


Abstract
A potential problem with the standard method of skin closure in pediatric surgery is the development of a skin abscess. To avoid this problem, we introduce a new stitch — the L-stitch. The technique involves passing the suture subcuticularly at the end of the incision and redirecting the needle at a 90° angle from the previous suture, before bringing it out to the skin surface. This stitch can be used in place of the initial and finishing knot of a running suture. It takes less time to perform than a square or a surgeon’s knot and is less bulky. This technique is straightforward and, when used in conjunction with adhesive skin closure strips, provides strong, reliable skin closure, yielding excellent cosmetic results.
Primary closure of surgical incisions in children should satisfy 4 criteria: skin-edge approximation, no need for postoperative suture removal, an excellent cosmetic result and a low incidence of postoperative wound complications.
The standard method of primary skin closure in pediatric surgery is a subcuticular (intradermal) continuous suture of 4-0 or 5-0 synthetic absorbable suture material such as Vicryl (Ethicon, Peterborough, Ont.) or Monocryl (Ethicon).1 This generally provides a strong, reliable closure yielding a good cosmetic result. However, a potential problem with this closure is the development of a stitch abscess at the site of the knot used to complete the suture.2,3 This complication, although minor, may require additional postoperative wound care, can lead to a poor cosmetic result and causes the children and their parents needless anxiety.
We describe a technique by which the surgeon completes the wound closure without a knot and thus avoids this stitch abscess and its attendant problems.
Technique
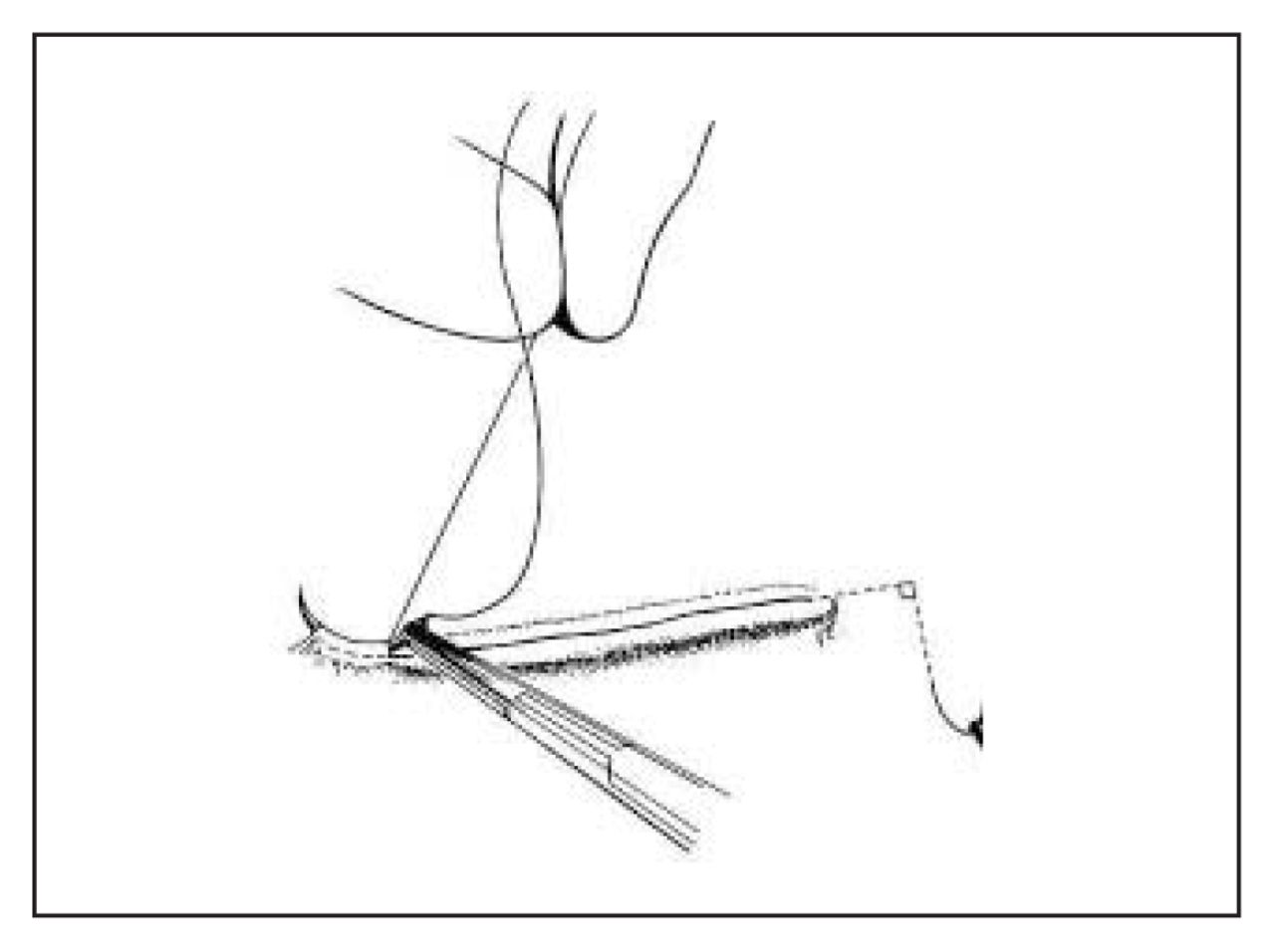
When the end of the wound is reached (Fig. 1), the suture is passed subcuticularly 5–10 mm beyond the wound apex and then brought out to the skin surface (Fig. 2). The needle is then redirected through the previous exit wound and carried 5–10 mm subcuticularly at a 90° angle from the previous suture before being brought out through the skin surface again (Fig. 3). The suture is then cut flush with the skin surface (Fig. 4). This describes the L-stitch as it is used at the distal end of the wound. This technique can also be used, with the steps reversed, to begin the wound closure as shown in Fig. 1.

