


Abstract
Objective: To study the vertebral involvement of the cervical spine, in particular the stability of C1–C2, in children with proven Goldenhar’s syndrome.
Design: A case review.
Setting: The Children’s Hospital of Eastern Ontario, Ottawa.
Patients: Eight children who had a minimum of 2 out of 3 Goldenhar criteria plus other strong associations with the syndrome and for whom detailed radiographic spinal assessment, including flexion–extension views of the cervical spine and computed tomography of the congenital anomalies, were available.
Outcome measures: Radiographic findings.
Results: Seven children demonstrated cervical spine anomalies. Of particular concern was the high incidence of C1–C2 instability in 3 children, 2 of whom required occiput to C2 fusion. The presence of hemivertebrae and failures of segmentation were most common and resulted in thoracic scoliosis, leading to spinal fusion in 2 children.
Conclusions: In patients with Goldenhar’s syndrome the cervical spines must be monitored carefully for C1–C2 subluxation before any proposed surgery for other malformations associated with the syndrome, so that any instability can be identified to avoid cord impingement during a general anesthetic.
The term Goldenhar’s syndrome is now synonymous with oculoauricular vertebral dysplasia. In 1952, Goldenhar1 described a syndrome of congenital malformations consisting of epibulbar dermoid appendages and preauricular skin tags. In 1963, Gorlin and Pindborg2 added to this the association of vertebral anomalies.
Patients with Goldenhar’s syndrome often have other abnormalities such as hemifacial microsomia, micrognathia and cardiac and renal defects.1–7 These features are frequently apparent but are not essential inclusion criteria. Those sufferient from this syndrome have a broad spectrum of involvement of part or all of the oculoauricular vertebral triad. The initial literature was more focused on the facial dysmorphic features, but recently concerns have been focused on the more disabling aspect of spinal deformity.8,9
The incidence of the syndrome has been quoted as ranging from 1 in 3000 to 1 in 5000 live births. An embryologic study in rats indicated that the defects may be in part attributable to disruption of development in the first and second branchial arch regions due to interference with the blood supply.10 The embryologic stapedial artery is responsible for blood supply in this region. Interrupting this blood supply in animal studies mimics the auricular and some of the vertebral manifestations, but the ocular component has been difficult to duplicate.11,12 There is no confirmed genetic component in spite of reported cases of an autosomal dominant pattern and trisomy 8, 9 and 22 occurrences.13 Monozygotic twin disconcordance and lack of an identifiable genetic abnormality in most cases do not support a genetic cause.14
The purpose of our study was to focus on the vertebral involvement of the cervical spine, in particular the stability of C1 and C2, in children treated at our centre with proven Goldenhar’s syndrome and with radiographic documentation of cervical spine stability.
Methods
All children with Goldenhar’s syndrome seen at the Children’s Hospital of Eastern Ontario, Ottawa, between 1974 and 1995, were considered for the study. Inclusion criteria included a minimum of 2 out of 3 Goldenhar criteria plus other strong associations with the syndrome. Over this 21-year span, 17 such children who met the criteria were identified from both inpatient and outpatient records. One patient was lost to follow-up and was excluded. For the remaining 16 patients we reviewed the complete radiographic record. Only plain chest films, including cervical to sacral spine were available for 8 patients, and they were excluded from the review. The remaining 8 children (3 boys, 5 girls) had more detailed radiographic spinal assessments, including flexion–extension views of the cervical spine and computed tomography of the congenital anomalies. These made up the study population.
Findings
Of the 8 patients, 1 boy had died by the time of our study (Table 1), as the result of a car accident. Six of the 8 patients had serious cervical spine abnormalities involving multiple areas of failure of segmentation and formation, often with severe rib malformation (Fig. 1). Odontoid hypoplasia (Fig. 2) with C1 to C2 instability greater than 5 mm, was demonstrated in 3 patients (Fig. 3), 2 with atlantoaxial instability greater than 7 mm requiring occiput to C2 fusions (Fig. 4) due to associated occipital and cervical instability. Only 1 of the 8 patients had no congenital malformations of the spine but had a thoracolumbar scoliosis. Of the 8 patients, 5 had thoracic congenital vertebral malformations consisting of hemivertebrae or fused vertebrae that caused scoliosis, and in 2 children spinal fusion was required.

