


Abstract
Objective: To study injury patterns of snowboarding trauma in children.
Design: A retrospective case series.
Setting: A major pediatric trauma centre.
Patients: A cohort of 113 children (97 boys, 16 girls), mean age 13.9 years, who sustained 118 injuries secondary to snowboarding.
Interventions: All fractures were treated by immobilization in a cast; 19 children required a closed reduction.
Outcome measures: Sex and age of patients, mechanism of injury, injury sustained, treatments and complications.
Results: Falls on the outstretched hand from a loss of balance accounted for 66 (57%) of the injuries, uncontrolled falls for 42 (36%) and collisions for 5 (4%). Seventy-nine percent of the injuries were to the upper extremity, whereas 7% were to the lower extremity.
Conclusions: The predominance of snowboarding injuries of the upper extremity seen in children differs significantly from those in adults in whom lower extremity injuries are more common.
Snowboarding is rapidly increasing in popularity among teenagers. It is a marriage of the speed from alpine skiing with the carefree and daring attitude of skateboarding and surfing. Because of this burgeoning popularity, some ski resorts are reserving 30% to 50% of their runs for the exclusive use of snowboarding. With a 40% to 100% yearly increase of participants during the 1990s and rapid influx of novices there has been a concomitant increased flow of injured patients into our emergency rooms. Many studies have outlined the injury patterns seen with skiing in both the general population and in children.1–12 However, the literature on snowboarding has only examined injury patterns for the general population, without focusing specifically on children.1–26 Because of the escalating numbers of children entering our fracture clinics with injuries sustained while snowboarding, we felt that this issue required closer examination.
Method
A retrospective review of all Emergency Department charts at the Children’s Hospital of Eastern Ontario, Ottawa, pertaining to winter sports injuries between January 1990 and May 1998 were examined for any injuries sustained as a result of snowboarding. For each patient, the sex, age, mechanism of injury, injury sustained, treatments involved, complications and follow-up were noted.
Results
The charts revealed a total of 113 children (97 boys, 16 girls) who suffered 118 snowboarding injuries. The average age was 13.9 years (range from 6 to 18 years). The distribution of the injuries during the winter months followed a normal curve, with the majority occurring in January and February.
Falls onto the outstretched hand from loss of balance on the snowboard accounted for 66 (57%) of the injuries, whereas uncontrolled falls (complete loss of control of the direction of the snowboard) were responsible for 42 (36%) and collisions with other skiers or snowboarders accounted for 5 (4%) injuries.
Injuries to the upper extremity (Fig. 1), including the shoulder girdle, were encountered in 93 (80%) of the 118 injuries. Lower extremity injuries occurred in only 8 (7%) cases, head injuries in 9 (8%) and abdominal injuries in 6 (5%). Injuries to the growth plate occurred in 12 (10%) cases (Fig. 2), with no apparent overt growth disturbances. Fractures of the distal radius were the most common injury, in 53 (46%) cases (Table 1). Of the 66 injuries attributed to a fall on the outstretched hand, 58 (88%) resulted in a fracture of the distal radius (30 right, 28 left) (Fig. 3).

Displaced fracture of the medial condyle in a 14-year-old boy (top), which required open reduction and internal fixation (bottom).
