


Abstract
Objective: To assess the efficacy of wound infiltration with local anesthetic in reducing postoperative pain after a muscle-splitting incision for appendectomy.
Design: A double-blind, placebo-controlled, randomized clinical trial.
Setting: The Royal Columbian Hospital, a university-affiliated community hospital.
Participants: Forty-three patients scheduled to undergo emergency appendectomy were randomized into treatment (21) and control (22) groups. Five patients were excluded from the treatment group.
Interventions: Local anesthetic infiltration of the wound before incision (treatment group) and saline infiltration (control group).
Main outcome measures: Postoperative analgesic requirements, pain assessment by visual analogue scale and length of hospital stay.
Results: No significant difference in analgesic use was seen between the 2 groups, as measured at 3 stages (Mc = control mean [standard deviation], Mt = treatment mean [standard deviation]): (a) in the recovery room, intravenous morphine use was Mt = 6.6 mg [8.6] v. Mc = 10.1 mg [7.2]; (b) in the first 2 postoperative days, intramuscular meperidine use was Mt = 309 mg [181] v. Mc = 278 mg [125] on day 1 and was Mt = 121 mg [132] v. Mc = 97 mg [128] on day 2; (c) in the final 5 days of follow-up, oral analgesic use was Mt = 11 [17] tablets v. Mc = 21 [16] tablets (acetaminophen with codeine). Pain assessments at rest, on a scale of 1 to 10, were found to be no different between groups, ratings being Mt = 4.7 [2.1] v. Mc = 4.5 [2.0] on day 1. Length of hospital stay averaged 3.0 days in both groups.
Conclusion: Infiltration with local anesthetic before incision does not pre-empt postoperative pain from a muscle-splitting incision used for appendectomy.
Over the past 10 years a new anesthetic concept, pre-emptive analgesia, has evolved from a theoretical construct to a clinically practised entity with firm adherents to its use. Pre-emptive analgesia is felt to act by reducing the input of noxious stimuli to central centres (the thalamus, somatosensory cortex and limbic system), thereby preventing the initiation of a negative cycle of pain-associated neural, humoral and behavioural responses.1,2
Diverse applications of this concept have been reported in the literature. Techniques of regional anesthesia achieve effective reduction in objective parameters of the stress response when used in lower limb and some pelvic surgery.3,4 Wound infiltration and regional nerve block techniques have been found to reduce postoperative pain and narcotic use for inguinal herniorrhaphy.5–7 Conflicting reports exist for the regional nerve block technique.8 Spinal and epidural anesthetic techniques have shown more variable results when applied to thoracic and abdominal operations. The impact of these techniques on the stress response has not been demonstrated, and there seems to be little effect on postoperative pain beyond 12 hours.2 Wound infiltration and nerve block anesthesia have been unsuccessful in controlling postoperative pain in cholecystectomy and thoracotomy incisions.9–11
Thus, although the concept of preemptive analgesia is attractive because of its potential to reduce pain and analgesic use, there is controversy regarding its efficacy in different clinical settings. We believed that a placebo-controlled, double-blind, randomized clinical trial would be the optimum method of evaluating wound infiltration as a pre-emptive technique in abdominal surgery. Wound infiltration, because of its simplicity, reproducibility and theoretic anti-inflammatory action, was used as our pre-emptive technique. We chose appendectomy because of its reproducible incision and the large volume of cases of appendicitis handled at our institution.
Our purpose was to assess objectively whether pre-incisional infiltration anesthesia reduces postoperative pain, analgesic use or length of hospital stay when applied to a muscle-splitting incision in the setting of emergency appendectomy.
