


Abstract
Mesh repairs have revolutionized hernia surgery. When used to patch or plug a musculoaponeurotic abdominal wall defect, the results have been much better than traditional pure tissue repairs. The difference is simple: patch and plug techniques avoid tension on tissues. The improved sutureless repair not only avoids tissue tension, it obviates the need to suture the mesh. Fixation is achieved by intra-abdominal pressure, the same force that caused the hernia. Thorough dissection of the inguinal canal and the indirect sac is essential to avoid early failure. Whereas various repairs can be used with excellent results, there is no substitute for a complete dissection of the peritoneal sac well into the iliac fossa.
The improved sutureless repair offers 2 advantages over the original version: (a) type III hernias can now be repaired without opening the canal’s posterior wall, and (b) the incidence of clinically evident seroma has been reduced by 90%. Most primary and recurrent groin hernias can be repaired under local or regional anesthesia on an outpatient basis. Immediate ambulation and prompt recovery accompany this technique. Most patients resume full activity and employment by the end of the first week. The procedure is simple to learn, easy to perform and less costly than other techniques.
The improved sutureless technique is the second generation of the original sutureless repair first used in 1987, reported in 1989 and published in 1992.1 All versions are based on the same principles: the internal ring is a natural muscular orifice that allows access to the iliac fossa; prosthetic mesh is an excellent material to use in this repair because it prevents an indirect hernial sac from protruding through the internal ring; and normal intra-abdominal force is sufficient to seat a mesh graft against the posterior wall (Pascal’s principle).
The internal ring is formed around the site where the testicle and spermatic cord pass through an aperture in the transversalis fascia. Its superior margin is formed by the transversus abdominis arch (internal oblique and transversus abdominis muscles), its inferior margins by aponeurotic fibres of the iliopubic tract, the inferior epigastric vessels and the interfoveolar ligament. Indirect inguinal hernias present through the internal ring. As the peritoneal sac and its contents enlarge, the internal ring progressively widens.
Prosthetic mesh is a safe, effective barrier to the internal ring. Of the nonabsorbable meshes currently available, polypropylene has proven most effective for this procedure. It has the best balance of pliability and resilience. The memory it develops by the size of its polymer strand and knitted characteristics encourage it to unfold when it is positioned in the iliac fossa. Its pore size allows sufficient fibrovascular cellular ingrowth for it to be incorporated into tissues. In contrast to polypropylene, Mersilene has no resilience, and expanded polytetrafluoroethylene lacks sufficient pore size to allow fibrovascular ingrowth.
Earlier concerns about mesh causing infection have been disproved.2 In the authors’ opinion, it is the availability and use of safe prosthetic mesh materials, more than any other factors, that have revolutionized techniques and improved the results of hernia surgery. Mesh has been essential in every laparoscopic technique of herniorrhaphy; certainly, without prosthetic mesh, laparoscopic efforts to repair hernias would not have lasted this long.
The 17th century work of Blaise Pascal on equalization of fluids in a closed space led to the development of the hydraulic press. Pascal’s principle, applied to intra-abdominal pressure, demonstrates that the pressure exerted by fluid in a closed space fluctuates with position and muscular exertion. In the adult human, the intra-abdominal pressure is 8 cm H2O in the supine or prone position, 20 cm H2O in the lower abdomen in the standing position, and as much as 80 cm H2O when a person coughs, vomits or strains. When prosthetic mesh is placed in the interparietoproperitoneal space, it becomes permanently seated against the anterior parieties by intra-abdominal pressures. Once this occurs, the mesh does not migrate. So long as the mesh is sufficiently large to cover the defect and to extend far enough radially from the edges of the defect to establish a sufficient purchase on the parities to which it fixes, intraabdominal force completely obviates the need to suture it. The repair is completely free of tension on tissues and on the graft.
