


A 36-year-old man presented with a 4-week history of intermittent right upper quadrant pain, radiating to the back. No abnormalities were found on physical examination and blood tests. Abdominal ultrasonography showed gallstones and multiple hyperechoic masses in an enlarged spleen. Computed tomography (Fig. 1) demonstrated multiple hypodense lesions up to 3 cm in diameter, replacing 40% of otherwise normal splenic parenchyma. No other abnormalities were noted. The referring hematologist and the radiologist raised concerns of this being a primary splenic lymphoma. Laparoscopic cholecystectomy and splenectomy were scheduled.

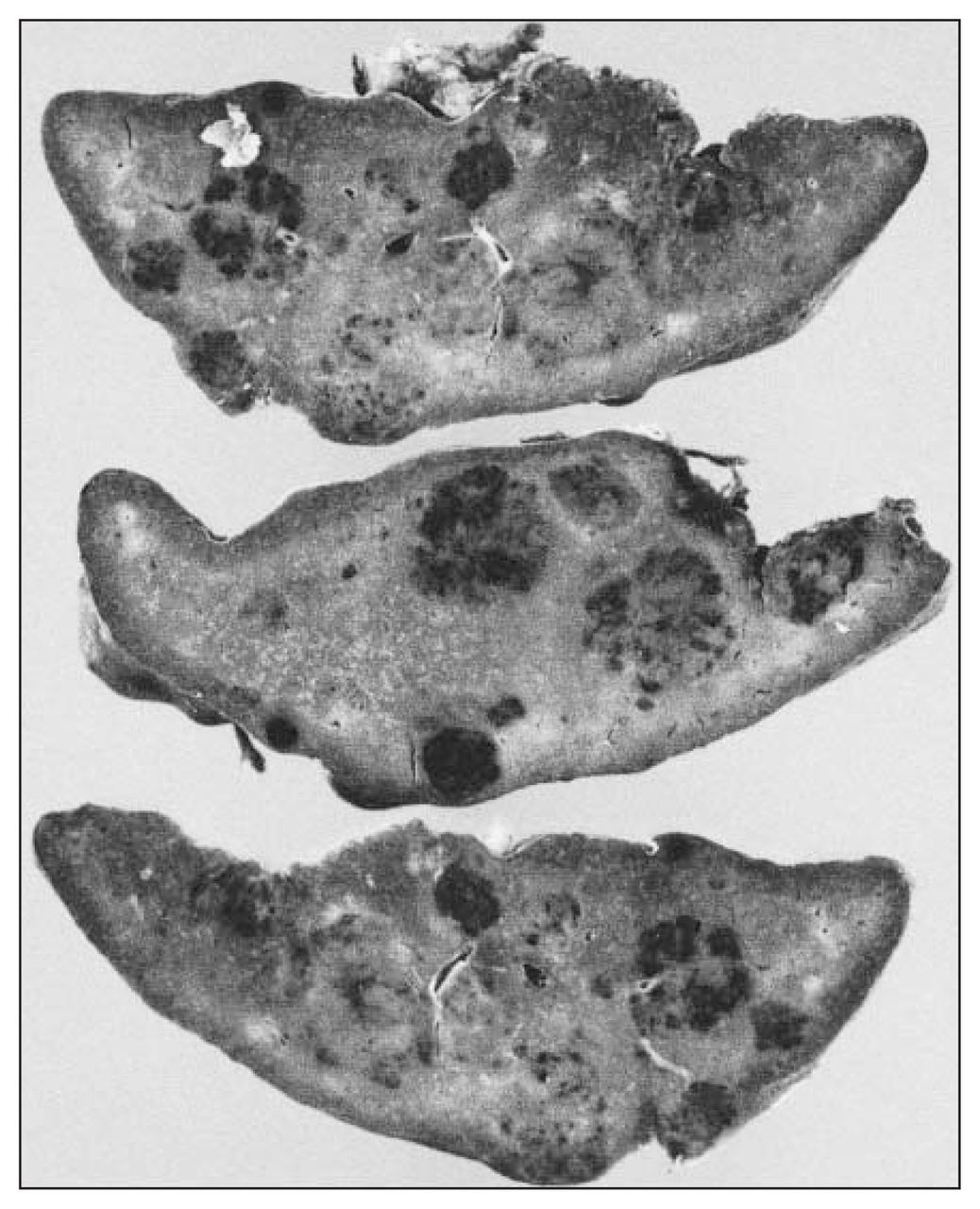
At laparoscopy, dense right upper quadrant adhesions, abundant intra-abdominal fat and inadequate visualization of the anatomy of the area prompted conversion to an open procedure. The gallbladder and spleen were removed without complication. Pathological examination of the gallbladder showed cholelithiasis and chronic cholecystitis. Grossly, the spleen weighed 500 g and measured 22 × 11 × 5 cm. The red pulp contained tan, spongy nodules, ranging in size from 0.5 to 3 cm (Fig. 2). The intervening splenic parenchyma was unremarkable.