Patients and methods
Between December 1992 and June 1994 we performed a double-blind, placebo-controlled, randomized clinical trial at the Royal Columbian Hospital, New Westminster, BC, enrolling consecutive patients who presented to the Emergency Department with a tentative diagnosis of appendicitis and who were between 16 and 75 years of age and fit to give informed consent. Five general surgeons at this community hospital participated in the study. Patients could only be enrolled if one of these surgeons was on call (which occurred about 50% of the time). Enrolment was established by the attending surgeon or a research nurse. Patients were excluded if the systolic blood pressure fell outside the range of 90 to 190 mm Hg, if the heart rate was greater than 120 beats/min, the respiratory rate greater than 24/min and temperature greater than 38.5 °C. Other exclusion criteria were cardiac arrhythmia requiring treatment, a history of allergy to a local anesthetic or of diabetes mellitus requiring medication. After selection and randomization, patients were also excluded if the appendix was perforated, the incision was extended beyond the area of anesthetic infiltration or an operation other than appendectomy was performed.
Preoperatively, patients received appropriate volume resuscitation and antibiotic prophylaxis. Once in the operating room, a general anesthetic was given according to standard protocol (induction with thiopental sodium, maintenance with isoflurane, relaxation if necessary with vecuronium bromide and minimal doses of fentanyl citrate early in the procedure). The planned incision site was marked and the abdomen prepared and draped in the usual fashion. A pair of vials marked only with a case number were then mixed together, followed by administration of 0.6 mL/kg of the solution into all layers of the proposed incision site. The control group received normal saline, whereas the treatment group received a combination of 1% lidocaine mixed with 0.25% bupivacaine and 1:400 000 epinephrine in equal volumes. The estimated duration of the local anesthesia was 4 to 6 hours.
Postoperatively, we requested that morphine or meperidine (or both) be used for parenteral analgesia and that acetaminophen with codeine be used for oral analgesia.
Postoperatively on the ward, each patient was requested to monitor the severity of pain every 3 to 4 hours and to document the use of oral analgesics in the study dossier. The surgical ward nurses were requested to record regularly the use of parenteral narcotics and patient mobility. On discharge, each patient was given a dossier and asked to complete a full week of postoperative self-monitoring. Each step of the study protocol was facilitated by the emergency research nurses, who also ensured complete collection of the dossiers. A blinded observer reviewed the patient charts to ensure that the protocol was followed and recorded data from the hospital stay.
Data analysis consisted of the comparison of group means by Student’s two-tailed t-test for the parametric variables (perioperative analgesic use, pain rating on the visual analogue scale and length of stay). Analysis was carried out using GV STAT software (IDE-DATA, Sweden, 1988) on a personal computer. The significance level was set at 0.05%.
Results
Forty-three patients were randomized in the operating room by a series of random numbers. Five more patients were eliminated, all from the treatment group. Reasons for exclusion included extension of the incision beyond the infiltrated area (2 cases), perforated appendicitis (2 cases) and age outside the study range (1 case).
The ages of patients in the 2 groups were similar (Table I). Neither operating times nor dose of the study agent given were significantly different in the 2 arms of the study. There were more males in the control group, but the difference was not statistically significant.
Demographic Characteristics of the 38 Patients Who Completed the Clinical Trial
We analysed analgesic requirements in 3 broad groupings: (a) morphine required in the recovery room; (b) parenteral analgesics needed in the first 48 hours and (c) analgesic requirements for the final 5 days of follow-up.
In the recovery room, the mean morphine requirements were smaller for the treatment group than for the control group (6.6 mg v. 10.1 mg of morphine sulfate) (Fig. 1). However, the difference was not statistically significant (p = 18) as the means had large standard deviations (treatment = 8.6 mg, control = 7.2 mg).
