


A 65-year-old man underwent barium enema examination for investigation of rectal bleeding. Sigmoid diverticular disease was diagnosed, but in addition the vermiform appendix was noted to be lying within an asymptomatic right inguinal hernia (Fig. 1). In addition to appendiceal diverticula, multiple fecaliths were evident within the lumen of the appendix. The patient was therefore at risk for the development of appendicitis in the hernial sac (Amyand’s hernia1,*). He underwent simultaneous hernia repair and appendectomy (Fig. 2) with broadspectrum antibiotic prophylaxis. His postoperative course was smooth, without wound complications or hernia recurrence.

Barium enema examination showing the vermiform appendix in a right inguinal hernia.

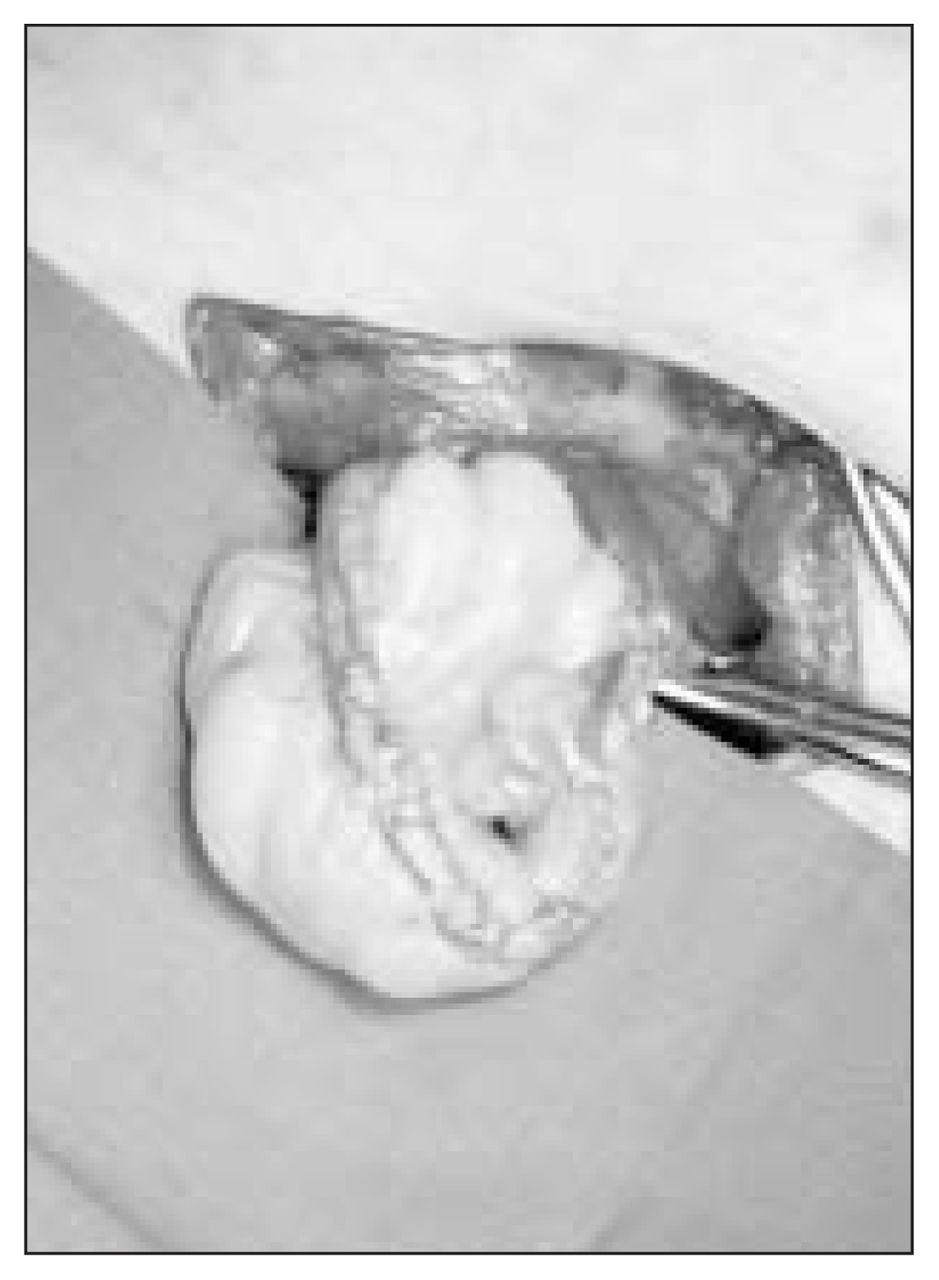
Operative view showing the vermiform appendix in a hernial sac.
Only rarely is the diagnosis of an appendiceal inguinal hernia made preoperatively.2 Even with perforation, appendicitis in this unusual position is difficult to diagnose.3 If the vermiform appendix is encountered unexpectedly in a hernial sac during elective herniorrhaphy, the risk of appendicitis (e.g., the presence of fecaliths) should be weighed against the risks of wound or mesh infection, and of hernia recurrence,4 when deciding on a concomitant appendectomy. 5
Footnotes
↵* Claudius Amyand (1681–1740), Sergeant-Surgeon to King George II and Principal Surgeon to St. George’s Hospital, London, UK. In 1735 he performed the first appendectomy for a discharging fecal fistula due to a perforated appendix in an inguinal hernia.1
Section Editors: David P. Girvan, MD, and Nis Schmidt, MD
In this issue

{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.