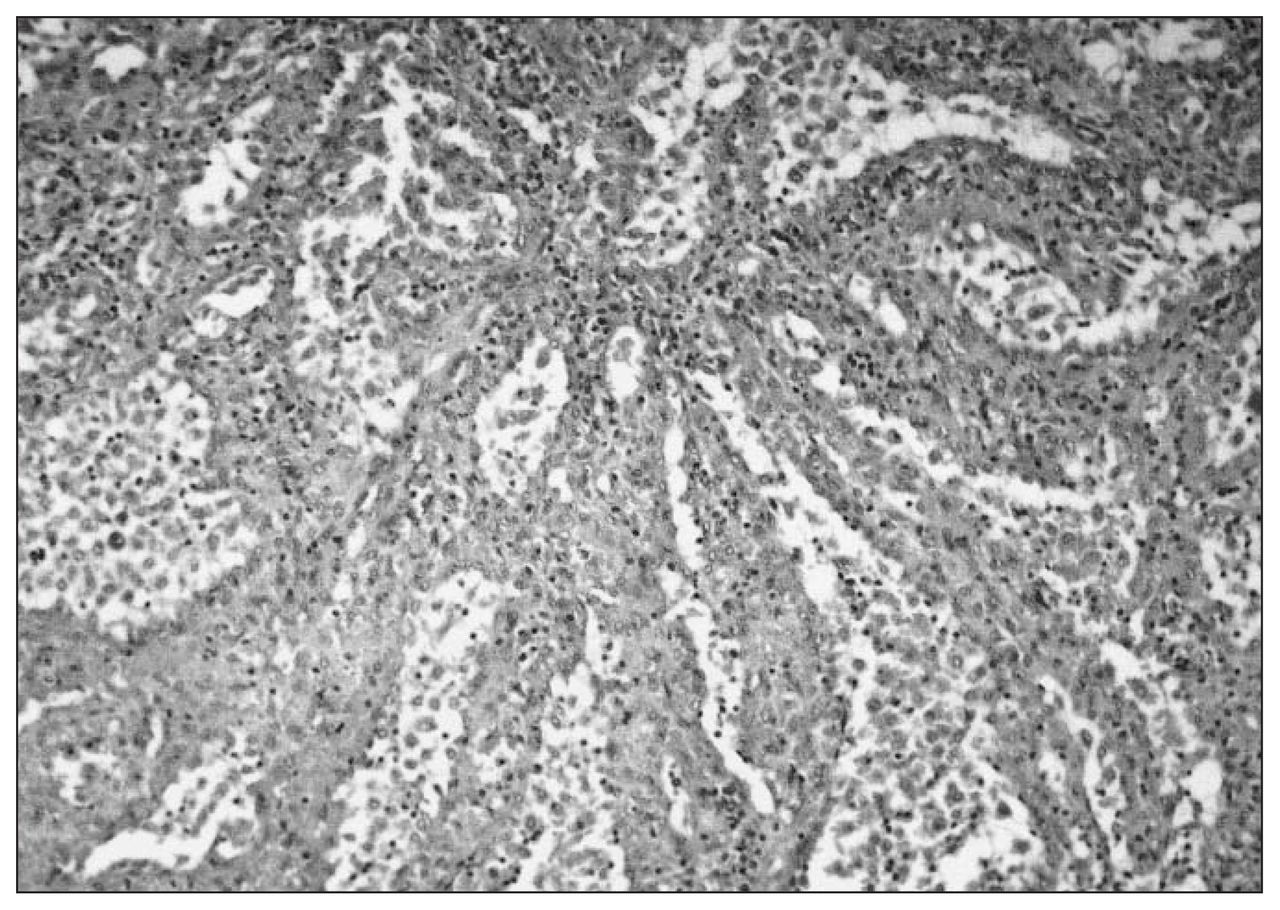
Microscopically, the lesions were composed of a mesh of ectatic anastomosing vascular channels lined by splenic sinus cells (Fig. 3). The cells were positive for both endothelial (Factor VIII, CD31 and CD34) and histiocytic (CD68) markers on immunohistochemical staining. Cytologic atypia and mitotic figures were absent. The diagnosis was littoral cell angioma.