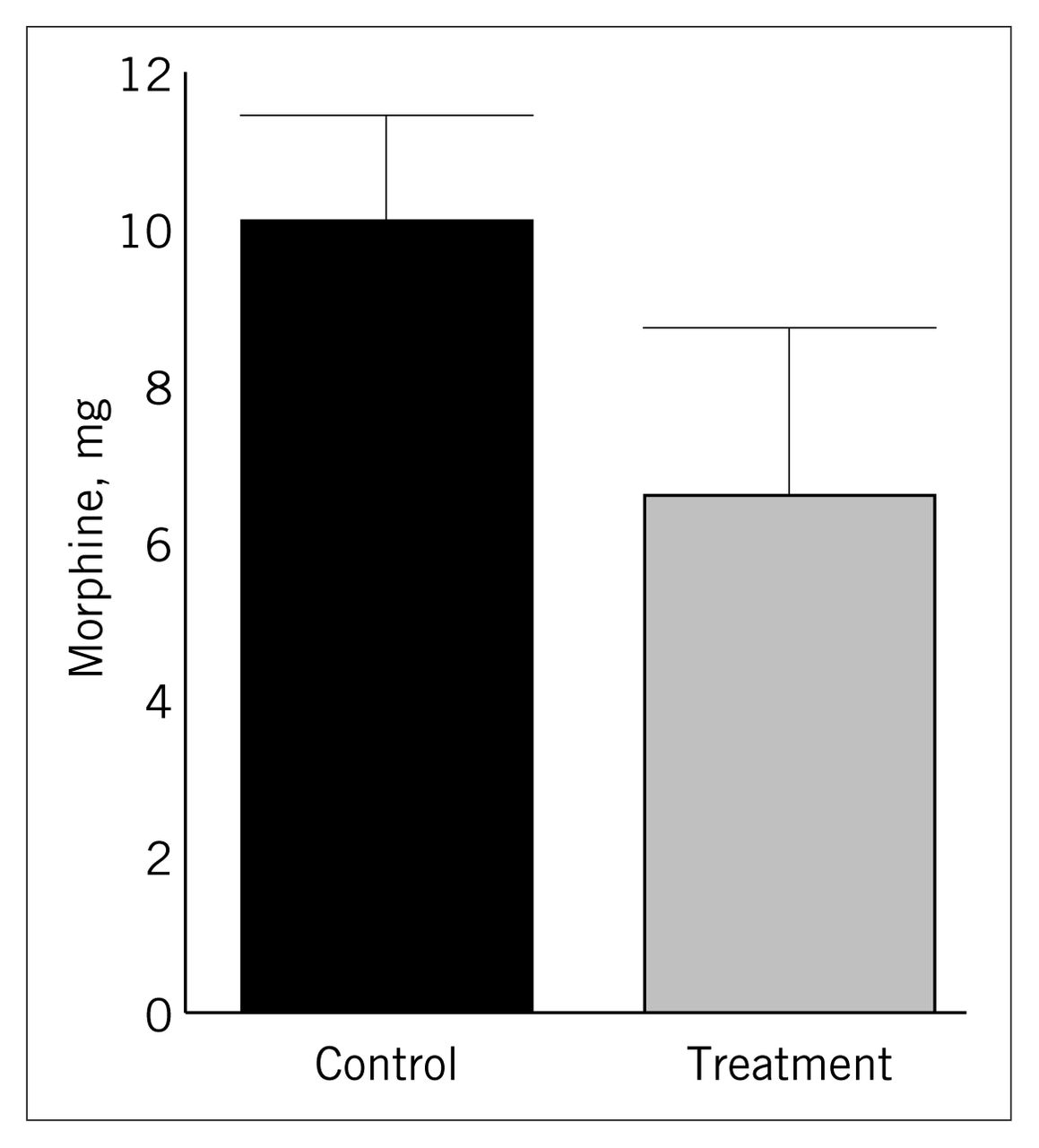
Mean morphine use in the recovery room for the control and treatment groups.
On each of the first 2 postoperative days, meperidine use was essentially equal for both arms of the study (Fig. 2).

Mean use of meperidine during the first 2 days postoperatively.