The wound is closed with the standard subcuticular technique until the end of the wound is reached. Wound closure is initiated by an L-stitch.
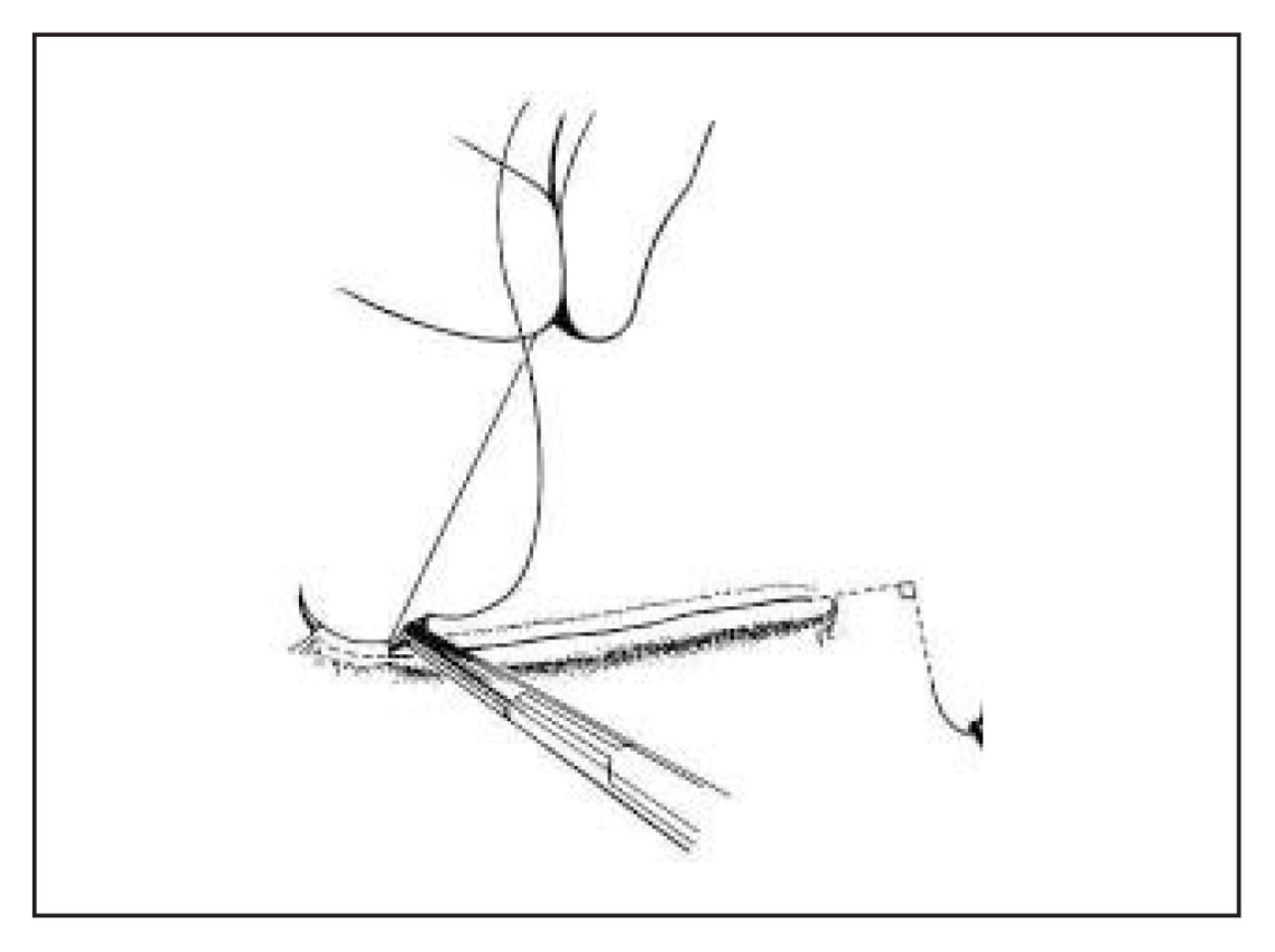
The suture is passed subcuticularly 5–10 mm beyond the end of the wound and is brought out to the skin surface.

The needle is then redirected through the previous exit wound at a 90° angle. It is carried a further 5–10 mm subcuticularly, before being brought out to the skin surface again.

The suture is cut flush with the skin surface.
Wound closure is completed with the application of adhesive skinclosure strips (e.g., Steristrips [3M Health Care, St. Paul, Minn.] that act as a dressing and reinforce the closure).
Comments
We have been using this technique of subcuticular wound closure routinely in our children and have been gratified with the results and the subjectively decreased incidence of stitch abscesses. The friction on the suture created by the 90° subcuticular tract is adequate to keep the skin edges opposed. However, excessive lateral stress on the wound margin must be avoided. By cutting the sutures flush with the skin surface, it leaves no suture exposed. Exposed suture ends can cause anxiety for the child and the parents. This technique is straightforward and, when used in conjunction with Steristrips, provides a strong, reliable skin closure, yielding excellent cosmetic results.
Footnotes
Reprint requests to: Dr. Geoffrey K. Blair, c/o Department of Surgery, 910 West 10th Ave., Vancouver BC V5Z 4E3; fax 604 875-4036
- Accepted September 9, 2002.
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.