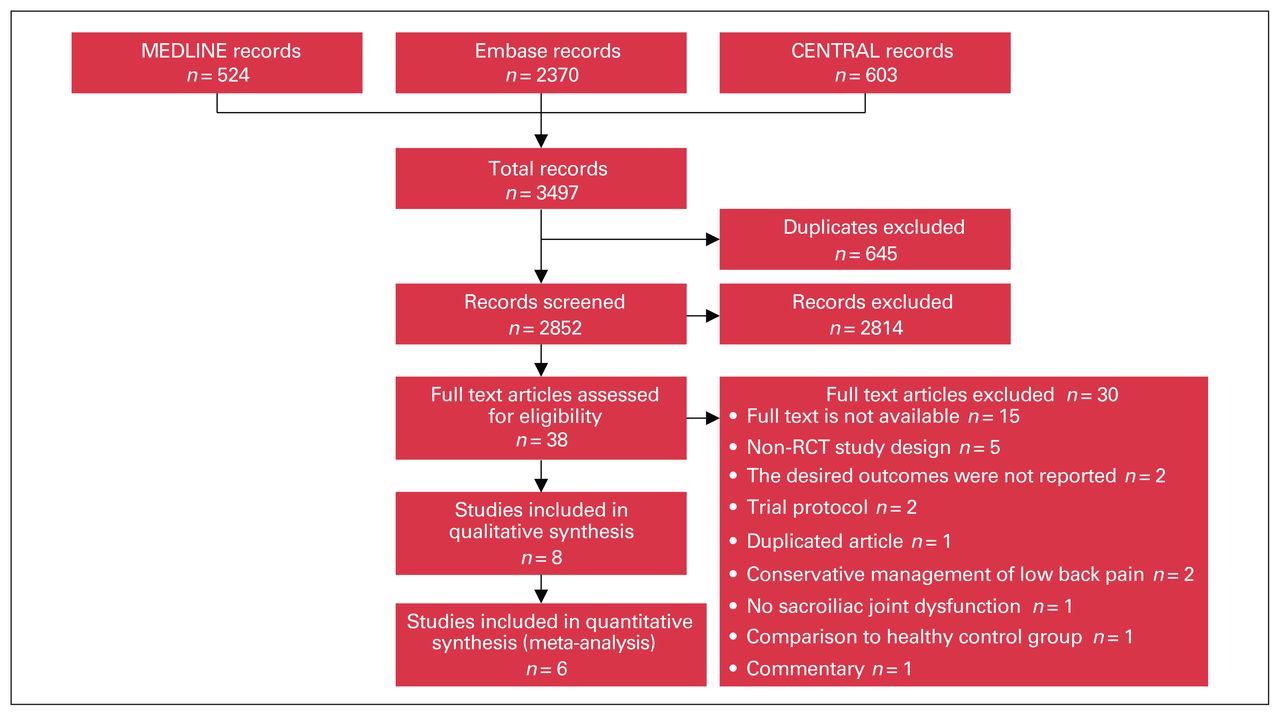
Literature search and selection of studies comparing minimally invasive sacroiliac joint fusion to nonoperative management. RCT = randomized controlled trial.
Description of the studies
The studies incldued a total of 423 participants, 154 (36.41%) of whom underwent MISIJ fusion and 97 (22.93%) of whom received nonoperative management. The remaining 172 (40.66%) participants underwent MISIJ fusion, and their outcomes were compared with their baseline nonoperative management. Of those who received MISIJ fusion, 268 (82.21%) underwent unilateral and 58 (17.79%) underwent simultaneous or staged bilateral MISIJ fusion. Most of the participants were female (70.45%) and ambulatory without assistance (67.38%) (Table 1). The weighted mean age was 50.16 (range 49.4–50.9) years and 50.50 (range 46.7–54) years in the MISIJ fusion and nonoperative groups, respectively. The weighted mean BMI was 28.77 (range 26.5–30.3) kg/m2 and 29.18 (range 27.6–30.6) kg/m2 in the MISIJ fusion and nonoperative groups, respectively (Appendix 1, Table 2).
Characteristics of the included studies comparing minimally invasive SIJ fusion to nonoperative management
The nonoperative management plan consisted of providing the optimal medical therapy for pain control, as directed by the site investigator; personalized physical therapy; patient education with adequate information and reassurance; and cognitive behavioural therapy. The MISIJ fusion was performed using a TTI implant system with a total of 2–4 TTI implants placed across the SIJ. The specific diagnostic criteria for SIJ dysfunction adopted by each of the included studies are presented in Table 2.
Diagnostic criteria and treatment of SIJ dysfunction in 8 studies representing 3 randomized controlled trials
Risk of bias and quality of evidence
The results of the risk of bias assessment for the individual studies can be found in Appendix 1, Figures 1 and 2. The risk of bias was low in all but 1 of the trials,25 which had a high risk of bias arising from a randomization concern. Additionally, as no outcome was reported by more than 10 studies, the funnel plot assessment was not performed. The rating for all outcomes according to GRADE criteria can be found in Appendix 1, Figure 3.