Failure of segmentation of the cervical spine in a 5-year-old child (patient 4) demonstrating 5 mm of C1–C2 instability (black arrows). White arrows depict the anterior tip of the atlas, which is subluxated forward.

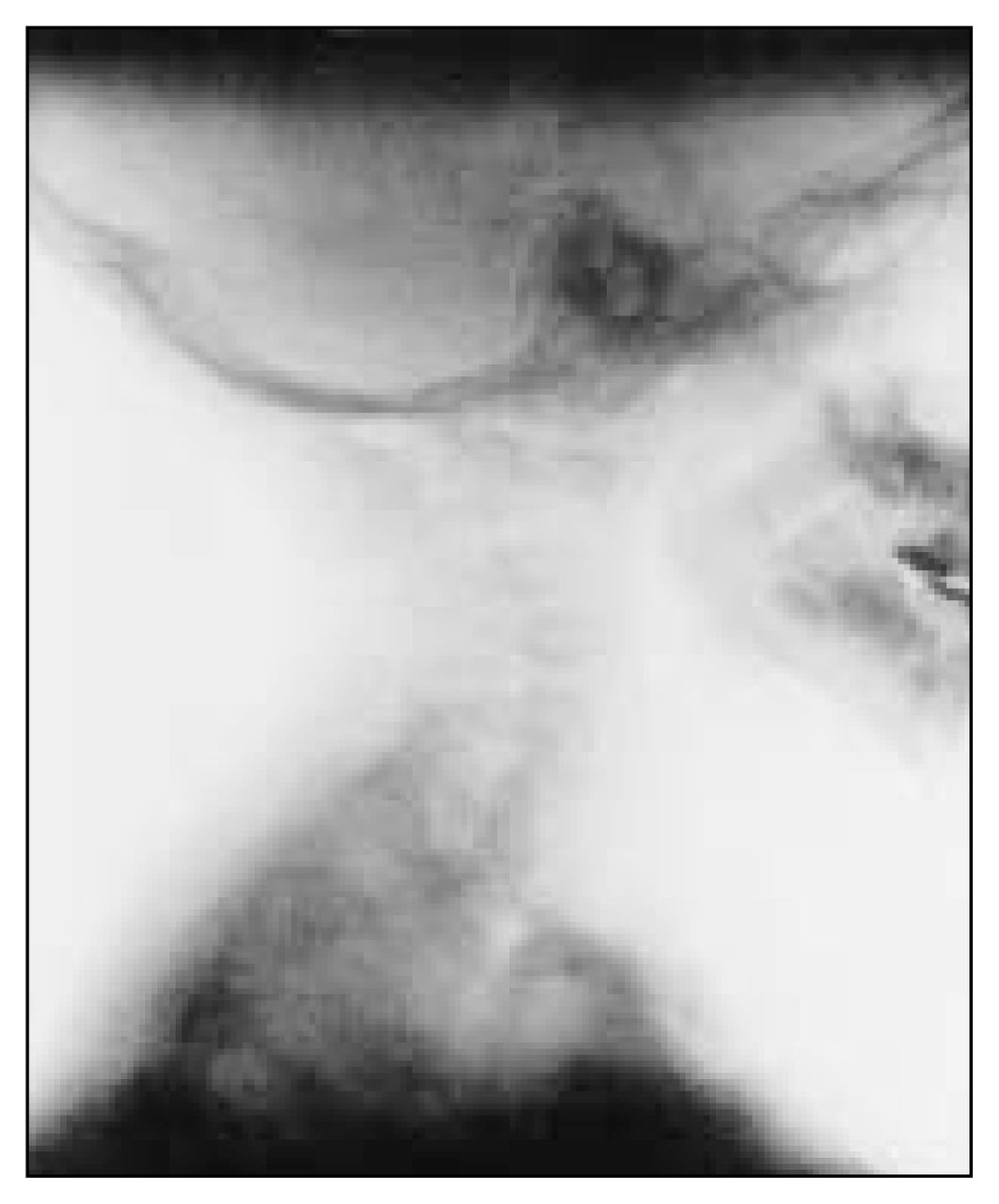
Hypoplastic odontoid process in a 15-year-old patient (no. 7).