Surgical technique
Surgery is typically performed with local or regional anesthesia injected by the surgeon (the local mixture is 50 mL bupivacaine 0.5%, 30 mL chloroprocaine 3% and 8 mL sodium bicarbonate 8.4%). This is supplemented by intravenous sedation (midazolam and fentanyl citrate), which is administered by an anesthesiologist or nurse-anesthetist. Whether for primary or recurrent hernias, patients aged 65 years or older receive a single perioperative dose of antibiotic. Cefazolin sodium, 1 g, is given unless the patient is sensitive to penicillin or cephalosporins, in which case clindamycin, 600 mg, is used. A transverse incision (average 6.5 cm long) is made laterally from the pubic tubercle. The external oblique aponeurosis is opened and the ilioinguinal nerve is preserved when it is visible. The cremasteric fascia is opened longitudinally and the spermatic cord is lifted from its nest within it. The medial leaf of the cremasteric fascia is excised to allow inspection of the posterior wall. By having the patient perform a Valsalva manoeuvre and cough, the surgeon can fully evaluate the integrity of the posterior wall. At this point the surgeon can verify that there is no direct component and that the sutureless repair can be used. The lateral cremasteric leaf, which contains the external spermatic vessels and the genital branch of the genitofemoral nerve, is preserved unless the hernia is found to be of type IV, or if a type IV component coexists with an indirect hernia.3 The internal spermatic fascia, which surrounds the cord, is opened. If a lipoma is present it is excised. The peritoneal sac is completely freed from the cord structures and from the investing fibres of the transversalis fascia at the deep ring. Dissection of the peritoneal sac to its true neck brings the operator through the internal ring to the threshold of the iliac fossa. Further dissection of peritoneum from