


Abstract
Carcinoids of the extrahepatic bile ducts and particularly the common bile duct are extremely rare. A 65-year-old woman presented with obstructive jaundice. Laboratory and imaging studies gave results that were consistent with an obstructing lesion in the common bile duct. In this case, a stent was inserted initially to decompress the bile ducts. Subsequently a laparotomy and pancreaticoduodenectomy were performed and a tissue diagnosis of carcinoid of the common bile duct was made. The patient was well with no evidence of recurrence 17 months postoperatively. The authors believe this is the 19th reported case of an extrahepatic bile duct carcinoid.
Carcinoids of the extrahepatic bile ducts are rare. We present what we believe is only the 19th reported case of a primary carcinoid occurring in the extrahepatic bile ducts, specifically in the common bile duct. The literature on the subject is reviewed briefly.
Case report
A 65-year-old diabetic woman was referred to the Victoria General Hospital in Victoria, BC, with obstructive jaundice. The patient had been well until 5 to 6 weeks before admission, at which time she started to have diarrhea, “orange urine” and pruritus and lost 4.5 kg in weight. She had complained of an unusual throbbing pain in the left upper abdominal quadrant periodically over the past several months. She became jaundiced 1 week later. Relevant medical history included a similar episode of jaundice 2 years previously, which lasted a few days and resolved without treatment. Thirty years earlier, she had undergone a cholecystectomy for multiple gallstones. She denied drinking alcohol and failed to describe any features consistent with the carcinoid syndrome.
On physical examination she was mildly icteric and in no distress. Her body temperature was normal, her heart rate was 76 beats/min and her blood pressure was 160/70 mm Hg. There was tenderness in the epigastric region but no discrete palpable mass, no rebound tenderness and no guarding. There was no evidence of hepatosplenomegaly. Laboratory investigations gave the following results: leukocyte count 15.9 × 109/L, hemoglobin level 121 g/L, serum levels of sodium 138 mmol/L, potassium 3.7 mmol/L, bicarbonate 29 mmol/L, chloride 102 mmol/L, urea 4.0 mmol/L, creatinine 80 μmol/L, total bilirubin 58 μmol/L (26 μmol/L conjugated), alkaline phosphatase 134 U/L, aspartate aminotransferase 61 U/L, γ-glutamyl transferase 188 U/L and amylase 47 U/L.