Extension (left) and flexion (right) views of the cervical spine of patient 8, lllustrating C1–C2 instability at 3 years of age. Black arrows = platybasia of the occiput, white arrows = anterior subluxated portion of the atlas.
Cervical occipital fusion for C1–C2 instability and occipitalization of C1 in a 4-year-old girl (patient 1).
Demographics of 8 Children With Goldenhar’s Syndrome and Spinal Defects
Our review also identified that 4 of the patients, including 2 with atlantoaxial instability before diagnosis, had had general anesthesia for various nonspinal surgical procedures.
Discussion
Children with Goldenhar’s syndrome have a high incidence of congenital malformations of the cervical spine including odontoid hypoplasia that puts them at particular risk during general anesthesia.15 In this series, 2 children required surgery on the cervical spine because of C1–C2 instability greater than 5 mm and associated pseudobasilar invagination (vertical migration of the odontoid process). Unfortunately, children with Goldenhar’s syndrome have many other malformations that would necessitate surgery under general anesthesia. For this reason we believe that all such children should have the cervical spine assessed for instability before they undergo any general surgery. Children with C1–C2 instability may not exhibit clinically symptomatic features of cervical spine instability until near skeletal maturity.8 Once diagnosed with Goldenhar’s syndrome, asymptomatic children can be monitored by flexion–extension views at 6month intervals, and activity can be modified to minimize a catastrophic event.8 If the C1 displacement exceeds 6 mm, C1–C2 fusion should be considered.8,11,16
There is some similarity between the Klippel–Feil syndrome and children with Goldenhar’s syndrome, but the former is not associated with other anomalies of the ear and eye. Unrecognized cervical instability may place the patient at great risk at the time of intubation due to excessive cervical spine manipulation or result in cord impingement during sports activities. Frequent surgical procedures and difficult intubation in these children owing to the facial anomalies, the small asymmetrical jaw and limited neck mobility place the child at high risk. The presence of a cervicothoracic scoliosis will also often complicate the intubation by deviating the trachea. Nasal intubation with fibreoptic visualization may be indicated.
Occipitocervical fusion was necessary in 2 patients with atlantoaxial instability greater than 7 mm, due to associated occipitalization of C1, an anomaly that appears to be more frequent in children with Goldenhar’s syndrome (Fig. 4). Both patients who underwent this procedure have done well postoperatively although there is always concern about the effect of occipitocervical fusion on rotation in children. We would advocate treating an asymptomatic instability greater than 6 mm in a child because catastrophic spinal cord impingement as well as increased loss of motion may occur if the cervical fusion is delayed until adulthood.15
It has been estimated that there is a 12% incidence of platybasia and occipitalization of C1 in children with Goldenhar’s syndrome.7 This suggests that there may be a malformation of the occipital plate as well as dysplastic development of the first and second branchial arches. Pseudobasilar invagination associated with occipital–C1 instability was also noted in 1 patient.2
Of the 8 children in our review, there was no family history of Goldenhar’s syndrome, and no chromosomal abnormalities were detected. This supports the well-documented heterogenicity of etiology of this condition. In a recent review by Gibson and associates,7 7 of 35 children had a defect in vertebral formation of the cervical spine and 21 had spinal malformations. However, their inclusion criteria was the presence of only 1 of Goldenhar’s basic criteria whereas we used 2 for our inclusion criteria.
In general, children with Goldenhar’s syndrome and spinal malformations are shorter than normal, as we found in our study. Even though there were considerable vertebral malformations, intraspinal anomalies were not detected in this group although only 3 of the children underwent magnetic resonance imaging. Scoliosis to date has occurred in 2 patients and required stabilization in 1, with fusion and instrumentation for progressive scoliosis greater than 50° by the Cobb measurement.
The high rate of cervical malformations and instability must be investigated in children with Goldenhar’s syndrome before reconstructive surgery is carried out. Such children should have adequate imaging of the cervical spine along with flexion and extension views to detect any instability before general anesthesia is induced.
- Accepted January 28, 2002.
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.