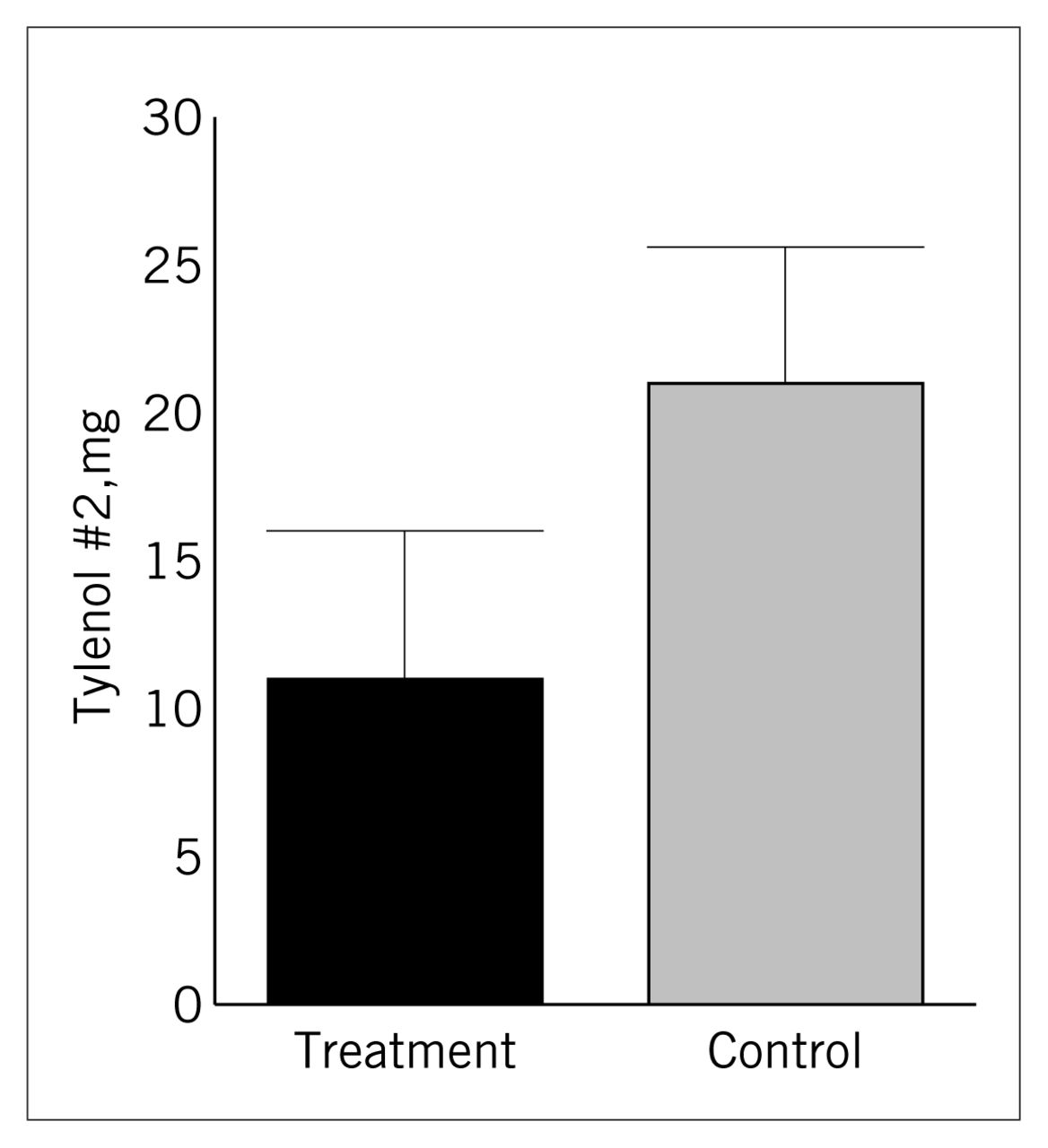
Although there appeared to be substantial group difference in the use of oral analgesia (Fig. 3), the difference was in fact marginally significant (p = 0.07) because of the large variance of the samples (treatment = 17 tabs, control = 16 tabs).

Mean use of oral analgesia during days 3 to 5 postoperatively, when most patients were discharged home.