Pain on visual analogue scale
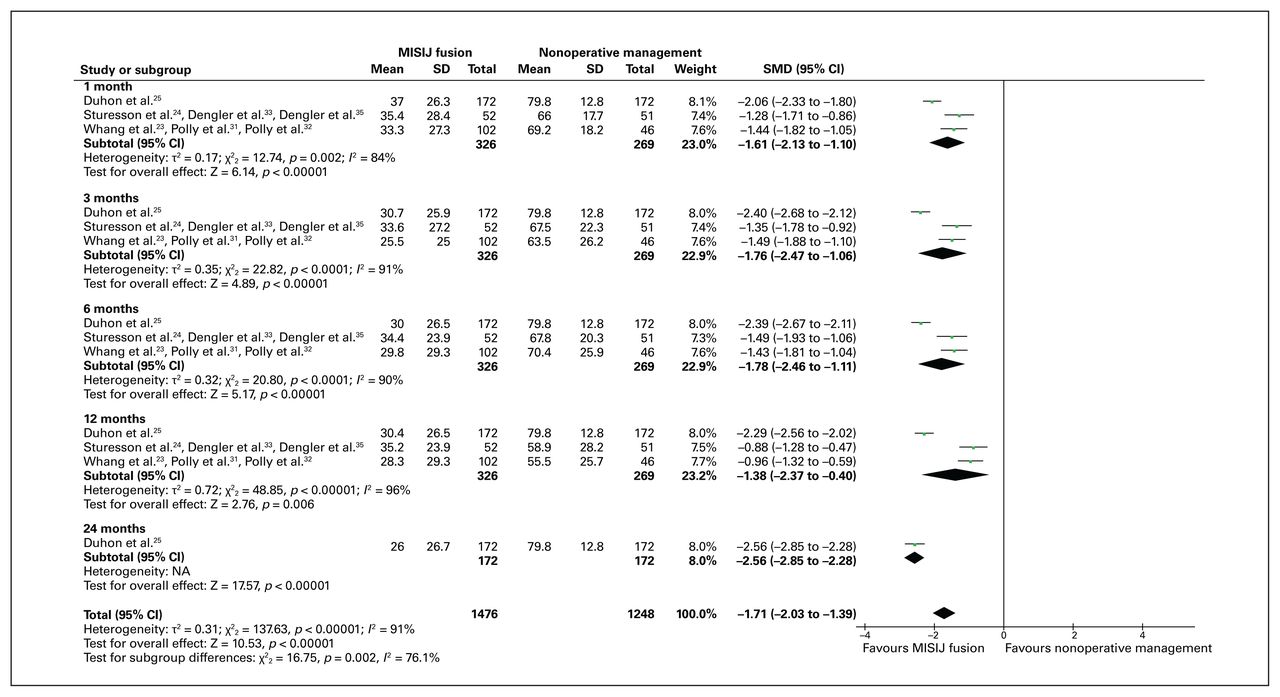
All 3 trials reported data on pain score, and all but 2 articles32,35 were included in our analysis.23–25,31,33,34 The weighted average pain score was 31.53 (range 25.5–37) and 70.95 (range 55.5–79.8) in the MISIJ fusion and nonoperative groups (weighted mean difference [WMD] −39.42), respectively. There was a significant reduction in the overall pain score with MISIJ fusion compared with nonoperative management (SMD −1.71, 95% CI −2.03 to −1.39, p < 0.00001, I2 = 91%, low-quality evidence). Similarly, the subgroup analysis showed a significantly lower pain score in favour of MISIJ fusion at 1, 3, 6, 12, and 24 months (Figure 3). The 2 articles that could not be included in the meta-analysis showed a significant improvement in pain score in favour of the MISIJ fusion at 24 months.32,35
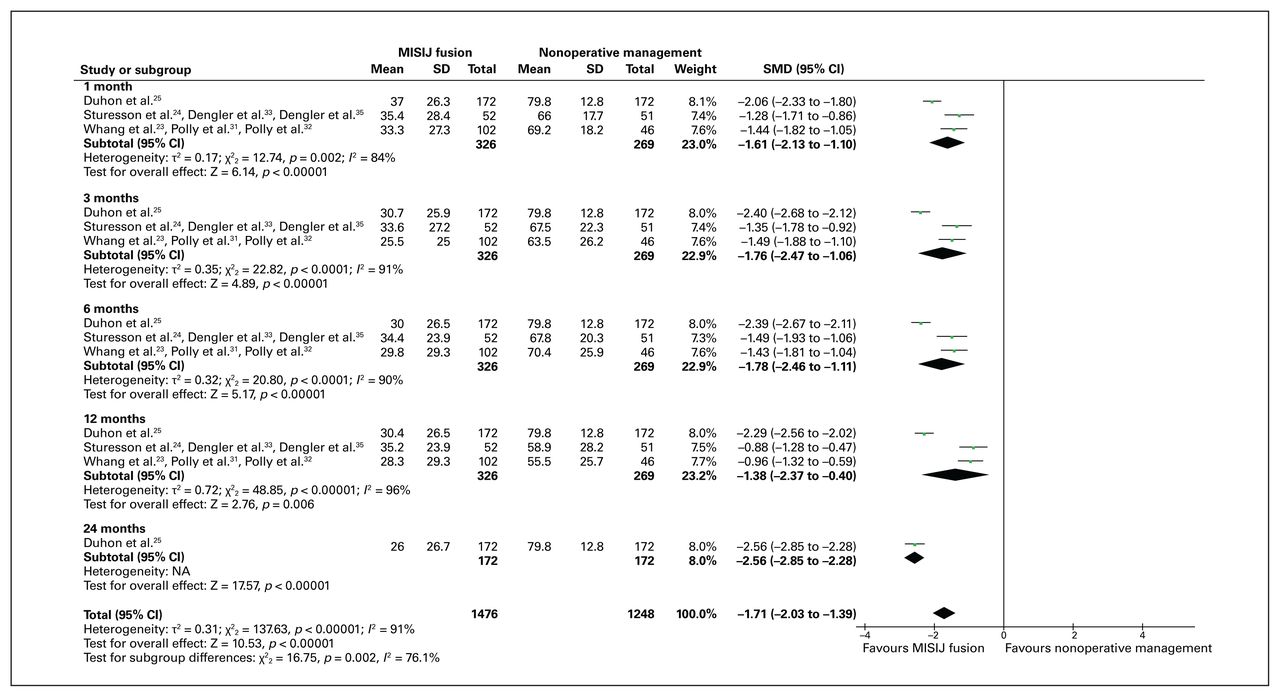
Pain score favouring minimally invasive sacroiliac joint (MISIJ) fusion over nonoperative management. CI = confidence interval; NA = not applicable; SMD = standardized mean difference.