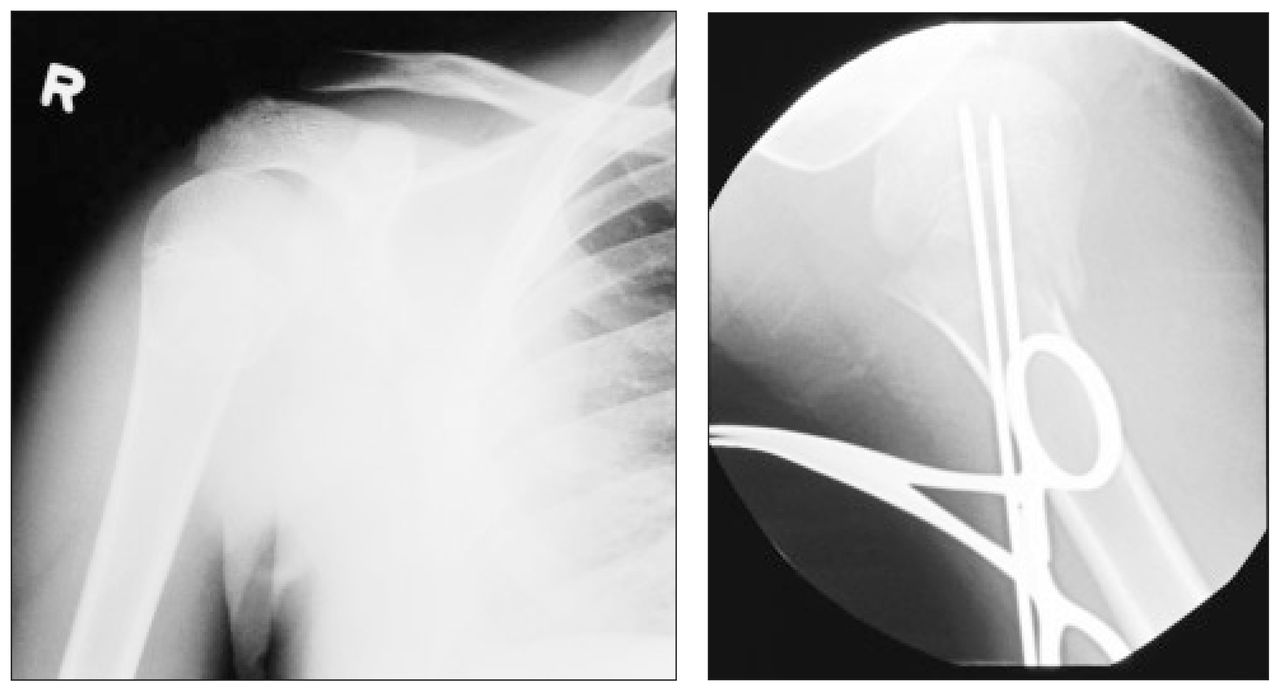
Type II physeal fracture of the proximal humerus in a 15-year-old boy (left) sustained when he lost control and fell backward from the snowboard. This fracture required closed reduction with percutaneous pinning (right).

A typical fracture of the distal radius and ulna in a 15-year-old boy, sustained in a forward fall after he lost control in a jump.
Site and Type of Injury in Children With Snowboarding Trauma
Closed reduction was attempted under intravenous sedation in 19 children, but 10 required general anesthesia for final reduction. In total, 13 children underwent closed reduction under a general anesthesia in the operating room. Two patients had a closed reduction supplemented with percutaneous pin fixation. One had an associated unstable, displaced physeal proximal humeral fracture, the other had loss of reduction of a Salter–Harris II distal radial fracture 1 week after an initially acceptable closed reduction. One child with a closed mid-diaphyseal injury to the forearm on his non-dominant side sustained an ulnar nerve deficit postoperatively. He recovered to grade 4/5 motor strength by 12 weeks before he was lost to follow-up. Follow-up of 3 months or longer was available for 75% of the children.
The most serious lower extremity injury was a spiral fracture of the femur. Four medial collateral ligament strains of the knee, 2 type I fractures of the fibula and a fifth metatarsal fracture made up the remaining lower extremity injuries. Nine children were admitted and detained for observation for mild cerebral concussion, none of which required surgical intervention. All children were wearing protective headgear.
Discussion
Over the past 15 years, snowboarding has emerged as the fastest growing sport in North America and is now represented in the Winter Olympics. Injuries to participants are expected, especially as beginners progress along the learning curve. Although not specifically noted in the charts, it has been our observation that snowboarders presenting to our clinic were most frequently novices who had typically been snowboarding fewer than 10 times.1,2,3,4,7–9,14,16–19,25 The pattern of injuries noted in our pediatric population were clearly distinct from those that occur in skiers1–12 or in adult snowboarders.1–5 The greatest number of injuries were isolated to the upper extremity (80%), with distal radial fractures accounting for 46% of the injuries. The mechanism of injury was usually a mistimed heel- or toe-turn, and because both feet are bound to the board, the snowboarder sustains a direct unbroken fall onto the outstretched hand. There were only 2 patients with scaphoid fractures, reflecting the more cartilaginous composition of the pediatric scaphoid, even though the mechanism leading to injury in 57% was a fall onto the outstretched hand.
Adult studies have demonstrated that patients presenting for medical attention because of a snowboarding injury are typically male (50% to 90%), with an average age between 19.1 and 21.6 years.1,2,4,5,7–9,14–19,25 The children in our study were 5 to 7 years younger, having an average age of 13.9 years. The association between beginner status and increased injury rate, particularly with injuries to the upper extremity, has been drawn in many series in the literature.5–10,18 In a group of 355 injured snowboarders, Chow and associates7 found that 44% of those injured were in their first season of snowboarding, and 19% were snowboarding for the first time when they received the injury. Zollinger and colleagues18 in their series of 180 patients noted that 20% were beginners and half were in their first season. Of the 73 snowboarders responding to a questionnaire, Abu-Laban5 reported that 36% were novices and 61% were in their first year of snowboarding. Bladin and associates8 reported that 58% of their patients were in their first season.