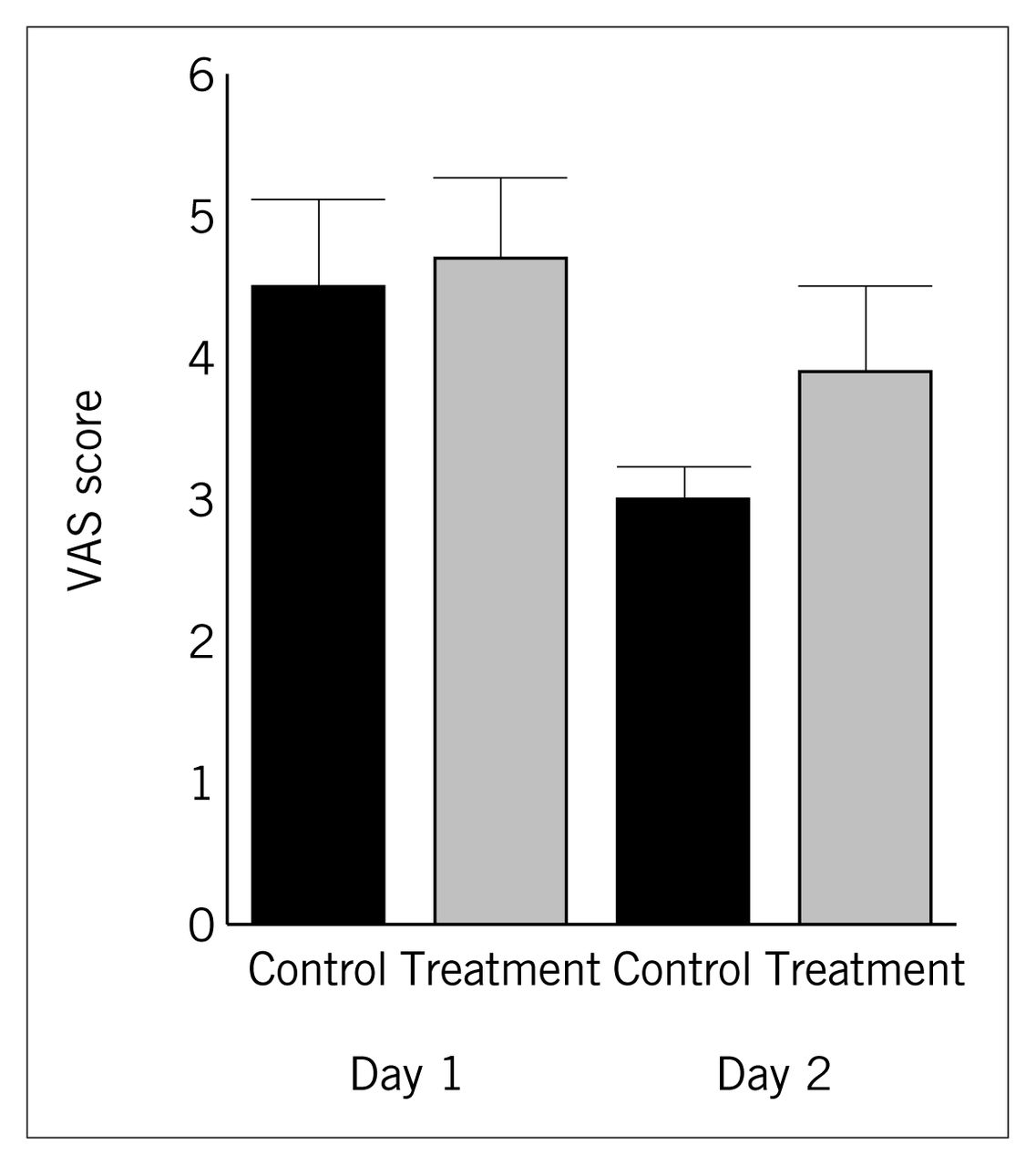
Visual analogue scale (VAS) ratings (range from 1 to 10) of postoperative pain in the 2 groups. The bars show the mean score of the first 2 postoperative days, for each group.
Patients monitored their own postoperative pain by means of a visual analogue scale. They were asked to record pain at rest, as well as pain when rising from the supine position, on a scale of 1 to 10 every 4 hours while awake. There was no demonstrable difference in pain at rest on either of the first 2 postoperative days (Fig. 2), when pain was consistently most intense, or at the later times. No significant difference was found between the treatment and control arms when pain was assessed for movement from the supine position.
Length of hospital stay was the same — 3 days on average — for both groups.
