


Abstract
A 34-year-old man with multiplex congenita contractures underwent replacement of 2 hips and 1 knee. Even though a good range of movement was achieved at surgery and intensive physiotherapy, his joints returned to their preoperative status within 2 years. This outcome suggests that total joint replacement has little to offer the patient with multiplex congenita contractures who has immobile joints.
Multiplex congenita contractures (MCC) or, as the condition used to be called, arthrogryposis multiplex congenita, is a rare disease characterized by stiff, deformed joints and muscle wasting. There are thought to be 2 types: neurogenic, due to patchy loss of the anterior horn cells in the spinal cord,1 and a failure of muscle embryogenesis with fibrosis and disorganization of muscle architecture. Excessive fibrous infiltration is said to be found in periarticular soft tissues as well as in subcutaneous fat and skin, which is tight and inelastic. The muscle abnormality is said to be static, but secondary joint changes tend to become more severe during the growing years. Patients with this disease can be considered in 2 categories: those who have mobile joints and those who have immobile joints.
The deformities include all 4 limbs in 50% of cases, both lower limbs in 30%, and rarely, both upper limbs.2 The hereditary aspects are not clear. Some neurogenic types may be associated with mental retardation, but in most cases the patient is intellectually normal.3 Although the disease has no effect on life-span,2 information on the treatment of the adult with this condition is almost nonexistent.
I achieved excellent results after replacing the hips of 1 patient who had MCC,4 but here I report a subsequent case in which it is doubtful that surgery benefitted the patient at all.
Case report
This 34-year-old man had a severe form of MCC, affecting both arms and legs. He had a 30° fixed flexion deformity of both hips with an active arc of motion of about 20°. This motion could not be increased passively. He also had a 20° internal rotation contracture and was unable to abduct more than 10° on either side. His left knee appeared to be in about 30° of valgus, but this was difficult to determine because of his internal rotation contracture at the hip. Movement in his left knee ranged from 5° to 50° and in the right knee from 10° to 90°. He had some ankle motion and could stand with his feet plantigrade. He could walk only with extreme difficulty. He had internal rotatory contractures of both shoulders and contractures of his elbows and wrists. His family was having increasing difficulties looking after him because of his immobility.
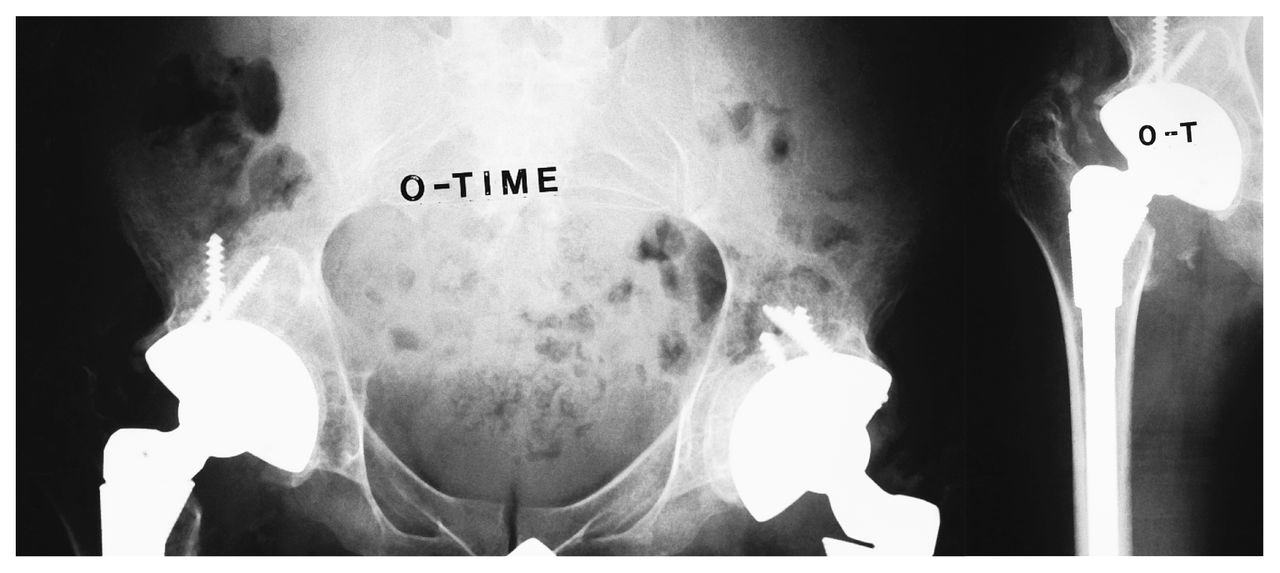
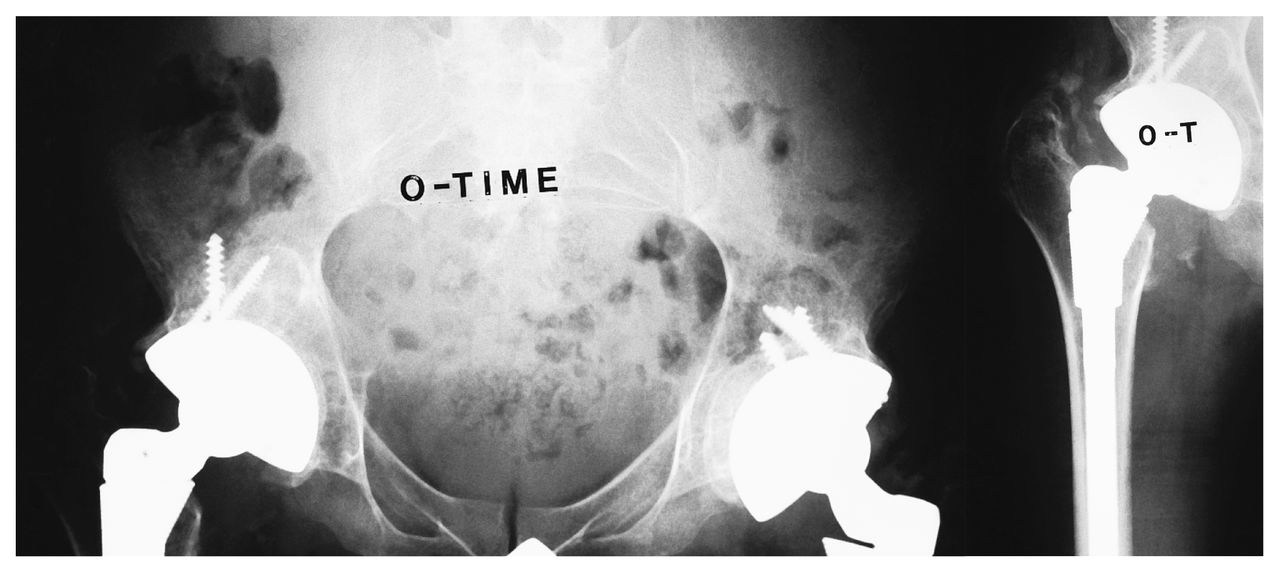
Radiographs of his hips (Fig. 1) and left knee (Fig. 2) showed a severe degree of osteoarthritis. Because the patient spoke no English (he was Sudanese), communication with him was difficult. However, pain did not appear to be a major issue. After multiple consultations with his family and other doctors, it was felt that bilateral total hip replacement and a left total knee replacement might allow him to become more functional, especially in terms of hip abduction to allow access to the perineum.