Oswestry Disability Index score
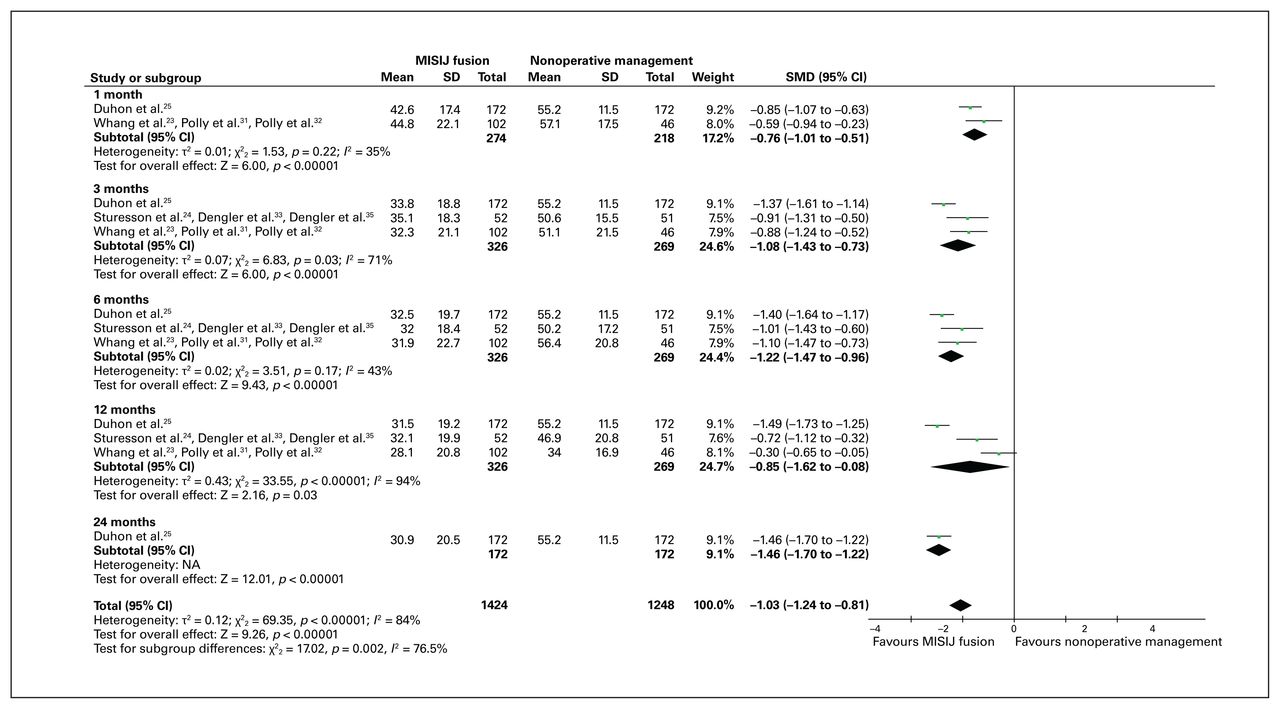
All 3 trials reported data on ODI score, and all but 2 articles32,35 were included in our analysis.23–25,31,33,34 The weighted average ODI score was 34.03 (range 28.1–44.8) and 52.11 (range 34–57.1) in the MISIJ fusion and nonoperative groups (WMD −18.11), respectively. There was significant improvement in the overall ODI score with MISIJ fusion compared with nonoperative management (SMD −1.03, 95% CI −1.24 to −0.81, p < 0.00001, I2 = 84%, low-quality evidence). Similarly, the subgroup analysis showed a significantly better ODI score in favour of the MISIJ fusion at 1, 3, 6, 12, and 24 months (Figure 4). The 2 articles that could not be included in the meta-analysis showed a significant improvement in ODI score in favour of the MISIJ fusion at 24 months.32,35
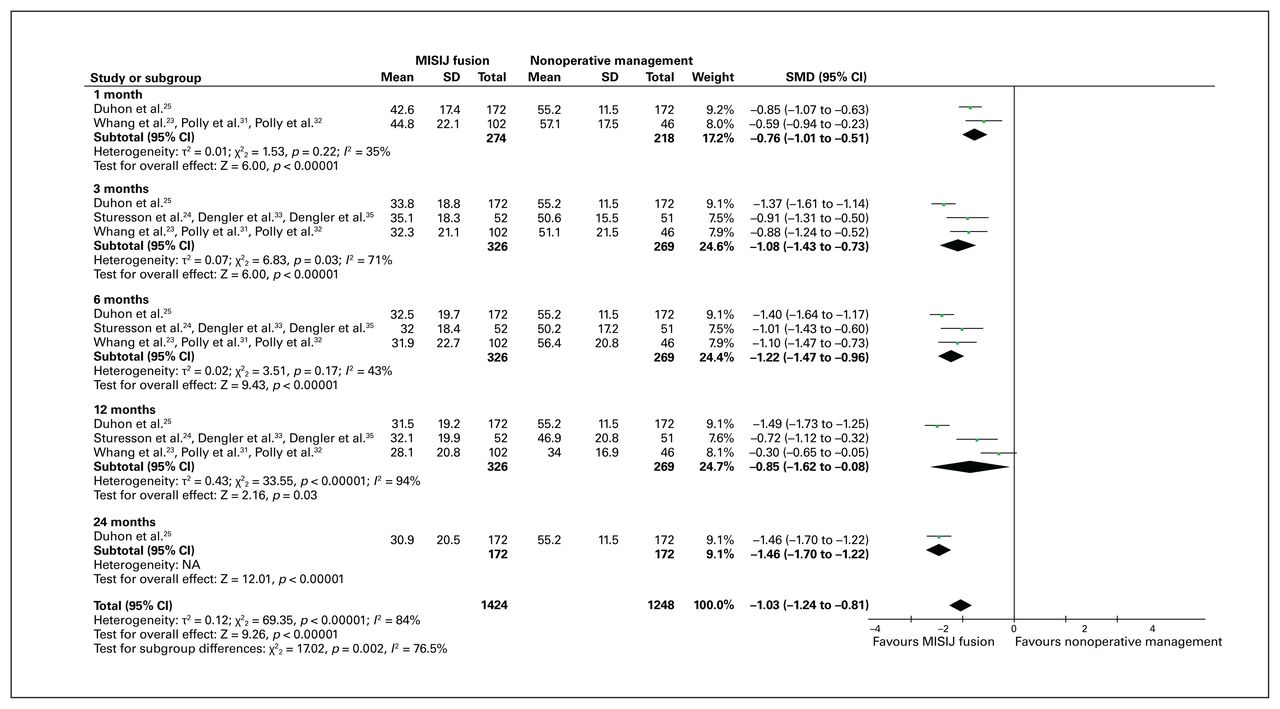
Oswestry Disability Index score favouring minimally invasive sacroiliac joint (MISIJ) fusion over nonoperative management. CI = confidence interval; NA = not applicable; SMD = standardized mean difference.