Abdominal ultrasonography revealed a dilated common bile duct with distal obstruction. Endoscopic retrograde cholangiopancreatography (ERCP) demonstrated an irregular stricture in the lower common bile duct 2 to 3 cm from the papilla of Vater (Fig. 1). A stent was inserted at the site of the stricture and computed tomography (CT) carried out to assess the possibility of a neoplastic lesion. The CT scan did not demonstrate a mass in the head of the pancreas. The patient’s jaundice resolved and laboratory values returned to normal within a few days.
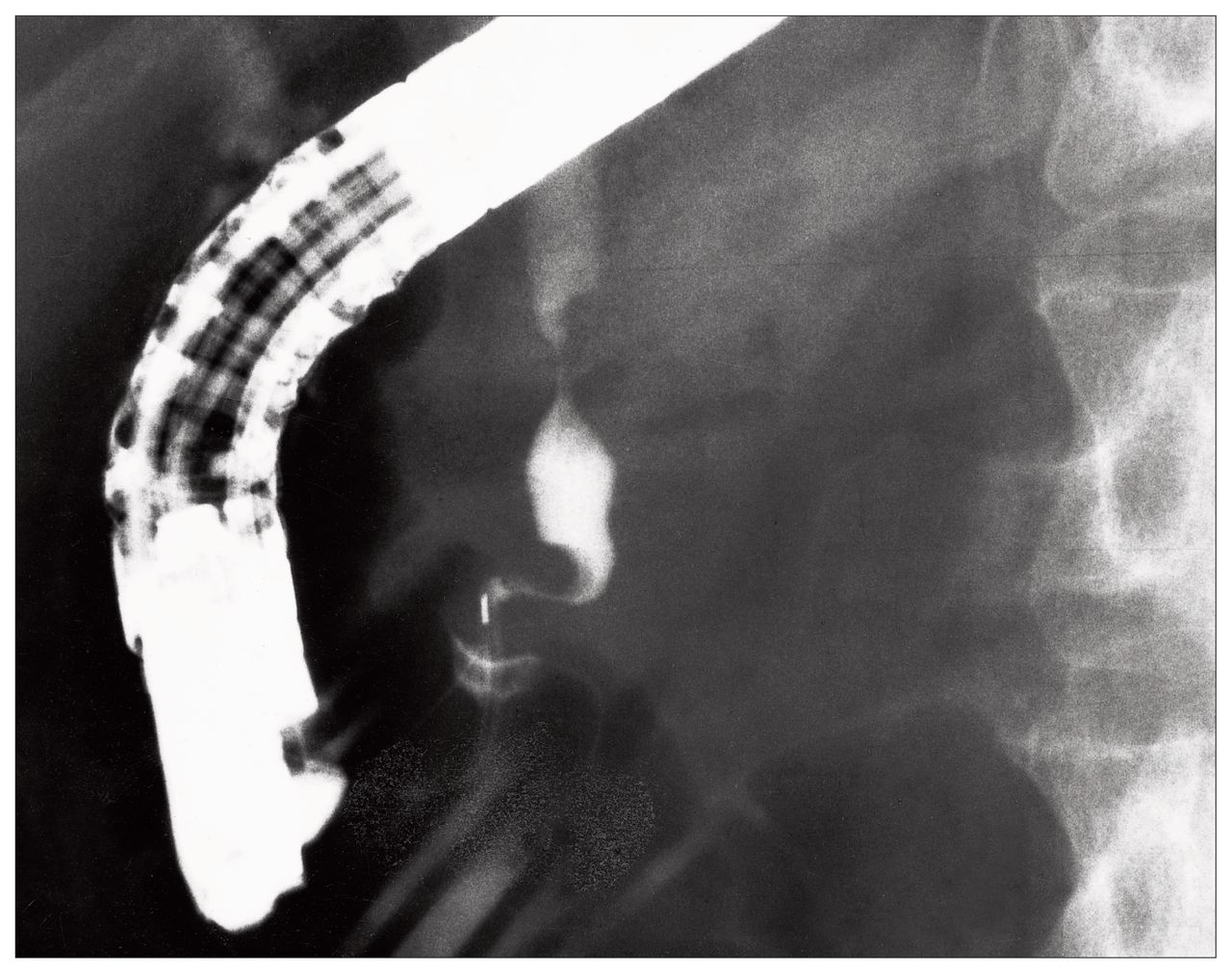
Endoscopic retrograde cholangiopancreatogram showing common bile duct stricture proximal to the ampulla of Vater.
The impression was that this patient, in view of her good health, had a benign, long-standing stricture secondary to her previous cholecystectomy. She was scheduled to return for stent removal in 2 to 3 months.
Four weeks later she was readmitted with abdominal pain, jaundice and fever, and a diagnosis of cholangitis. At that time laboratory findings were as follows: leukocyte count 11.2 × 109/L, hemoglobin level 113 g/L, and serum levels of sodium 137 mmol/L, potassium 3.6 mmol/L, bicarbonate 29 mmol/L, chloride 100 mmol/L, urea 3.0 mmol/L, creatinine 80 μmol/L, total bilirubin 74 μmol/L (conjugated 52 μmol/L), alkaline phosphatase 148 U/L, aspartate aminotransferase 170 U/L and amylase 29 U/L. The ERCP was therapeutic, enabling drainage of pus from the proximal bile duct, as well as clearly demonstrating the common bile duct stricture again. The patient was referred to a general surgeon and after assessment at laparotomy, she underwent a pancreaticoduodenectomy.
Postoperatively, she progressed well for 6 days when she experienced abdominal pain, fever and shortness of breath. Two fluid collections were found in the abdomen. One was drained with CT guidance, and the fluid obtained was old, sanguineous, bile-tinged fluid. No definite anastomotic leak was found. The other fluid collection was diagnosed as a hematoma, which slowly resolved. The patient was discharged home 24 days after operation and was well at follow-up 17 months postoperatively.