Lower extremity injuries were surprisingly rare in our review (7%). This is likely a reflection of the young age of our patients and therefore of a less advanced skill level at snowboarding. The association between experience and lower extremity injuries and their patterns has been documented.1,2,4,5,7–9,14–19,25 In some studies the association is confounded by the fact that most novices begin with hard-shell boots, which tends to be associated with tibial and knee injuries, whereas intermediate and advanced snowboarders tend to use soft-shell boots, which are associated with an increased rate of ankle injuries. When the mechanism of injury is examined specifically in the literature,4,5,10,15,18,21 the forward, or lead, leg is the lower limb injured in up to 80% of patients. This was also our experience in the smaller number of lower limb injuries seen in children. This reflects the greater amount of torque applied to the forward leg as the body weight transits from behind to excessively far to the front or side of the leg. In the uncontrolled falling state, the change of necessary stabilizing muscular forces to prevent supraphysiologic strain is exceeded, leading to injury. The “snowboarder’s fracture”23,24 — a fracture of the lateral process of the talus — was not seen in this study, possibly because the lateral process is more cartilaginous in children.
Abdominal injuries from snowboarding were highlighted by Prall and colleagues11 as the forward falling snowboarder, with the left side of the body leading, lands with the left elbow adducted against the left upper quadrant. This predisposes particularly to splenic injury, so casualty officers must be cognizant of this possible relationship with snowboarding. Our abdominal injuries consisted of an anterior abdominal wall “hematoma,” a splenic laceration, a renal hematoma and a renal contusion with splenic laceration, in 1 child each.
Spinal injuries are rare in children and tend to result from high-risk aerial manoeuvres. Genelin and associates12 reported that adult snowboarders are particularly prone to cervical spine injury. Our only spinal injuries, aside from coccygeal contusion in 2 children, consisted of a cervical strain (and concussion) in a 12-year-old boy and an undisplaced fracture of C7 (Fig. 4) in a 17-year-old girl. Both injuries healed well with no neurologic sequela. In the adult series reported by Abu-Laban,5 12% of the patients had spinal injuries

A 17-year-old girl sustained a hyperflexion injury to her cervical spine in a high-speed snowboarding accident, shown in the lateral radiograph (top) and the computed tomography scan (bottom).
From our review it is apparent that there is a difference between patterns of adult snowboarding injuries reported in the literature and those seen in children. In younger patients there is a marked propensity for injury to the upper extremity. The distal radius is particularly at risk in this age group, as evidenced by the 46% rate of children sustaining a radial fracture. Although there are several weaknesses in this review, including its retrospective nature, the exclusion of the large number of children with minor injuries (sprains, undisplaced fractures), which are usually seen and treated in urgent care clinics and community hospitals, and a database of medical records that does not specifically note the mechanism of injury unless recorded by the examiner, we are confident that most of the significant trauma secondary to snowboarding in our area has been identified.
Many authors have concluded that wrist guards and formal instruction should be mandatory for novice snowboarders. We would agree that, given the large proportion of fractures of the distal radius in the pediatric population, the use of wrist guards similar to those used by in-line skaters should be used by all skeletally immature snowboarders. The theoretical concern that use of wrist guards may predispose to more proximal upper limb injury has not been demonstrated. Given the frequency of wrist injuries, we feel that this theoretical risk cannot outweigh the real risk of fracture to the unprotected wrist of a snowboarder. As we did not directly examine the issue, we cannot make any recommendations regarding the preferential use of soft- or hard-shelled boots, or specific types of bindings. Bjornstig and Bjornstig15 recommended the development of a release mechanism for the boots–board bindings, as well as the use of soft-shell boots for all snowboarders. Soft-shell boots have been associated with a higher incidence of lower extremity injuries, particularly to the ankle.
Conclusions
The pattern of injuries from snowboarding seen in a pediatric emergency room setting is clearly different from that described in the literature for the adult population, with a much greater susceptibility to upper extremity fractures in children.
Mandatory safety training for children under the age of 17 years prior to participation, with instruction in proper equipment, risk avoidance and falling techniques should help novice snowboarders protect themselves from avoidable high-risk situations and should be strongly encouraged.
- Accepted August 22, 2000.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.