36-Item Short Form Health Survey score
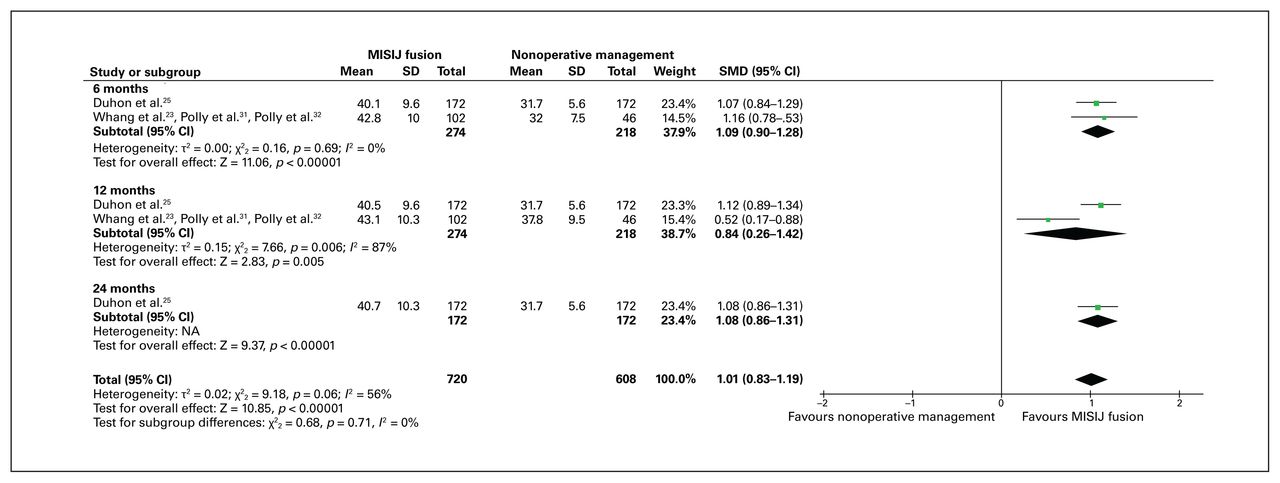
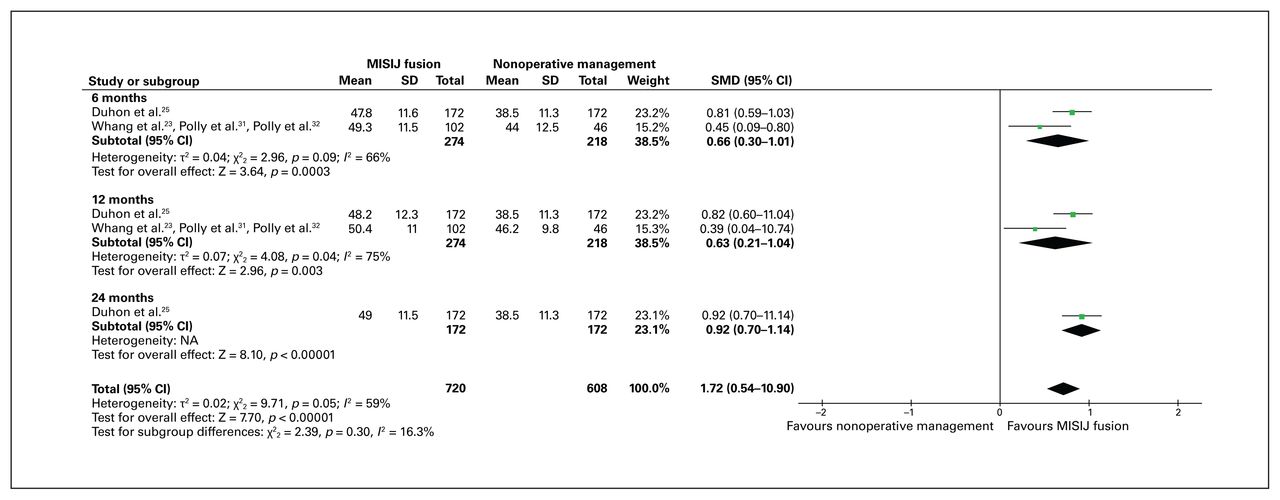
Two trials (5 of the articles) reported HRQoL using the SF-36 score, and all but 1 article32 were included in the analysis.23,25,31,34 The SF-36 score is further divided into 2 component scores: the physical component summary (PCS) and mental component summary (MCS). The weighted average SF-36 PCS score was 41.19 (range 40.1–43.1) and 32.68 (range 31.7–37.8) in the MISIJ fusion and nonoperative groups (WMD 8.51), respectively. The overall SF-36 PCS score was significantly higher with MISIJ fusion than with nonoperative management (SMD 1.01, 95% CI 0.83 to 1.19, p < 0.00001, I2 = 56%, low-quality evidence). Similarly, the subgroup analysis showed a significantly better SF-36 PCS score in favour of MISIJ fusion at 6, 12, and 24 months (Figure 5). The weighted average SF-36 MCS score was 48.8 (range 47.8–50.4) and 40.51 (range 38.5–46.2) in the MISIJ fusion and nonoperative groups (WMD 8.29), respectively. The