


Abstract
Surgeons caring for severely injured patients have witnessed tremendous change over the past 2 decades with the rapid evolution of trauma systems. This paper describes the evolution of trauma systems in Canada, using the one in Calgary as a model. Canadian system guidelines were produced by the Trauma Association of Canada in 1993. Participation in Canadian accreditation is accelerating as increasingly more centres across the country undergo external review each year. Reporting of trauma outcomes, including standardized mortality and a variety of performance measures, is becoming the norm. Injury is being treated as a disease with comprehensive control strategies aimed at reducing death and disability rates through prevention, treatment and rehabilitation.
Although the concepts of trauma care originate in antiquity, organized comprehensive civilian trauma systems are a relatively new phenomenon. The Royal College of Physicians and Surgeons of Canada launched the Trauma Association of Canada (TAC) in 1983. The Society was founded to provide a multidisciplinary vehicle for the promotion and development of trauma systems across Canada. During the late 1980s, some regional trauma centres received recognition and funding from provincial ministries of health, principally in Ontario. In 1993, the TAC released its guidelines, 1 which were based upon the American College of Surgeons’ document2 but reflected the realities of Canadian trauma care, including a propensity for blunt trauma and greater geographic catchment areas. The guidelines also provided an inclusive model with categories for tertiary, district and rural trauma centres, while maintaining a minimum standard of commitment felt to be essential for providing quality trauma care. Budget cutbacks and restructuring, due to government deficits and debt, precipitated regionalization of trauma services across Canada during the early 1990s. The effects of these changes are ongoing; however, they certainly have focussed attention and in some cases accelerated the development of regional trauma systems across the country. A voluntary system of accreditation has been promoted by the TAC and has seen active participation by many tertiary trauma facilities.
Responsibility of a trauma centre
The responsibility of a tertiary trauma centre is not only to provide complete, coordinated and efficient care but to enhance the entire trauma system through a variety of activities. These include outreach activities, education, and injury prevention and control, as well as development of the data system, including registry and injury surveillance. The centre must also establish cooperative relationships, good communication, transport and bypass agreements with primary and secondary hospitals in the region to complement the entire trauma system.3 A simplified schematic of a regional trauma system is illustrated in Fig. 1.
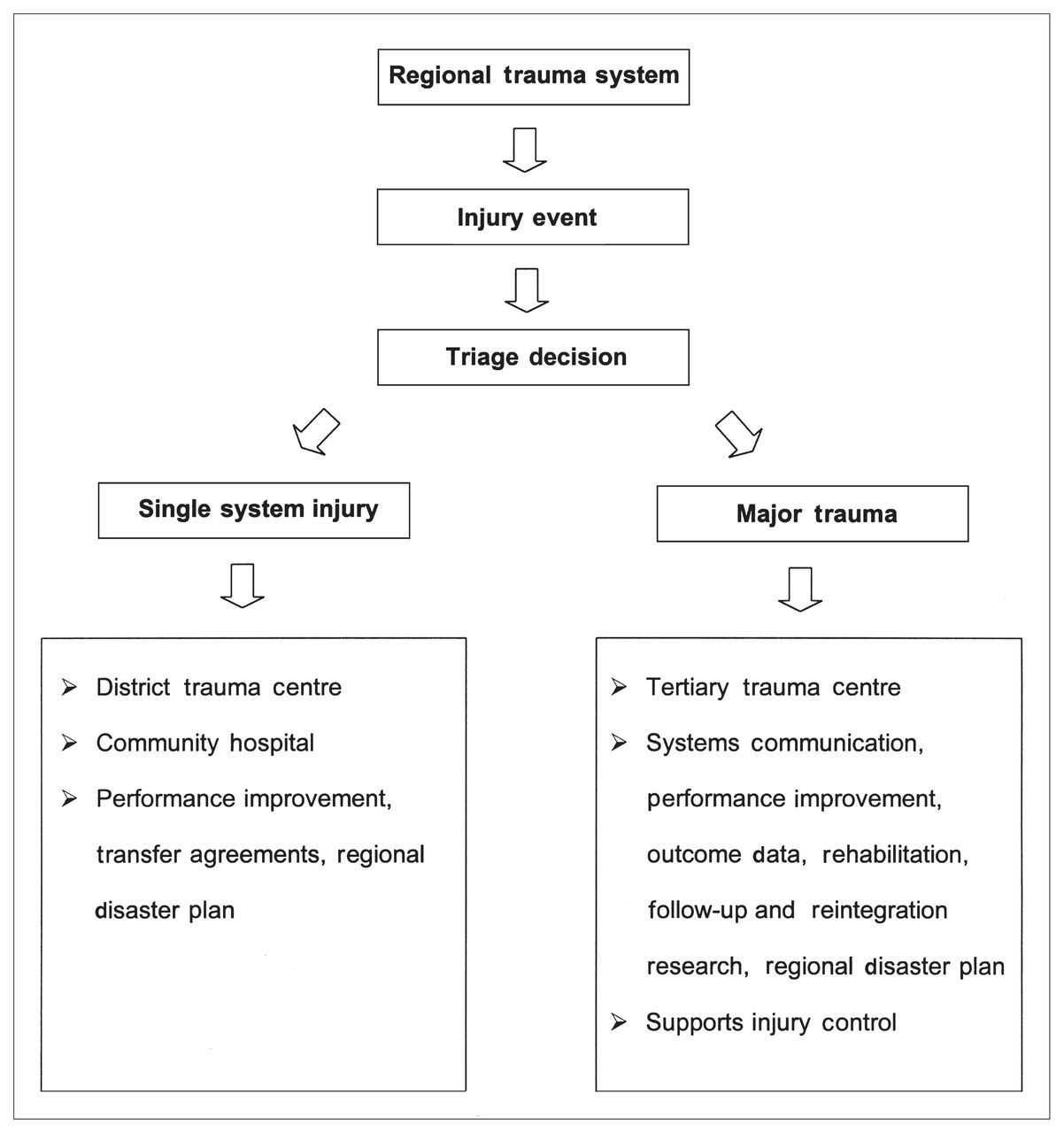
Schematic diagram of a simplified regional trauma system.