Finally, we examined the results obtained for patients treated by the staff surgeon with the greatest experience in local anesthesia and compared these to the group means (Table II). We selected only those patients receiving local anesthetic solution. No difference was significant.
Results Obtained by an Experienced Staff Surgeon Compared With the Overall Results in the Treatment Group*
Discussion
A motivating factor for our study was the presence of conflicting reports in the literature regarding the effectiveness of wound infiltration with local anesthetic even in the “established” area of inguinal hernior rhaphy.5,8 One area of difficulty in some reports is that preincisional anesthesia is compared to post-incisional anesthesia without the use of a placebo control group, making the effectiveness of treatment uncertain. 4–6,8
Another problematic area is the lack of blinding, either patients or investigators, in some studies.2,4,6 This is particularly important when dealing with a subjective area such as pain control.
Our approach was to conduct a placebo-controlled, double-blind randomized clinical trial to assess the effects of local anesthetic infiltration in patients who undergo appendectomy. This study design should have avoided confounding variables such as individual pain thresholds, the severity of the condition and variation in narcotic administration by different caregivers. However, when our study end points of postoperative narcotic use, postoperative pain levels and length of hospital stay were examined, we found no significant difference between the treatment and placebo groups.
One explanation for the failure of our study to show a benefit for preemptive local anesthesia could be that an adequate sensory block was not achieved. In our study, each patient was under general anesthesia at the time the wound was infiltrated, thus making assessment of the degree of block difficult. However, there is literature support for wound infiltration as effective pre-emption under similar circumstances in adult and pediatric inguinal herniorrhaphy.5–7,12 Furthermore, analysis of the current study’s group results in comparison to those obtained by one of the participating surgeons with a large experience in local anesthesia showed that the results were not dependent on experience.
A second possibility is that the presence of visceral pain preoperatively would initiate the pain response. Thus, local infiltration was not truly pre-emptive in our study. This is a valid argument, but does not on its own eliminate the potential for benefit from reducing postoperative incisional pain (as so well demonstrated in laparoscopic cholecystectomy).
Before drawing any conclusions from the results of this study, errors arising from sample size should be considered. In pre-trial planning, by examining samples used in similar studies5–11 ranging from 22 to 72 subjects, we estimated the sample size necessary to detect a significant decrease in intramuscular meperidine use to be 30 to 50 cases. However, 2 problems reduced the power of the data. The first was the exclusion process. Some cases had to be excluded after randomization, for example, when it was necessary to extend the incision to improve surgical access and this extension occurred beyond the area of infiltration or when the appendix was unexpectedly found to be perforated. This reduced the sample size to 43 cases. In addition, there was unexpected variability in the results, which further reduced the power to about 60% for detecting a reduction in morphine use. Statistical methods used to determine sample size from post-study data require a more uniform pattern of variability than the results we obtained for intramuscular meperidine use.13 In hindsight, a more appropriate technique of pain control would have been patient-controlled analgesia, which permits a more accurate measure of declining analgesic use over time than does intermittent intramuscular injection. We cannot therefore claim significant power to this study’s results in showing no difference between placebo and local anesthetic infiltration with regard to narcotic use. There are some clinically relevant findings, however, such as the lack of difference in postoperative hospital stay between the 2 groups (averaging 3 days each). This may reflect physician and patient attitudes toward early discharge in the 1990s, rather than improved comfort. We also found no difference in the patients’ self-assessed pain scores, which, when taken in concert with the lack of consistent difference in narcotic use, suggest that it may be worthwhile to pursue our hypothesis in future work.
Acknowledgments
We thank the staff surgeons at the Royal Columbian Hospital, whose participation in the trial was critical to its success: Drs. M. Bojm, S. Bugis, E. Letwin and L. Turner. Enrolment into the trial and compliance with its data collection was achieved through the work of Cathy Geldrich and the Emergency Research team at the Royal Columbian Hospital. Thanks to Ann Davidson, RN, Bonita Elliot, RN, and Doug Malyuk, Assistant Director of Pharmacy Services, for their help.
- Accepted August 20, 1996.
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.