overall SF-36 MCS score was significantly higher with MISIJ fusion than with nonoperative management (SMD 0.72, 95% CI 0.54 to 0.9, p < 0.00001, I2 = 59%, low-quality evidence). Similarly, the subgroup analysis showed a significantly better SF-36 MCS score in favour of MISIJ fusion at 6, 12, and 24 months (Figure 6). The article that could not be included in the meta-analysis showed a significant improvement in SF-36 PCS and MCS scores in favour of the MISIJ fusion at 24 months.32
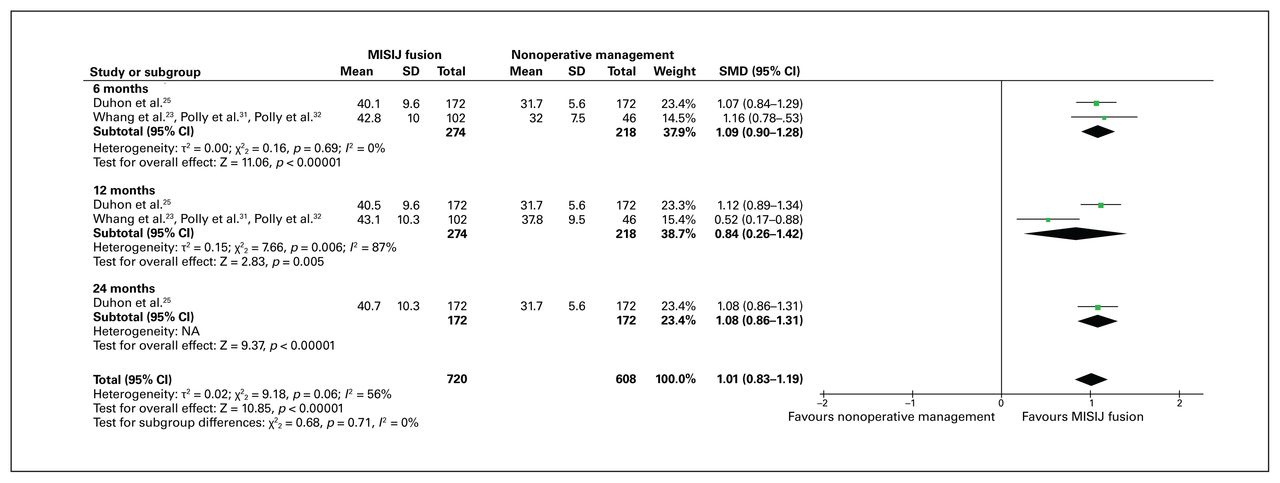
36-Item Short Form Health Survey physical component summary score favouring minimally invasive sacroiliac joint (MISIJ) fusion over nonoperative management. CI = confidence interval; NA = not applicable; SMD = standardized mean difference.
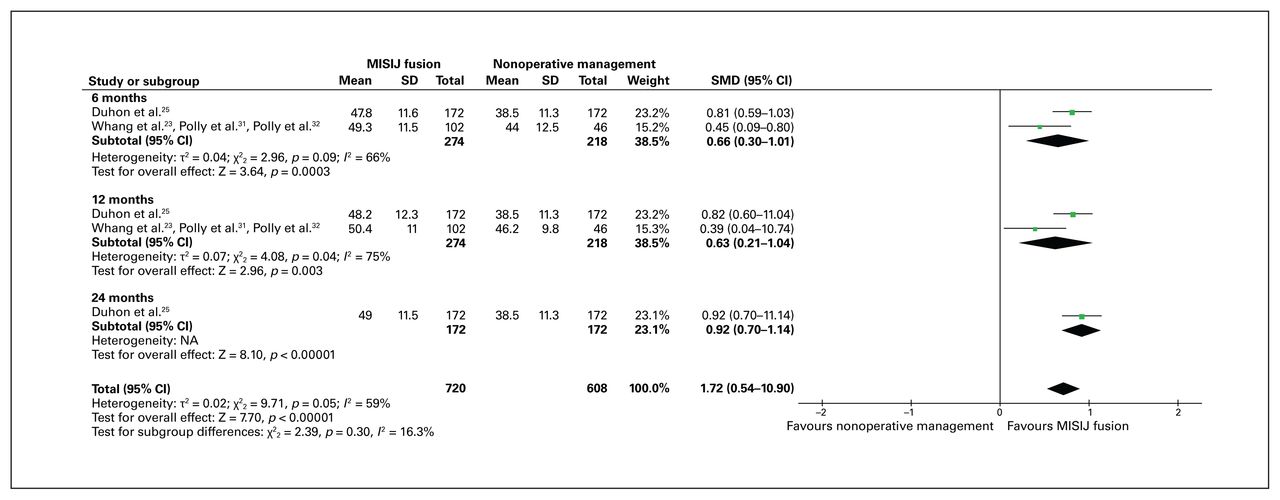
36-Item Short Form Health Survey mental component summary score favouring minimally invasive sacroiliac joint (MISIJ) fusion over nonoperative management. CI = confidence interval; NA = not applicable; SMD = standardized mean difference.