the transversalis fascia, easily done with a sponge-stick through the internal ring, actualizes the potential space in the iliac fossa. A double layer of transversalis fascia exists at the internal ring and is divided by the deep epigastric vessels. The deeper layer must be opened to enter the interparietopreperitoneal spaces of Bogros and Hureau.4 If the vas and vessels are not freed from the neck of the sac, recurrent indirect herniation will occur.5 The peritoneal sac is usually not opened. It is invaginated through the deep ring into the iliac fossa. If a long sac is present within the cord, it is opened in its middle or proximal part to avoid compromising the vascularity of the distal cord and testis. The distal portion of the sac that remains attached to the cord is left undisturbed. The proximal portion is circumferentially dissected free, ligated and invaginated as described earlier. It is essential that the peritoneal sac be cleared from the threshold of the deep ring. This is necessary whether or not a sliding component exists. When the dissection has been completed, an umbrella plug is fashioned from a sterile individual swatch of polypropylene mesh (Fig. 1).6
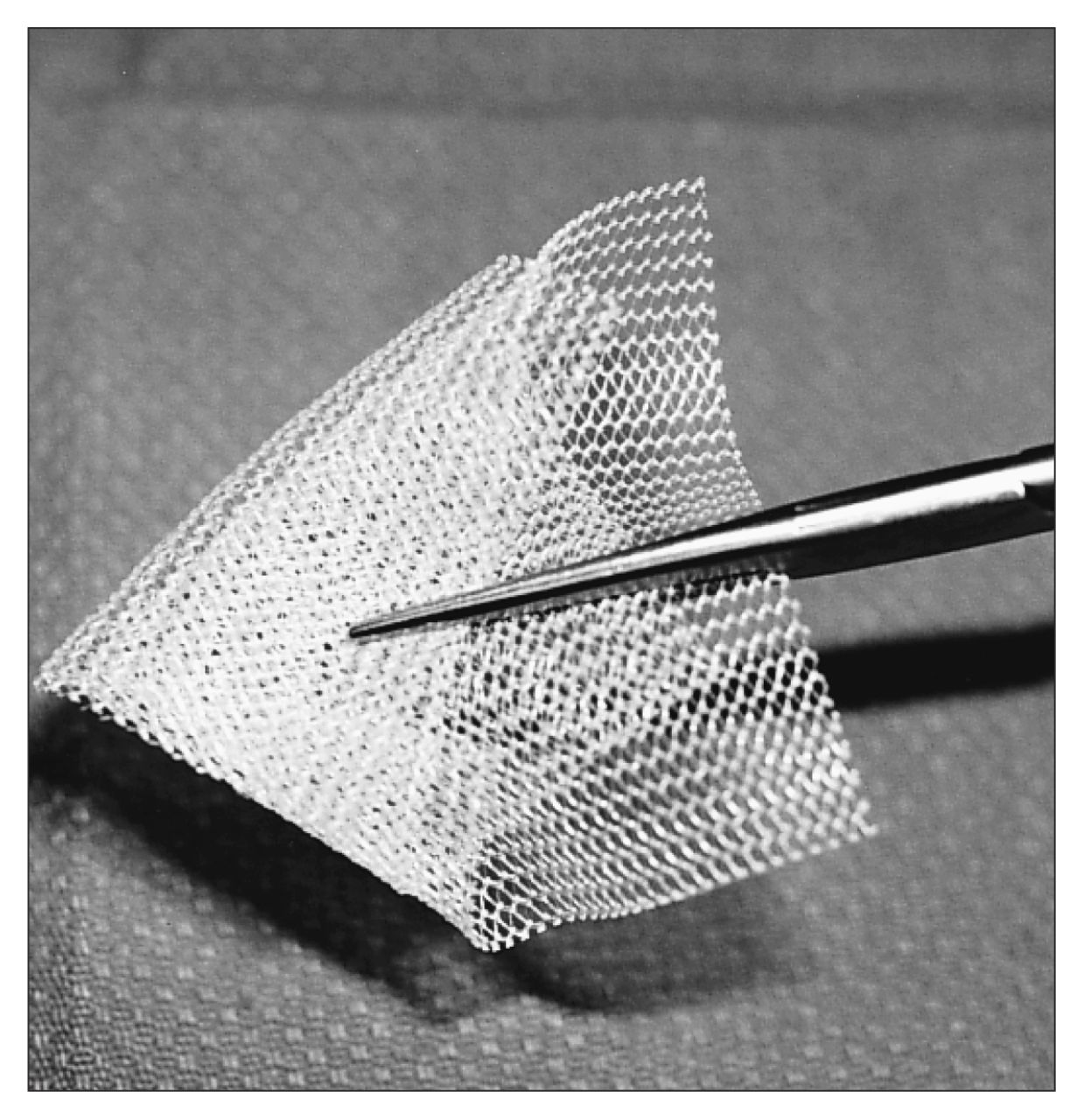
Umbrella plug graft, measuring 6.25 × 11.25 cm, made from Prolene mesh.
The insertion manoeuvre is performed as follows: (a) forceps are used to invaginate the peritoneal sac through the internal ring; (b) the operator’s index finger is passed along the forceps through the internal ring; (c) the forceps are removed; (d) the index finger palpates the iliac atery laterally (Fig. 2), (e) the umbrella plug is slid through the internal ring by riding it down the medial side of the operator’s index finger (Fig. 3); (f) the umbrella plug is released in the iliac fossa.
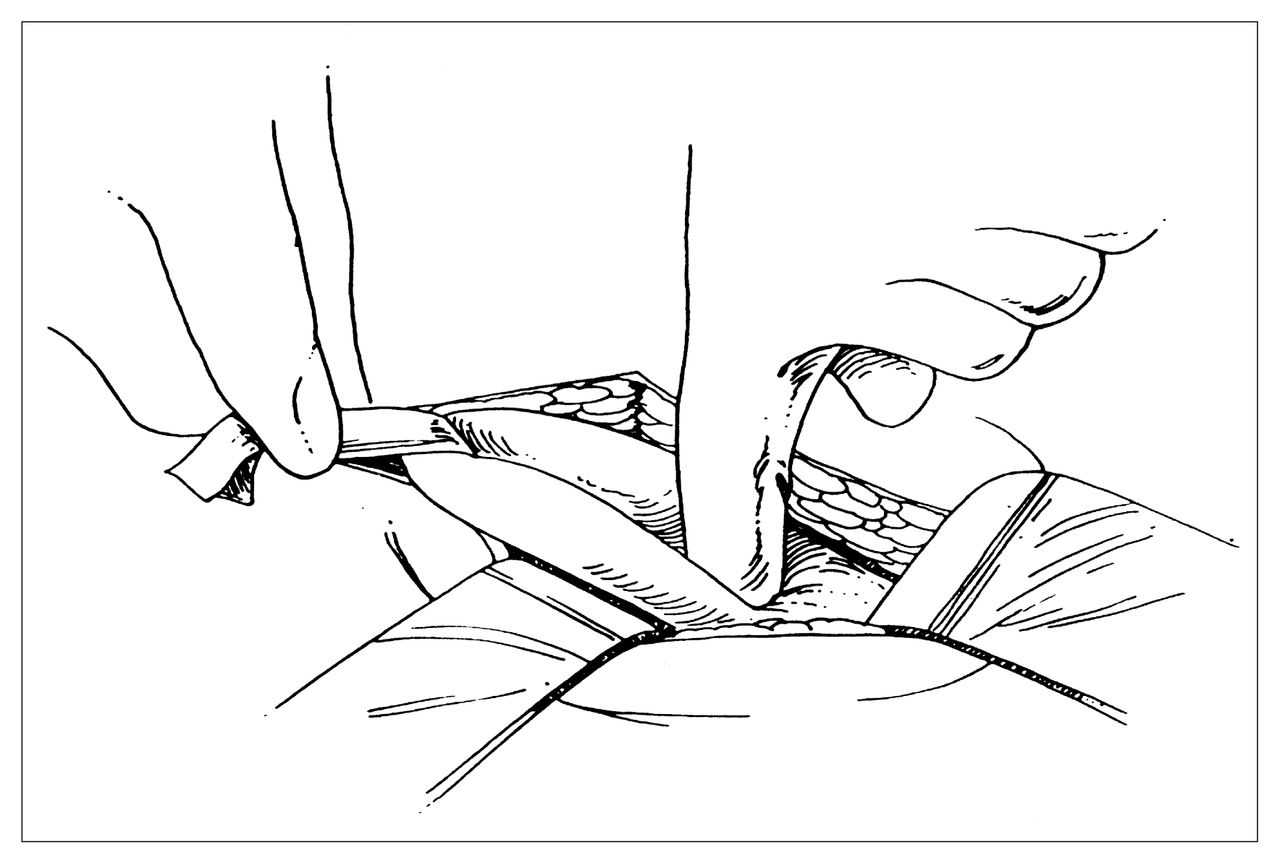
Index finger inserted through the internal ring after forceps have been removed.