Pathological findings
Examination of the tissue revealed a constricted area of the distal common bile duct, which was surrounded by a firm yellowish grey mass. Histologic examination (Fig. 2) showed an infiltrating tumour in the wall of the common bile duct, which was composed of numerous sheets and nests and cords of cells. In some areas tubules had formed. The cells contained a moderate amount of pale granular cytoplasm. Nuclei were central and uniform in appearance. They showed some clumping of chromatin and had small nucleoli. Mitoses were infrequent. The tumour was infiltrating into the immediately adjacent pancreatic tissue, but the resected margins were negative for tumour cells. The tumour had a neuroendocrine appearance. Perineural and lymphatic invasion was noted. All lymph nodes were negative for malignant cells. Immunoperoxidase staining was strongly positive for chromogranin and the tumour was also positive for neuron-specific enolase. The final diagnosis was carcinoid of the common bile duct with perineural and lymphatic invasion.
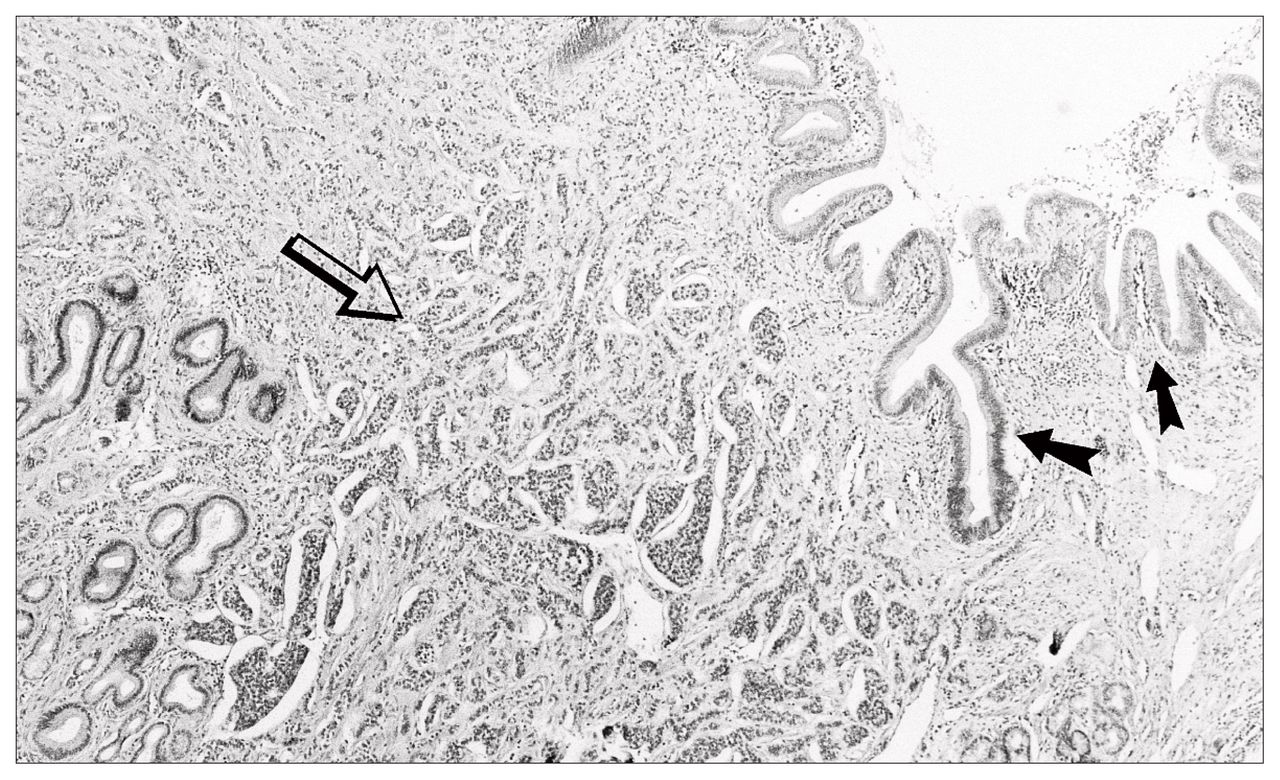
Photomicrograph showing normal common bile duct (black arrows) with tumour infiltration (open arrow) (hematoxylin–eosin stain).
Discussion
Carcinoids of the extrahepatic bile ducts are extremely rare, with only 18 previously reported cases. The term “carcinoid tumour” was first used by Oberndorfer in 19071 to denote a “carcinoma-like” lesion with no malignant qualities. Carcinoids are derived from enterochromaffin cells, which are also known as Kulchitsky’s cells. These cells are located in the bases of Lieberkühn’s crypts.