EuroQoL score
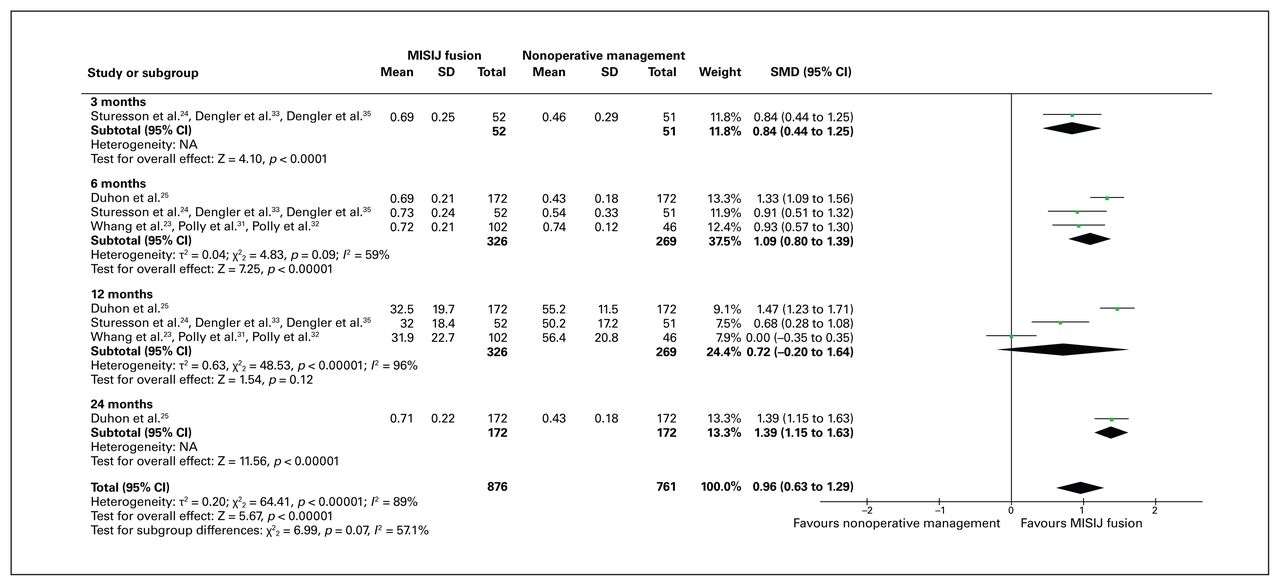
All 3 trials reported data on HRQoL using the EQ-5D score, and all but 2 articles32,35 were included in the analysis. 23–25,31,33,34 The weighted average EQ-5D score was 0.72 (range 0.69–0.74) and 0.50 (range 0.43–0.74) in the MISIJ fusion and nonoperative groups (WMD 0.22), respectively. The overall HRQoL using the EQ-5D score was significantly higher with MISIJ fusion than with nonoperative management (SMD 0.96, 95% CI 0.63 to 1.29, p < 0.00001, I2 = 89%, low-quality evidence). Similarly, the subgroup analysis showed a significant improvement in EQ-5D score in favour of MISIJ fusion at 3, 6, and 24 months, although the improvement was not significant at 12 months (Figure 7). The 2 articles that could not be included in the meta-analysis showed a significant improvement in EQ-5D score in favour of MISIJ fusion at 24 months.32,35
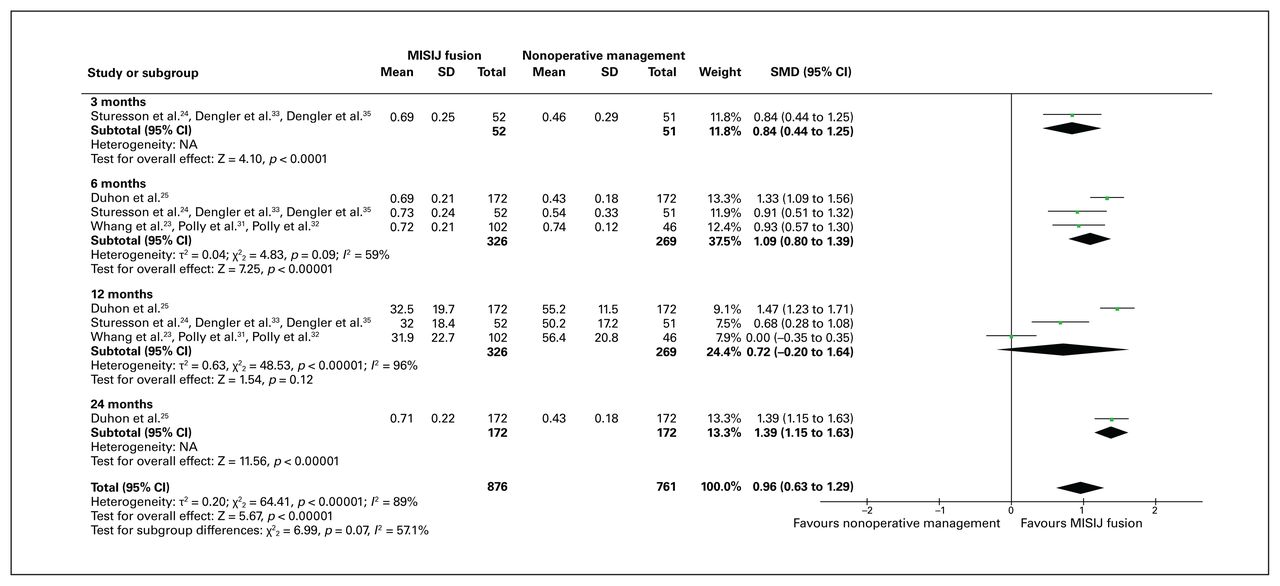
EuroQoL score favouring minimally invasive sacroiliac joint (MISIJ) fusion over nonoperative management. CI = confidence interval; NA = not applicable; SMD = standardized mean difference.
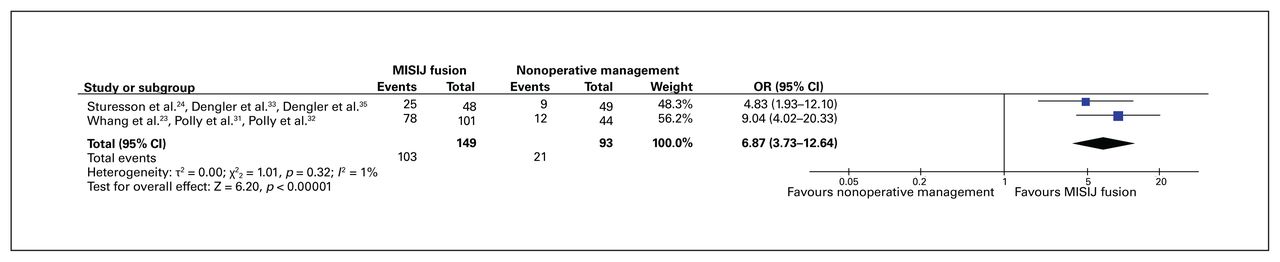
Patient satisfaction
Two trials (6 studies) reported data on patient satisfaction and were included in the analysis.23,24,31–33,35 The proportion of patients who were very satisfied at the end of the trial follow-up period (24 months) was 69.12% and 22.58% in the MISIJ fusion and nonoperative groups (incidence difference 46.54%), respectively. The satisfaction rate was significantly higher with MISIJ fusion than with nonoperative management (OR 6.87, 95% CI 3.73 to 12.64, p < 0.00001, I2 = 1%, moderate-quality evidence) (Figure 8).
