


A 69-year-old man with a left inguinal hernia, present for 15 years was seen in the emergency room because the hernia had become much larger in the preceding months. In addition, he had symptoms consistent with an incomplete bowel obstruction. Physical examination revealed a very large irreducible left inguinal hernia that had descended into the scrotum down to the level of the patient’s mid-thigh. It contained bowel, and the sac was moderately tense but without evidence of strangulation. A plain radiograph of the lower abdomen and pelvis (Fig. 1) revealed a long, distended loop of colon in the left scrotal hernia. He was admitted to hospital, and bowel preparation was begun in the expectation that some of the contents of the hernia might need to be resected because of loss of their right of domain in the abdominal cavity. The bowel preparation was only partially effective, however, and produced cramping and distension of the hernia and abdomen.

Plain radiograph of the pelvis, showing a long, distended loop of colon (arrow) in a large left scrotal hernia.
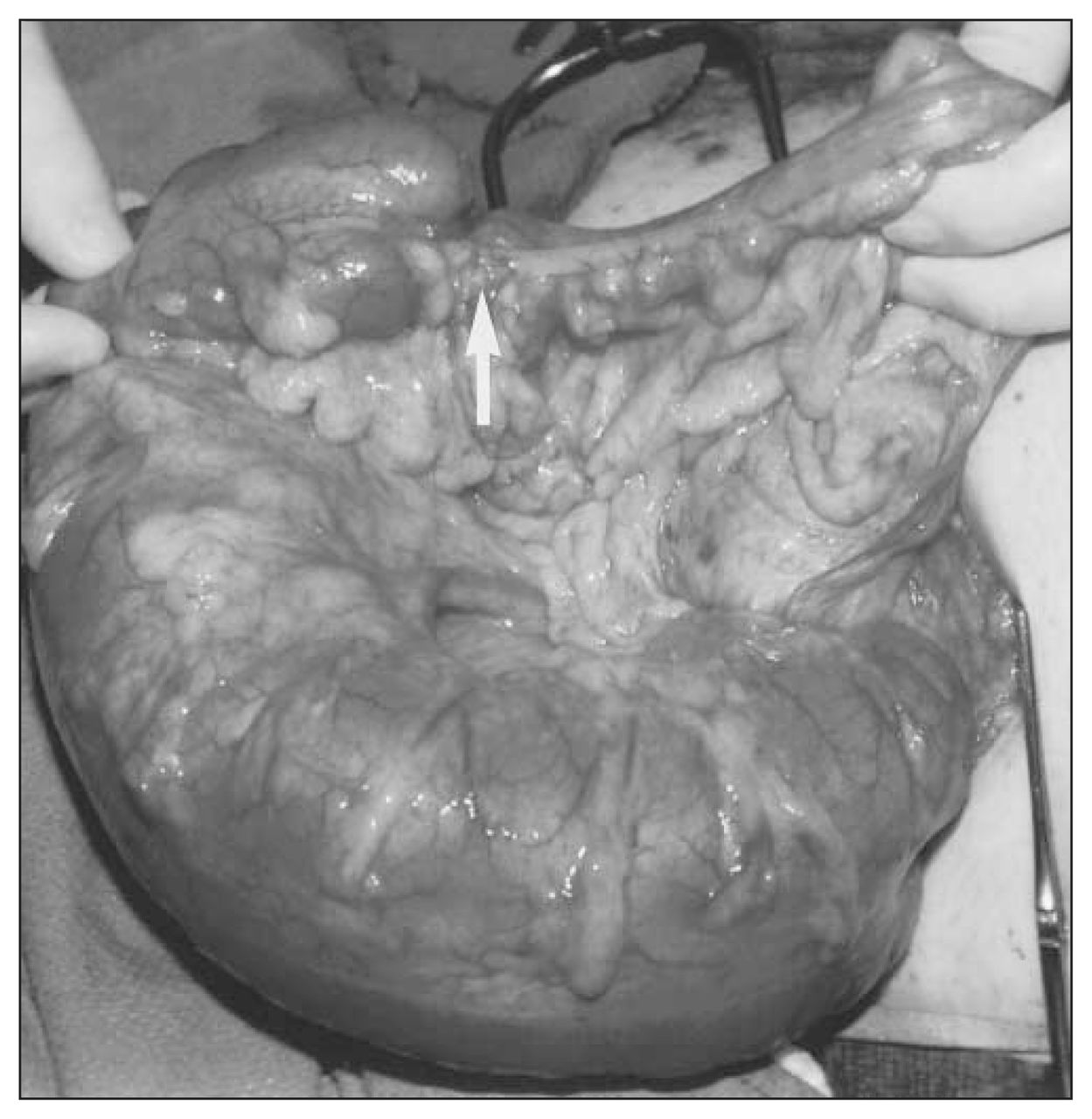
Through a left inguinal incision, a huge hernial sac was delivered from the scrotum. The sac contained an enormously distended segment of colon that was obstructed by a small walnut-sized, stenosing carcinoma (Fig. 2). Beyond it, the colon within the sac was collapsed. The draining lymph nodes were not palpably enlarged. The colon and its mesentery were resected and an end-to-side anastomosis was performed. The Bassini technique was used to close the large direct defect in the posterior inguinal wall. Skin and subcutaneous tissue were left open to heal by secondary intention. Because there was a significant amount of liquid stool in the colon, a defunctioning transverse colostomy was performed. The patient made an uncomplicated recovery, and the colostomy was closed 6 weeks later. The cancer was a moderately differentiated adenocarcinoma that had penetrated through to the serosal surface. None of the 15 resected lymph nodes contained malignant cells.

The opened hernial sac containing a large loop of sigmoid colon obstructed by a small carcinoma (arrow). The patient’s head is to the right.
The enlargement of the patient’s groin hernia was due to dilatation of the colon within the hernia secondary to the obstructing carcinoma that was also within the sac. The possibility of a pathologic condition other than the hernia was the combination of abdominal distension and an increase in the size of the hernia when the bowel was prepared. The hernia itself, although irreducible, was not tight enough to cause obstruction. Its irreducibility was attributable to its chronicity and size.
Colon carcinoma in an inguinal hernial sac has been reported in 19 patients.1,2 Obstruction of the colon was present in only 7 of them. It has been questioned whether patients who present with inguinal hernias should have colon imaging as part of their initial work-up,3,4 because partial colonic obstruction could be a precipitating factor in the development of a groin hernia. A recent casecontrol study compared 614 patients who underwent elective herniorrhaphy of whom 149 had flexible sigmoidoscopy or colonoscopy with 149 control patients who underwent sigmoidoscopy or colonoscopy as part of screening for colon cancer during the same time period.5 There was no increase in the incidence of colon cancer in the hernia group, leading the authors to suggest that screening for colon cancer in patients with groin hernias is not necessary.
Footnotes
Submissions to Surgical Images, soft-tissue section, should be sent to the section editors: Dr. David P. Girvan, Victoria Hospital Corporation, PO Box 5375, Station B, London ON N6A 5A5 or Dr. Nis Schmidt, Department of Surgery, St. Paul’s Hospital, 1081 Burrard St., Vancouver BC V6Z 1Y6.
In this issue

{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.