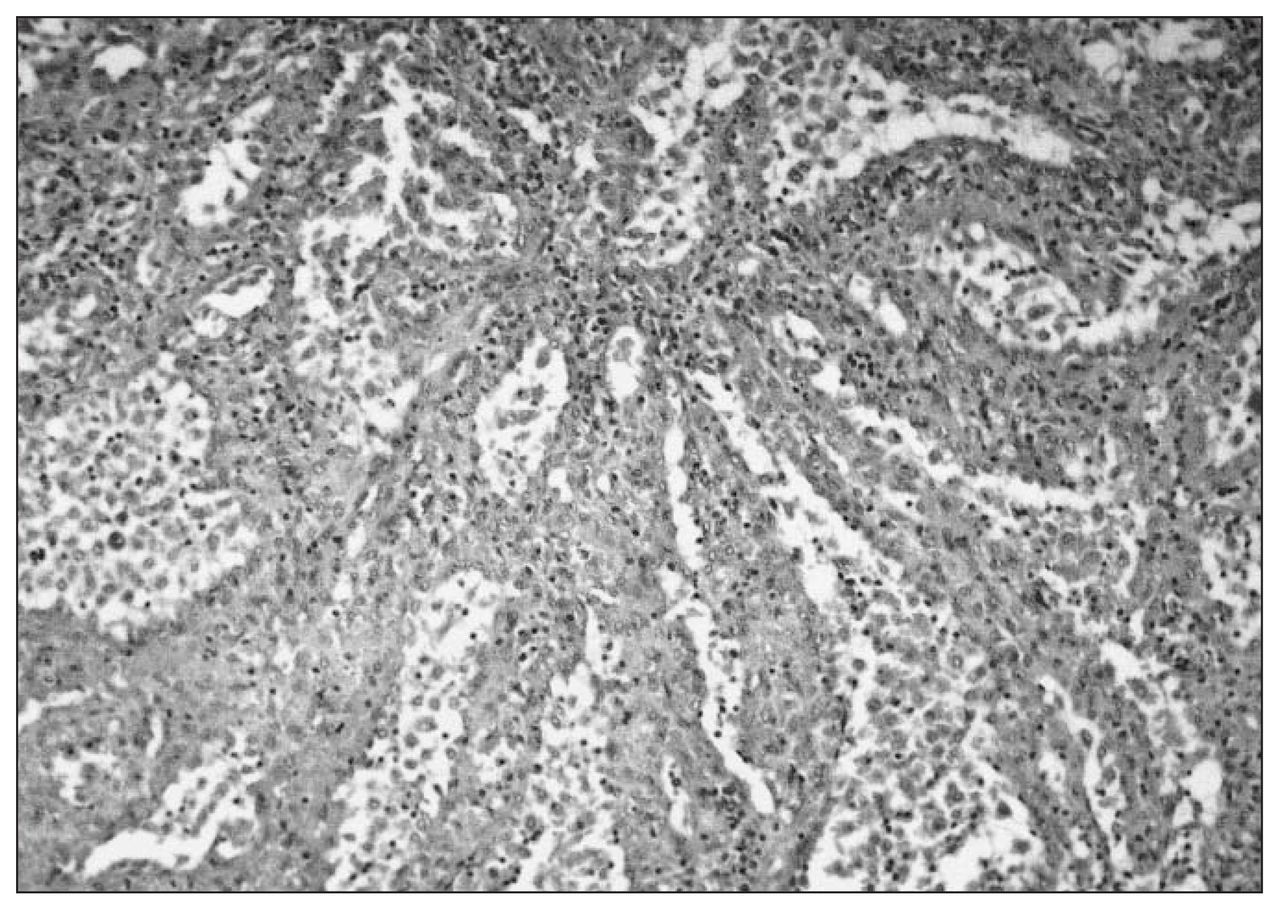
Hematoxylin–eosin stain, original magnification × 200.
Primary splenic tumours are most often benign proliferations of vascular endothelial tissue. Littoral cell angioma is an unusual primary splenic vascular neoplasm first described in 1991.1 It originates from lining cells of the red-pulp sinuses (littoral cells), exhibiting endothelial and histiocytic features.1,2 Although usually found incidentally, littoral cell angioma may present with splenomegaly, thrombocytopenia or anemia.3 Diagnosis is difficult because of the nonspecific nature of clinical, laboratory and radiologic features; splenectomy is necessary to exclude lymphoma and other malignant neoplasms.3 There are no reports of local recurrence or distant metastases with typical benign littoral cell angioma, but a malignant variant (littoral cell angiosarcoma) has been described.4 An association with visceral organ cancers (colorectal, renal, pancreatic) has also been noted.5
Footnotes
Submissions to Surgical Images, soft-tissue section, should be sent to the section editors: Dr. David P. Girvan, Victoria Hospital Corporation, PO Box 5375, Station B, London ON N6A 5A5 or Dr. Nis Schmidt, Department of Surgery, St. Paul’s Hospital, 1081 Burrard St., Vancouver BC V6Z 1Y6.
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.