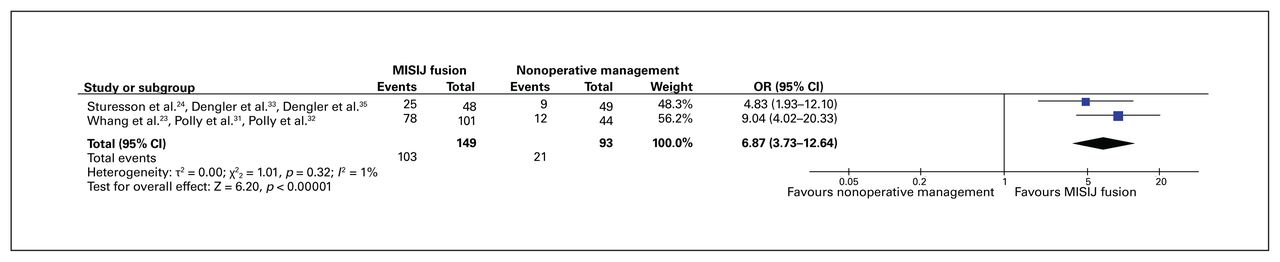
Patient satisfaction score favouring minimally invasive sacroiliac joint (MISIJ) fusion over nonoperative management. CI = confidence interval; OR= odds ratio.
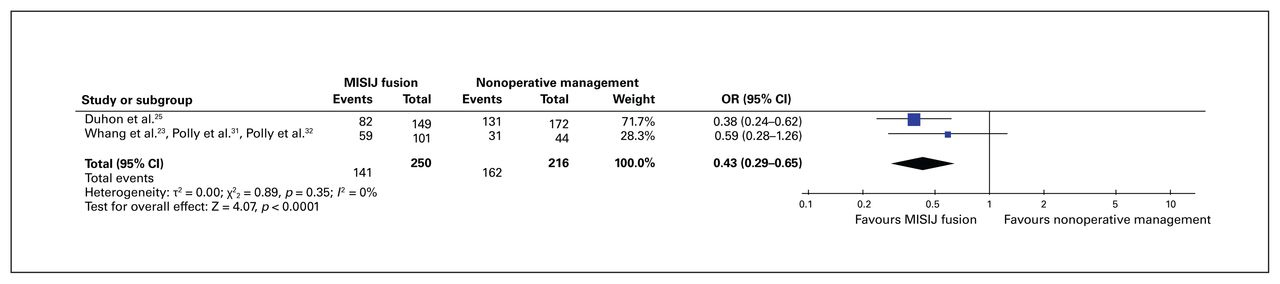
Opioid use
Two trials (5 studies) reported opioid use and were included in the analysis.23,25,31,32,34 The proportion of patients who were still using 1 or more opioid analgesics for SIJ or low back pain at the end of the trial follow-up period (24 months) was 56.4% and 75% in the MISIJ fusion and nonoperative groups (incidence difference −18.6%), respectively. There was a significant reduction in opioid use with MISIJ fusion than with nonoperative management (OR 0.43, 95% CI 0.29 to 0.65, p < 0.0001, I2 = 0%, low-quality evidence) (Figure 9).
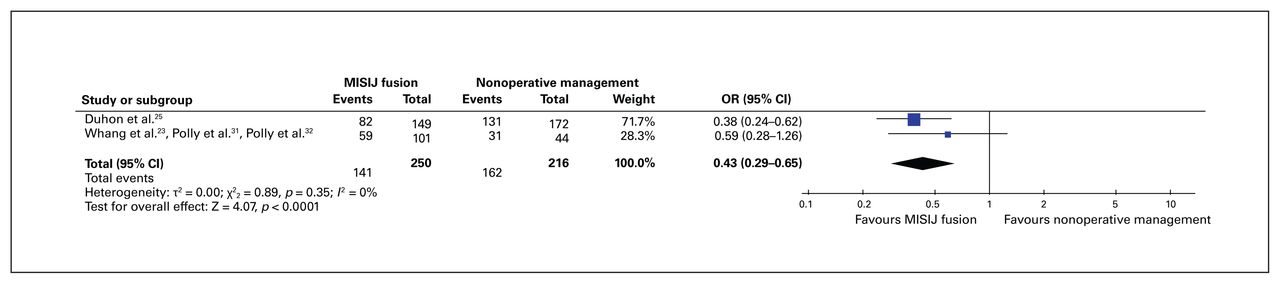
Opioid use favouring minimally invasive sacroiliac joint (MISIJ) fusion over nonoperative management (i.e., fewer patients in the MISIJ fusion group were taking opioids). CI = confidence interval; OR = odds ratio.
Adverse events
Two trials (6 studies) reported data on adverse events and were included in the analysis.23,24,31–33,35 The weighted average for the number of adverse events per patient at the end of the trial follow-up period (24 months) was 1.11 (range 0.27–1.8) and 1.14 (range 0.19–1.9) in the MISIJ fusion and nonoperative groups (WMD −0.03), respectively. In the MISIJ fusion group, the adverse events were divided into device-related and procedure-related events. Revision surgery (1.95%) and surgical wound problems (2.1%) were the most common device-related and procedure-related adverse events, respectively (Table 3). No significant difference was found between the MISIJ fusion and nonoperative management groups in terms of the number of adverse events per patient (SMD −0.03, 95% CI −0.28 to 0.23, p = 0.84; I2 = 0%, moderate-quality evidence) (Figure 10).

Comparison of adverse events between the minimally invasive sacroiliac joint (MISIJ) fusion and nonoperative management groups. There was no significant difference between the groups. CI = confidence interval; SMD = standardized mean difference.
Comparison of adverse events associated with MISIJ fusion
Discussion
In this systematic review and meta-analysis, the pooled estimate showed a significant improvement in pain score, disability score, HRQoL scores, patient satisfaction, and use of opioid analgesics in favour of MISIJ fusion with TTI at a follow-up of up to 24 months. Additionally, MISIJ fusion with TTI was not associated with a higher adverse event rate than nonoperative management for SIJ dysfunction.