Preoperative view of the hips shows bilateral severe arthritis with considerable osteophyte formation.

Anteroposterior (left) and lateral (right) views of the knee preoperatively show severe arthritis. The anteroposterior view does not show the degree of valgus that is clinically present.
The hip replacement was done through an anterolateral approach. The periarticular tissues did not appear to be particularly abnormal but were very tight, so the short external rotators were released and a posterior capsulectomy was carried out (Fig. 3). The range of motion achieved at surgery was good: flexion of more than 90° was obtained. Early in the rehabilitation phase, he seemed to have a good range of movement in his hips. Ambulation, however, was still extremely difficult because of his left knee contractures, so the knee was replaced 6 weeks later. Since he appeared to be losing hip abduction capacity, bilateral percutaneous adductor tenotomies were carried out at the same time. The knee replacement was extremely difficult, requiring extensive ligament releasing. Because of this, a total condylar type III knee prosthesis was used (Fig. 4).
Radiographs obtained shortly after the hip replacement. Ingrowth components were used because of the patient’s age. No particular difficulties were encountered except that the femoral head was virtually fused into the acetabulum and was broken up in situ. Some floor grafting was required.

Radiograph obtained after total knee replacement. Extensive ligament release was required so a total condylar type III knee prosthesis was inserted.
Unfortunately, he continued to lose range of movement in his hips in spite of intensive physiotherapy, and by the end of the first year postoperatively, his condition had effectively returned to that seen preoperatively. His knee also returned to its preoperative range of motion and the internal rotation of his hips again produced an apparent knee valgus, although a true anteroposterior x-ray film showed that the knee was relatively well aligned.
At 2-year follow-up radiographs of his hips showed heterotopic ossification on one side (Fig. 5) but not on the other. It is unlikely that this heterotopic ossification explained his contractures.

View at 2 years. Myositis ossificans is seen on one side (arrow). The other hip, however, has an identical flexion, adduction and internal rotation contracture.
At the last follow-up, the patient could walk only with extreme difficulty and was almost wheelchair-bound.
Discussion
In this case, it is doubtful if surgery benefitted the patient at all, other than increasing access to the perineum. There almost no published reports on surgery for MCC in adults. In my previous experience of a case of MCC, bilateral total hip replacement was very successful in terms of pain relief and range of motion. In the present case, however, the joints returned to their preoperative status. The difference may be that the hips in the first case were effectively dislocated and a good range of motion without contractures was present before surgery. The second patient would seem to be of a different type, starting with largely immobile joints and returning to that state. Because there is so little in the literature on total joint replacement in cases of MCC and yet these people enjoy a normal life expectancy, perhaps the appearance of severe arthritis in this patient was merely a coexistent disease. Alternatively, because pain was not a major feature in this case as it was in the patient with mobile joints, one may theorize that the arthritic joint may not be a significant source of symptoms in the immobile type of MCC.
In retrospect, an excision arthroplasty of the hip, perhaps even a derotation abduction osteotomy of the proximal femur, might have been of more value to this patient. However, because he was able to walk before surgery, albeit with extreme difficulty, there was some concern that either of these operations would have effectively precluded ambulation.
The only conclusion that one can draw from this case is that joint replacement is unlikely to increase the range of motion or abolish contractures in the adult with MCC who has a contracted joint with a very limited range of movement. The cause of these contractures in the soft tissue subsequent to total joint replacement remains unknown.
- Accepted August 11, 1997.
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.