


Adult ileocolic intussusception
Intussusception is uncommon in adults and has an identifiable cause in 90% of cases.1 It presents with a variety of acute, intermittent and chronic symptoms, making it difficult to diagnose preoperatively. Abdominal ultrasonography and computed tomography (CT) were shown to be the most useful radiologic methods in the diagnosis of adult intussusception.2
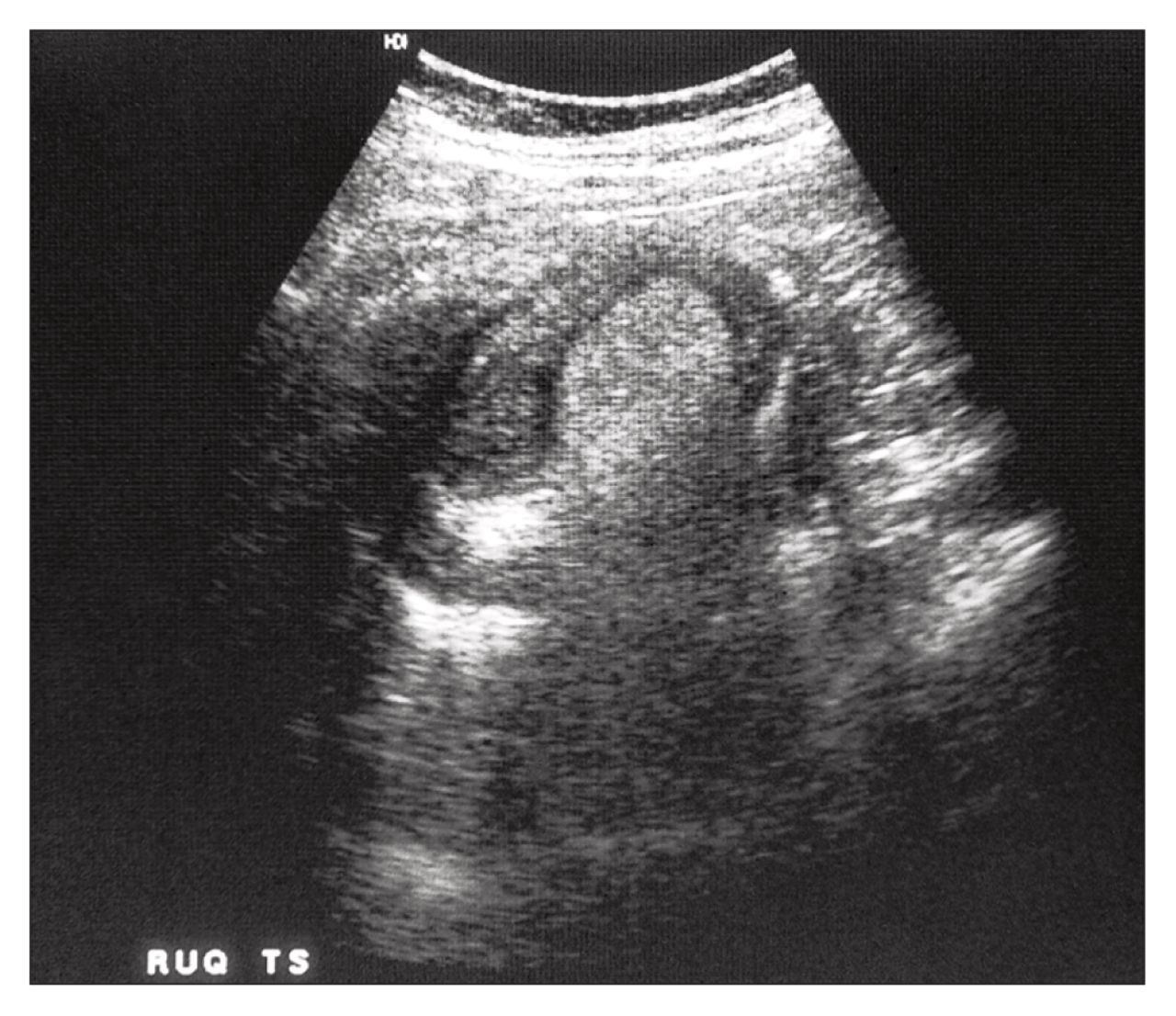
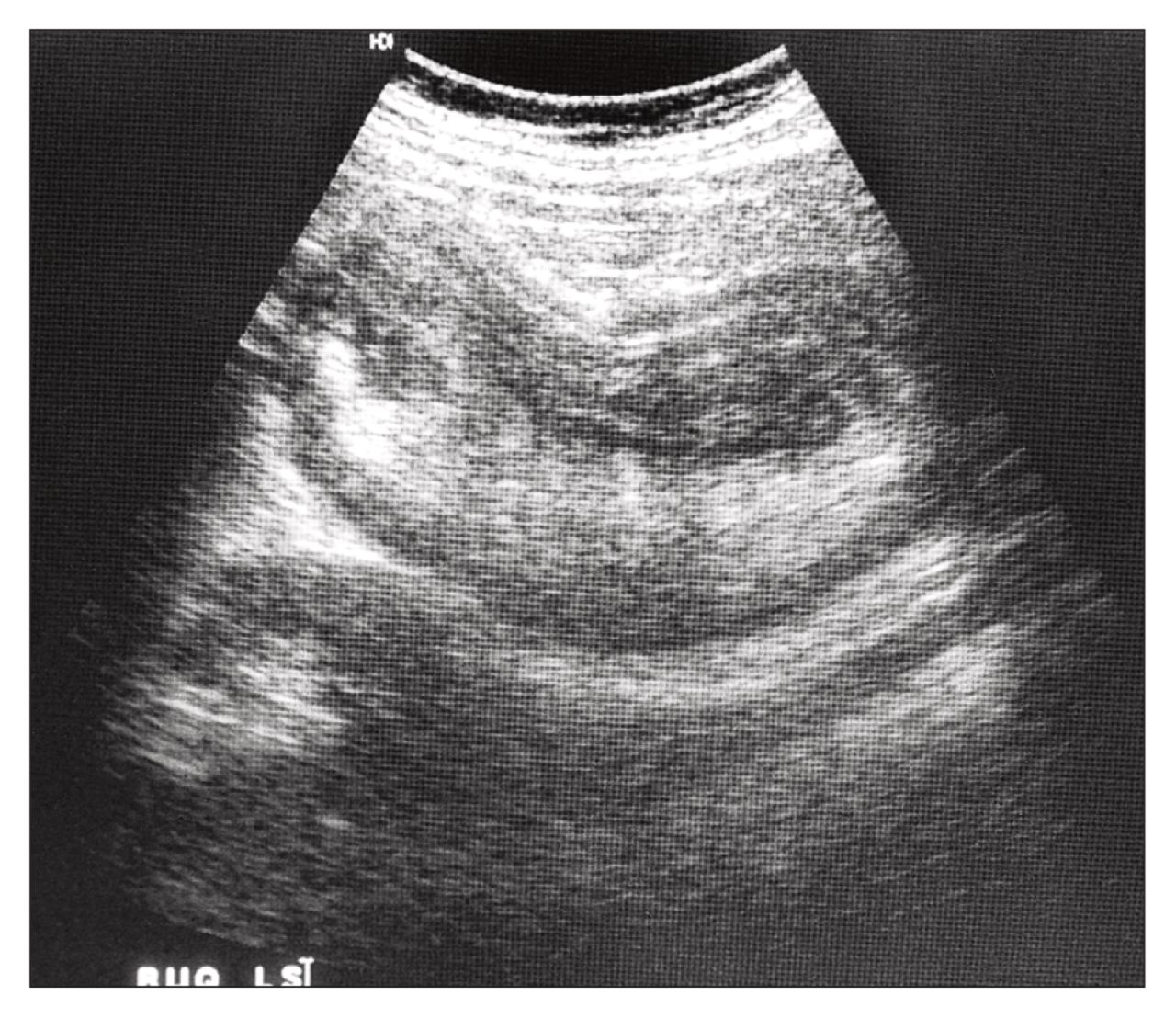