Low back pain attributed to SIJ dysfunction has been perceived as a major cause of disability worldwide.1,36–38 In our review, the weighted average pain score was 2-fold lower in those who underwent MISIJ fusion than those who received nonoperative management (WMD –39.42). This statistically significant reduction in pain score is also clinically important, as it exceeds the threshold of the minimum clinically important difference (MCID) in chronic low back pain, which is a difference of 20 or more points on the VAS scale.39,40 Furthermore, the significant reduction in pain score has manifested in the ODI score. There was a statistically and clinically important improvement in the ODI score with MISIJ fusion compared with nonoperative management (WMD –18.11 points, MCID for ODI score ≥ 15 points difference) up to 24 months.23 Darr and Cher41 carried out a 4-year follow-up of some of the included trials and found that the clinical improvement in pain score (54-point decrease from baseline) and ODI score (26-point decrease from baseline) continued to be substantial. Furthermore, a comparative case series by Vanaclocha and colleagues42 compared conservative management, including weight reduction, smoking cessation, physiotherapy, and the use of nonsteroidal anti-inflammatory drugs to radiofrequency ablation and MISIJ fusion. At the 6-year follow-up, conservative management and radiofrequency denervation were associated with higher pain score (17 points and 11 points higher than baseline values, respectively) and ODI score (9 points and 8 points higher than baseline values, respectively). On the other hand, MISIJ fusion showed a statistically and clinically significant improvement in pain score and ODI score (58 points and 21 points lower than baseline values, respectively).
Health-related quality of life is an essential factor in determining the impact of a treatment plan on activities of daily living. In our review, HRQoL was measured using SF-36 PCS and MCS scores and the EQ-5D score. Patients assigned to MISIJ fusion had a marked improvement in SF-36 PCS and MCS scores and EQ-5D scores compared with patients assigned to nonoperative management. This improvement continued to be statistically significant up to 24 months. The EQ-5D score at 12 months was the only exception, showing a nonsignificant improvement in favour of MISIJ fusion. The weighted average SF-36 PCS score was 41.19 in the MISIJ fusion group and 32.68 in the nonoperative management group, and the weighted average SF-36 MCS score was 48.8 in the MISIJ fusion groups and 40.51 in the nonoperative management groups, and the weighted average EQ-5D score was 0.72 in the MISIJ fusion group and 0.50 in the nonoperative management group. The statistical improvement in the HRQoL scores exceeded the MCID threshold (SF-36 PCS score: WMD 8.51 points, MCID ≥ 4.6 points difference; SF-36 MCS score: WMD 8.29 points, MCID ≥ 6.8 points difference; EQ-5D score: WMD 0.22 points, MCID ≥ 0.15–0.46 points difference).43,44 Therefore, the MISIJ fusion heralds a substantial clinical improvement in HRQoL for patients with SIJ dysfunction.
The adverse event rate was comparable between MISIJ fusion and nonoperative management. The weighted average for the number of adverse events per patient was relatively low across the 2 treatment options (1.11 v. 1.14 adverse events per patient, respectively). Recurrent or residual SIJ pain was the most commonly reported patient complaint across the 2 groups. In the MISIJ fusion group, the proportion of adverse events requiring surgical revision was 1.95%. Miller and colleagues45 performed a postmarket analysis of the patients’ complaints following MISIJ fusion with TTI. The proportion of patients who had postoperative complains was 3.8%, and the most commonly reported postoperative complaint was pain. Neuropathic pain and recurrent SIJ pain were the most common causes. The proportion of adverse events requiring surgical revision in the study by Miller and colleagues was 1.8%,45 which is similar to that in our review. Surgical revision occurred mostly for symptomatic, malpositioned implants (0.9%) in the early postoperative period (median 19 d) and for symptom recurrence (0.6%) in the late postoperative period (median 279 d).45
There are many approved implant systems for MISIJ fusion other than the TTI system; these include hydroxyappatite coated screws and simmetry implant systems.46 Rappoport and colleagues,47 in a prospective case series, showed clinically meaningful results with MISIJ using a hydroxyappatite coated screws system. They reported a statistically significant and clinically important improvement in pain score (MCID ≥ 20-point difference on VAS scale) from baseline (55.8 ± 26.7) at 3 months (28.5 ± 21.6), 6 months (31.6 ± 26.9), and 12 months (32.7 ± 27.4). Furthermore, the clinical improvement in ODI score (MCID ≥ 15 points difference) from baseline (55.6 ± 16.1) was also substantial at 3 months (33.3 ± 16.8), 6 months (33 ± 16.8), and 12 months (34.6 ± 19.4).47 Similarly, a prospective single-armed clinical trial by Araghi and colleagues48 showed clinically significant improvements in pain score, ODI score, EQ-5D score, and SF-36 PCS and MCS scores with the use of a SImmetry implant system for MISIJ fusion. The evidence on the efficacy and safety of these other implant systems, however, was obtained from nonrandomized and noncontrolled studies. Moreover, these studies were limited by their small sample sizes, which affects the generalizability and applicability of the findings.
Limitations
Though our review provided clinical insight into the long-term impact of MISIJ fusion with TTI on pain, disability, and HRQoL in patients with SIJ dysfunction, we acknowledge that it has several limitations. First, the review included a small number of trials and had a relatively small sample size. Second, the quality of evidence according to GRADE was low for most of the reported outcomes, mainly because of the small number of trials and participants as well as high statistical heterogeneity in most of the outcomes.
Conclusion
Our systematic review and meta-analysis showed a statistically significant and clinically important improvement in pain, disability, HRQoL, and patient satisfaction in favour of MISIJ fusion with TTI compared with nonoperative management for SIJ dysfunction. Similarly, significantly fewer patients who had MISIJ fusion than those who received nonoperative management were using opioids. There was no significant difference in the rate of adverse events between MISIJ fusion and nonoperative management.
Footnotes
Competing interests: None declared.
Contributors: All authors contributed to the study conception and design. A. Ghaddaf, J. Alsharef, M. Alsaegh, R. Alshaban, A. Almutairi, and M. Alshehri acquired the data, which N. Alsharef, and A. Abualola analyzed. A. Ghaddaf, J. Alsharef, M. Alsaegh, R. Alshaban, A. Abualola, and M. Alshehri wrote the article. All authors revised it critically and approved the final version for publication.
- Accepted September 6, 2023.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.