Indexes for major trauma
Major trauma has often been defined as being present in patients with an Injury Severity Score (ISS) greater than 16 whose risk of death was more than 10%, as defined by the major trauma outcome study.4 Injury severity scoring, however, is retrospective, and major trauma presents as part of a continuum from minor to lethal injury. Studies of inclusive systems suggest that of all injuries presenting to hospital, 5% to 10% require the resources of a tertiary trauma centre.5,6 In addition, the spectrum of injury extends from severe life-threatening polytrauma to outpatient injuries.7 This is best illustrated by the injury pyramid (Fig. 2). The trauma system accreditation guidelines, developed by the TAC in 1993, attempt to address the need for an inclusive model of a trauma system.

The injury pyramid.
Identifying patients who potentially have multiple injuries consistent with major trauma and who would benefit from trauma treatment in a tertiary level trauma facility, has been a goal of the prehospital system. A variety of triage tools have been proposed and studied, including the Trauma Score8 and CRAM’s scale.9 The prehospital index (PHI),10 in conjunction with the mechanism of injury (MOI), was assessed by a prospective study in the Calgary region over a 6-month period, analysing more than 3000 emergency medical service (EMS) injury transports.11 The combined score had 89% specificity and 78% sensitivity for detecting major trauma (Table I). The majority of patients in whom high ISSs were missed were the elderly who had falls from standing heights. The study concluded that PHI/MOI triage was effective but emphasized that any triage system should be tailored to the individual requirements of the community in which it is to be used.
Effectiveness of the Triage Tool Used to Treat Patients Admitted With Blunt Trauma*
Transportation of trauma patients
Any evaluation of a Canadian trauma system must also reflect the reality that half of the patients presenting to the tertiary centre are transported from rural and regional centres, often covering great distances over many hours.12 The quality of air ambulance transfers was assessed by van Wijngaarden and colleagues,13 who demonstrated inappropriate care in less than 6% of cases and a very small overtriage rate of 5%. The study concluded that, given the difficulty of triage, the air ambulance system was likely underutilized. Many factors determine time from injury to tertiary care including pre-primary hospital time, time in the originating hospital before contacting dispatch and, finally, organization of the air ambulance transport system. Appropriate selection of patients who are physiologically unstable for rapid evacuation and transport also remains controversial. 14 These are all items of ongoing interest. Many centres have developed trauma hotlines or rapid access lines. The Calgary region now has a single 1–800 number for critically ill and injured patients, providing immediate access by rural physicians to the receiving tertiary trauma or critical care team, as well as the emergency flight physicians and the dispatch centre.
Measures for evaluating trauma centres
Do trauma centres make a difference? A heterogeneous population, multiple health professionals and caregivers, and a variety of health organizations all are factors that challenge our ability to scientifically validate the effectiveness of trauma systems. Despite these challenges, a large body of evidence now supports the effectiveness of regionalized trauma systems. 15–20 The development of trauma registries has allowed the science of injury to progress.21 These comprehensive databases have evolved to allow prospective data entry on severely injured patients. They support performance improvement through the review of cases identified by standard audit filters and death reviews. Research on outcomes and effectiveness, injury surveillance and support for allocation of resources are all benefits of the tool.22 Analysis of the Trauma Injury Severity Score (TRISS), based on a major trauma outcome study, has been one method of survival analysis.23 Most organized centres today report TRISS outcomes and z scores, demonstrating a significantly improved outcome compared with major trauma outcome study (MTOS) data. The z score shows whether there is a significant difference between the centre’s overall mortality and survival statistics and MTOS data.24 The W statistic indicates the actual increased or decreased number of survivors per 100 trauma admissions. The M statistic is used to demonstrate whether the populations match.