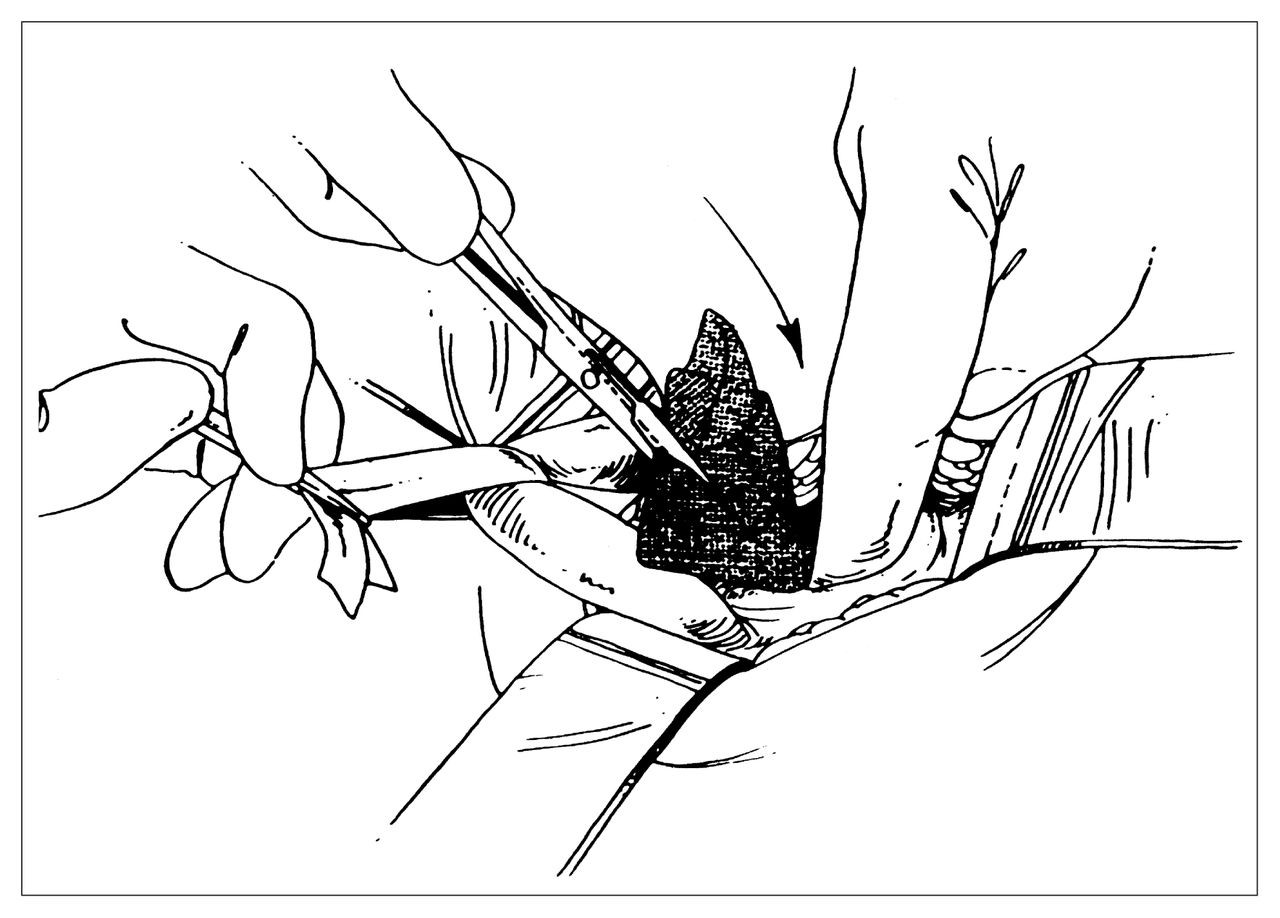
Placing umbrella plug into the properitoneal space.