The classic sonographic features include the “dough-nut sign” in the transverse view (Fig. 1) and the “pseudokidney sign” in the longitudinal view (Fig. 2).3

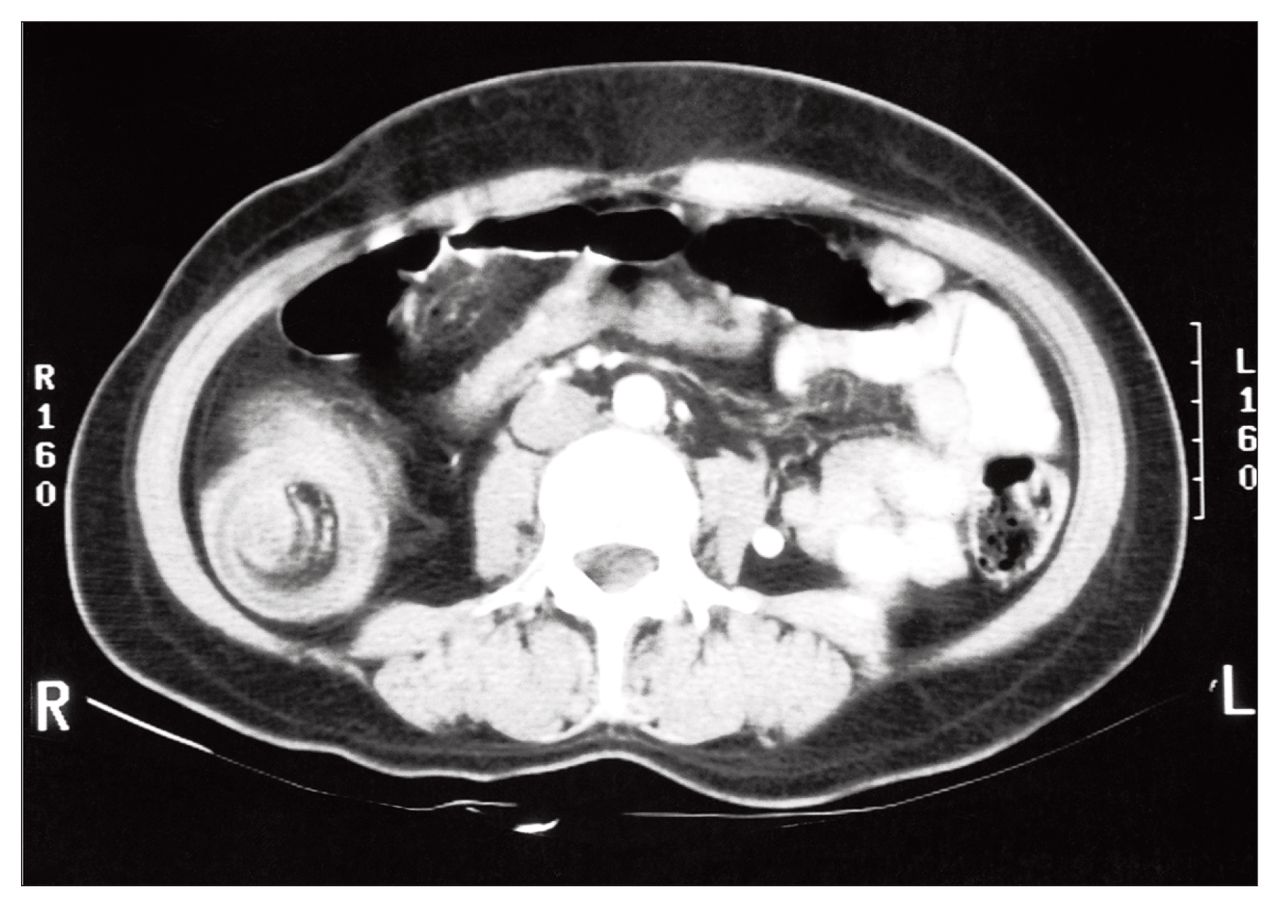
Abdominal CT reveals a mass lesion caused by a thickened segment of bowel due to telescoping of intussusceptum into the intussuscipiens and an eccentrically located low attenuated fatty mass that represents the invaginated mesentery (Fig. 3).4 In this case of ileocolic intussusception, CT at the level of the ileocecal valve revealed a tubular mass of mixed soft-tissue and fat projecting into the contrast-filled cecum (Fig. 4).

Laparotomy revealed a 13-cm segment of terminal ileum intussuscepting through the ileocecal valve into the ascending colon. The involved segment was resected. Histologic examination showed hemorrhagic necrosis of the terminal ileum but no other lesion. The patient recovered without complication.
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.