


Adenocarcinoma of the breast commonly metastasizes to the skeleton, resulting in bone pain and pathologic fractures. After palliative internal fixation of these fractures or joint reconstruction for juxta-articular metastases, it is very unusual for progression of the disease process to result in failure of the prosthetic fixation, but in the case described here and in the images shown, rapid continued growth of the metastatic disease caused failure of fixation on 2 occasions due to bone erosion, culmMinating in amputation.
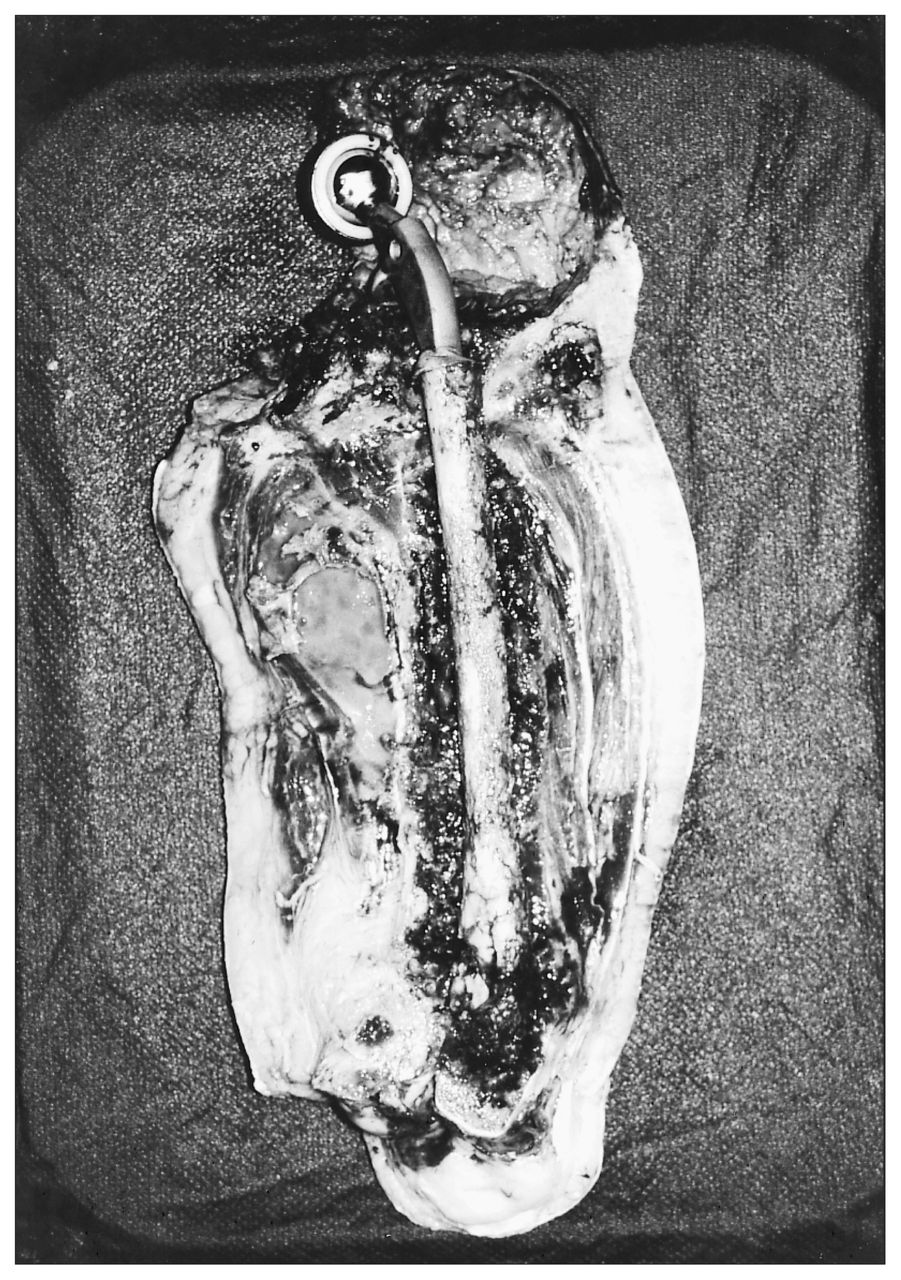
A 60-year-old woman underwent mastectomy for an infiltrating ductal carcinoma of the right breast. She remained well for 5 years, when an intertrochanteric metastasis developed in the right proximal femur. This was stabilized prophylactically with a dynamic compression screw and plate (Fig. 1). Three years later she had symptoms from recurrence of metastatic disease at the lower end of the plate, and this was treated by conversion to a long-stemmed cemented hemiarthroplasty (Fig. 2). However, 4 months later she again had symptoms in the right thigh. A radiograph revealed near-complete disappearance of the entire right femur with complete loss of fixation of the cemented stem (Fig. 3). A biopsy confirmed recurrent metastatic disease. Because she had severe pain from movement of the prosthesis within the soft tissues, we carried out a hip disarticulation. The excised specimen confirmed the complete absence of bone down to the level of the femoral condyles and the prosthesis lying freely within the soft tissues (Fig. 4).



Footnotes
Section Editors: David P. Girvan, MD, and Nis Schmidt, MD
Submissions to Surgical Images should be sent to Dr. David P. Girvan, Victoria Hospital Corporation, PO Box 5375, Station B, London ON N6A 5A5 or to Dr. Nis Schmidt, Department of Surgery, St. Paul’s Hospital, 1081 Burrard St., Vancouver BC V6Z 1Y6, with a copy of the submitting letter to Dr. Jonathan L. Meakins, Rm. S10.34, Royal Victoria Hospital, 687 Pine Ave. W, Montreal QC H3A 1A1
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.