TRISS analysis is limited, however, because it is a rather crude measure of outcome, and many patients who present to trauma centres that have registries are already intubated and initial physiologic data required for TRISS is not available.25 These patients often represent the more seriously injured ones with higher mortality. Other techniques used to examine the effectiveness of particular trauma systems include internal and external death and morbidity reviews that study preventable and potentially preventable deaths and complications. Finally, examination of specific injury cohorts has been an effective means of the examining outcome. Smith and colleagues26 demonstrated a significant reduction in death and complication rates in patients treated at trauma centres, compared with nontrauma centres, based on discharge abstract data and patient management categories. Nakayama and colleagues27 examined outcomes of childhood trauma in the Pennsylvania trauma system. On the basis of TRISS analysis, they reported higher pediatric death rates in rural trauma centres. Cales,28 in a landmark article in 1984, demonstrated significant improvements in potentially preventable morbidity and mortality after the introduction of organized trauma care in Orange County. In 1995, Stewart and colleagues29 demonstrated a significant increase in survival of 6% after Ontario Ministry of Health designation. Finally, a variety of performance indicators measure the effectiveness of trauma systems (e.g., prehospital time, time to laparotomy). These are now appearing in the public domain, with some systems publishing their results on their Web sites (e.g., www.trauma.org, a British trauma site with links to many trauma centres).
Canadian evaluation of trauma systems is ongoing with attention to defining essential elements. Two important publications have originated from changes in the Quebec system. Sampalis and colleagues30 demonstrated the effectiveness of regional bypass with destination policies in urban trauma systems. They then presented the results of an ambitious project analysing the effects of regionalization and the development of a trauma care network from 1992 to 1998.31 The death rate in major trauma patients (ISS greater than 12) fell from 52% to 18%. The large study population also permitted assessment of trauma system components and their relative impact, including prehospital time, trauma centre designation and transfer versus direct transport. In 1996, a trauma program with a dedicated clinical trauma service was introduced in Vancouver.32 Important reductions in delays to the operating room, length of stay in the trauma unit and TRISS mortality resulted.
Injury control
Injury control is a term increasingly used to reflect a comprehensive approach to the disease of injury.33 It represents a systems approach, including injury prevention, education and treatment through to rehabilitation and reintegration. The cure for injury is prevention. Injury continues to be the leading cause of death in the first 4 decades of life, and challenges cancer and heart disease for overall potential years of life lost.34 Per capita, fatalities due to motor vehicle collisions have been falling in Western countries since 1965 (Fig. 3). This presumably is a result of improved vehicle safety design, traffic regulation and enhanced trauma systems, as well as general awareness and education.35 Further reductions in deaths due to motor vehicle accidents are obtainable as evidenced by the Victoria, Australia, casualty crash initiative.36 This effort achieved a mortality reduction of almost 50% between 1990 and 1992. Further reductions are possible but only through heightened public awareness and education, stricter enforcement and effective lobbying for changes in legislation. Health restructuring and cutbacks have focussed attention on injury control and have seen developments across the country.

Comparison of the number of fatalities per 100 000 motor vehicles in Canada (diamonds), the United States (squares), the United Kingdom (triangles) and Australia (crosses) for 1960, 1970 and 1992.
Alberta has recently funded a provincial office of injury control. The objectives of the centre are to promote comprehensive solutions including enhanced injury surveillance, adoption of TAC guidelines, changes in public awareness, enforcement and legislation. Similar programs are evolving across North America.37–39 In addition, 1997 saw the launch of the National Trauma Registry by the Canadian Institute for Health Information in conjunction with the TAC.40 This important project will support national injury surveillance as well as population-based research on injury and trauma. In 1999, a proposal to link TRISS results from Canadian trauma centres and develop a national benchmark, CTRISS, was presented at the TAC meeting in Montreal. Despite these improvements, research dollars are also necessary to drive evidenced-based improvements in the system. Injury research remains grossly underfunded relative to other health care problems, particularly in view of its significance as a public health problem.41
Summary
Trauma system development has made great strides. Trauma systems and injury control remain heterogeneous across the country. National guidelines and associations represent a powerful tool for committed individuals and organizations to ensure that quality is not compromised and that this important problem is addressed. This is particularly relevant during a time of rapid change and fiscal restraint during which health care traditions are continually challenged. The Ottawa-Carleton system, applying a model assessing cost per quality-of-life year gained, has confirmed the cost-effectiveness of trauma systems in Canada.42 Trauma will continue to strike down, through loss of life and limb, many productive members of our society in the coming years. The value of investing time and energy in enhanced injury control is apparent.
Footnotes
Part of the symposium “What’s New in Trauma Care?” presented at the 66th annual meeting of the Royal College of Physicians and Surgeons of Canada, Vancouver, BC, Sept. 26, 1997.
- Accepted July 9, 1999.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.