These cells are also known as argentaffin cells because of their affinity for silver staining compounds. Carcinoids can occur anywhere in the distribution of these cells, which are found scattered among the organs and mucosa of the entire digestive system as well as other body systems.2,3 They are found quite frequently in the ileum and appendix,3–8 where proportionally, more Kulchitsky’s cells are found. The biliary tree has sparse numbers of Kulchitsky’s cells.7,9,10 It has been suggested that there is a pre-disposition to the formation of carcinoids in the biliary tree, caused by chronic inflammation. The process of inflammation in the biliary tree is thought to result in intestinal metaplasia of the biliary mucosa, which causes a relative increase in the number of Kulchitsky’s cells in this area.9–12
All extra-appendiceal carcinoids have variable malignant potential.5,7,9 Carcinoids are composed of multi-potential cells with the ability to secrete numerous hormonal substances, and vasoactive peptides.8 These substances give rise to the clinical features that constitute the carcinoid syndrome. To date, however, there has been no reported case of an extrahepatic bile duct carcinoid being associated with the carcinoid syndrome. Of utmost importance is the primary malignant potential of these tumours, rather than the presence of the carcinoid syndrome.
In reviewing the literature (Table I2–7,9–20) we found that the average age of patients was 47.5 years (range from 19 to 79 years) with a male–female distribution of 43.7% to 56.3%. The predominant symptoms experienced were jaundice, abdominal pain and pruritus. Laboratory investigations were not included in all the previous case reports, but it was evident that the most common laboratory abnormality was an increase in the serum bilirubin level, with a predominant conjugated fraction, and an increase in the serum alkaline phosphatase and γ-glutamyl transferase levels.
Previous Case Reports of Biliary Tract Carcinoids
Abdominal ultrasonography demonstrated dilated intrahepatic or extrahepatic ducts in all cases in which it was performed. Other imaging studies that have been used to aid in diagnosis include CT, ERCP, percutaneous trans-hepatic cholangiography (PTC) and angiography. However, the precise diagnosis of a carcinoid of the common bile duct or other extrahepatic ducts is rarely made without direct histologic and immunochemical examination of the tissue in question.
Of the 18 previously reported cases, 13 were found to have their origin in the common bile duct and 5 had their origin in the common hepatic duct, most frequently at the junction of the left and right hepatic ducts. In our case the tumour arose in the common bile duct. Ten of the previous cases had no evidence of metastatic disease, whereas 5 had liver metastases, 2 had lymph-node metastases and 1 showed portal vein invasion.
The treatment of carcinoids of the extrahepatic bile ducts is surgical excision when possible, based on the exact location of the tumour and the extent of spread at the time of presentation. 3,4,9,10 In our case a pancreaticoduodenectomy was successfully performed with en bloc resection of the tumour and surrounding structures.
Radiotherapy is considered to be of little benefit in the treatment of carcinoids.7,9,10 The experience with chemotherapy of carcinoids in the extrahepatic bile ducts is limited to one case.18 However, it is reported to be of “some benefit” in the treatment of carcinoids occurring in other anatomic locations.7,10 Clearly, the use of this type of therapy will require further investigation.
The prognosis of these tumours is difficult to establish because of our limited experience with them. The literature demonstrates that of the 18 previously reported cases (Table I), 15 provided survival data. Of those, 9 patients were alive (range from 7 days to 20 years); 6 patients died, 4 of them postoperatively. One patient died of suspected pulmonary embolism, 3 weeks postoperatively.
Three patients died 1, 4 and 6 days postoperatively; the cause of these deaths was not reported. One patient died of pneumonia and the diagnosis of biliary tract carcinoid was made incidentally at autopsy. One patient died 10 months after diagnosis of metastases to the liver.
Because of the rarity of carcinoids of the extrahepatic bile ducts, it is difficult to accurately and adequately assess the natural history of this tumour, its malignant potential, the response to different types of therapy and the overall prognosis and survival after treatment. This can only be achieved with continued detailed reporting of single cases, including responses to treatment and long-term follow-up.12 Only with additional information from further case reports can rational and reasonable conclusions be drawn regarding the appropriate treatment and prognosis for this rare tumour.
- Accepted July 9, 1998.
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.