Once the graft has been released, the patient seats it by coughing and straining on request. The umbrella plug alone is sufficient for types I and II hernias. When the internal ring is widened to 2 fingerbreadths or more (type III hernia), a single Prolene suture is placed, as described by Marcy,7 to reduce the size of the ring to no more than 1 fingerbreadth. This essentially converts a type III hernia to a type II hernia and allows the umbrella plug to do the necessary work of blocking the deep ring. No sutures are placed in the graft. The enlarged umbrella plug immediately cures the indirect hernia. It also protects a larger area of the posterior wall from developing an incipient direct hernia. The cord and the ilioinguinal nerve are replaced in their normal positions, and the external oblique aponeurosis is closed with a 3–0 continuous Vicryl suture, recreating the external ring. Subcutaneous and subcuticular closure is done. Immediately after the procedure, in the operating room, the patient exercises, then returns to the recovery area where he or she eats a light meal and is discharged after about an hour.
The improved sutureless repair is an excellent technique for all indirect hernias. In contrast to the original sutureless technique, which employed 2 swatches of Prolene mesh, the improved version uses only 1. The samesized (6.25 × 11.25 cm) rectangular-shaped sterile packaged mesh is used. By making an enlarged umbrella plug graft of Prolene mesh and inserting it through the internal ring, the surgeon secures the peritoneal sac of most indirect inguinal hernias deep to the abdominal wall. The Marcy suture can be placed if the operator has the least doubt about the effectiveness of the umbrella plug alone. The suture is equally effective when placed medial or lateral to the cord. Caution is advised in both instances: avoid the deep epigastric vessels when suturing medially and avoid the femoral vessels and nerve when suturing lateral to the internal ring.
Clinical experience
Since 1987 we have used a sutureless technique in 1621 of the 4485 patients who required repair of primary or recurrent hernias. Of these, the last 908 were done with the improved version. There were 5 failures (3 interstitial, 1 direct and 1 indirect) for a recurrence rate of 0.3%. Seroma formation, which occurred in 4.5% of original sutureless repairs, declined to 0.7% after introduction of the improved version. We attribute this reduction to avoiding mesh placement anterior to the canal’s posterior wall. In the improved version, serum that accumulates below the posterior wall is absorbed in the iliac fossa and does not become a clinical nuisance by swelling the wound. Among other complications, the incidences of infection, hematoma, testalgia and neuralgia were similar in both versions.
Patients return to their normal activities immediately. Self-employed patients resume work within 1 or 2 days, others within a week. Those who do heavy chores usually require a second week before they can perform all their responsibilities. Driving is restricted for 48 hours because of the potential liability related to the intravenous sedation used during the procedure.
Advantages of the sutureless technique and its improved version are: simplicity of the technique, absolute tension-free repair, minimal discomfort, immediate resumption of activity without fear of damaging the repair, and minimal cost considering the reduced surgical time needed and the nominal cost of mesh material.
Sutureless repairs are not used for type IV hernias. For full-floor direct hernias, we find it preferable to open the canal’s posterior wall, insert an underlay graft of Prolene mesh and do the first two layers of a Shouldice repair with 3–0 Prolene suture. The cord and nerve are handled as in the sutureless repairs. For multiple-time recurrent hernias, especially bilateral recurrences, we often do Stoppa’s procedure (giant prosthetic reinforcement of the visceral sac) with Mersilene mesh.8 Femoral hernias are repaired with a rolled plug by an external approach.9 Occasionally, femoral hernias are repaired through a posterior approach, especially when strangulation is suspected.
The sutureless repair of inguinal hernias is being done in many surgical centres. Personal communications from colleagues reflect their enthusiastic acceptance of the technique. The learning curve required for this procedure is minimal, therefore the degree of technical facility required in many other procedures, especially the laparoscopic approach, is unnecessary. Currently, comparative series of this technique are being done in Germany and Spain. We plan to report those results along with our own after adequate follow-up of our patients.
Footnotes
Symposium presented at the annual meeting of the Canadian Association of General Surgeons, Montreal, Que., Sept. 16, 1995
- Accepted January 29, 1997.
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.