


Abstract
Introduction: Slipped capital femoral epiphysis (SCFE) is a common hip disorder in adolescents. Treatment can be associated with serious complications, mainly avascular necrosis (AVN). The objective of this study was to evaluate treatment outcomes and complications based on physeal stability at presentation.
Methods: We reviewed retrospectively all children treated for SCFE from 1990 through 2000 at the Children’s Hospital of Eastern Ontario, Ottawa.
Results: Of a total of 87 patients (56 male) identified, 73 had slips classed as stable and 14, unstable; 42 involved the left side, 34 the right, and 19 were bilateral. Avascular necrosis (AVN) developed in 1 patient with a stable slip (morbidity 1.4%) and in 3 with unstable slips (21.4%; p = 0.001). Manipulative anatomical reduction was done in 11 cases (78.5%), all unstable slips. All slips complicated by AVN had been classified according to the traditional system as acute-on-chronic. Complication rates differed significantly between unstable slips (36%) and stable (20%). No statistically significant association was found between AVN and slip severity, time to fixation or use of reduction.
Conclusions: The treatment of stable slips exhibits a lower incidence of AVN. These results nevertheless suggest that gentle reduction of unstable slips is safe and unaccompanied by an increase in complications.
Slipped capital femoral epiphysis is the commonest serious hip disorder in the adolescent. Its traditional classification is according to symptom duration. An acute slip has symptoms that last less than 3 weeks; a chronic slip has a gradual onset and progression of symptoms, which last for longer than 3 weeks. A slip is designated acute-on-chronic when symptoms are chronic for more than 3 weeks with a sudden acute exacerbation lasting less than 3 weeks.1
Loder and colleagues2 emphasized the importance of physeal stability at presentation by correlating it with outcome. A slip is considered to be stable if walking and weight-bearing are still possible, with or without crutches. If walking is impossible even with crutches, the patient has an unstable slip regardless of the duration of symptoms.
The purpose of this retrospective study was to evaluate and compare treatment outcomes of children presenting with a slipped capital femoral epiphysis, stable or unstable, at a major tertiary pediatric trauma centre.
Material and methods
We reviewed the records of all children treated for slipped capital femoral epiphysis in our institution between 1990 and 2000 (inclusive), identifying 87 patients with 106 slips.
Medical records were reviewed for demographic data at the time of the slip, including each child’s age, sex, weight, injured side, history of trauma, weight-bearing status on arrival, duration of symptoms, and length of time from presentation to operation. From initial radiographs, the percentage of slip and slip angle were determined as described by Southwick.3,4 Operative reports were reviewed for the method and number of screws used for fixation, any manipulation attempted, and intra-operative complications.
Range of hip motion, patients’ activity level, and any complaints (pain, limp or stiffness) were recorded from their latest follow-up. Radiographs from the latest follow-up were used to determine the presence of avascular necrosis (AVN) and chondrolysis, which was considered present if there was a joint space narrowing of 3 mm or less.5
For patients with AVN or who underwent reoperation for any reason, we reviewed immediate postoperative and subsequent radiographs, and recorded the time from initial operation to the identification of complications.
Statistical analysis was performed with SPSS software, version 10.0. A 2-tailed Student’s t test was used to quantify significant differences between 2 groups of continuous data. For 2 × 2 analyses when the number in any cell was 5 or less, we used Fisher’s exact test to test differences between groups of discrete data, and the χ2 test when the number in all cells was more than 5.
Results
Based on their ability to bear weight on arrival, 73 (84%) of the 87 patients with slipped capital femoral epiphysis had stable slips and 14, unstable (Table 1).2 Boys (64% of the study group) had 56 slips (7 unstable) and girls, 31 (7 unstable). The right side was involved in 26 slips, and the left in 34; 19 were bilateral.
Comparison of data for patients having stable and unstable slips
Three patients in our evaluation group had an underlying endocrine or genetic disorder: congenital adrenal hyperplasia, histiocytosis and Frohlich’s syndrome, respectively.
Fourteen (16%) of the children presented with distal thigh or knee pain, in isolation or associated with hip and groin pain.6
Stable slips
There were 90 stable slips in 73 patients, of whom 49 (67%) were male (Table 1). Twenty involved the right hip, and 34 the left; 19 were bilateral. The average age at presentation was 12 years (range 5–17 yr); average weight was 73 kg. Eleven patients (15%) had a history of hip trauma before the onset of symptoms on that side. The period from symptom onset to surgical pinning averaged 3 months (range 3 d to 24 mo). According to the traditional classification system,5 70 slips (78%) were chronic, 14 (16%) acute and 4 (4.4%) acute-on-chronic; 2 were pre-slips.
A single screw was used to fix a slipped epiphyses in 58 cases, a pair of screws in 29, and three Knowles pins in 2 cases. One slip occurred in a 5-year-old child with juvenile Scheurmann’s syndrome (Fig. 1). Duration of follow-up averaged 2 years and 9 months (range 2–8 yr).

Radiograph of the hips of a 5-year-old boy with Scheuchmann’s syndrome, illustrating widened physis in the anteroposterior view (upper x-ray) and grade I slips bilaterally on the frog-leg view (lower x-ray).
One patient with a stable slip developed AVN 15 months after fixation (Fig. 2). He had presented at age 14 with groin pain that had been present for 4 months but had worsened over the preceding week. His grade II slip was initially fixed with 2 cannulated screws, which were changed to a single screw in the first postoperative day because of joint penetration by 1 of the screws. The avascular area was limited to the anterolateral area of the femoral epiphysis (Fig. 2).

Radiographs of a 14-year-old boy with a stable slip. The 2 cannulated screws were changed to 1 screw the day after the first operation because of joint penetration. The radiolucent area involves the anterolateral area of the head on both the anteroposterior (left x-ray) and frog-leg lateral (right x-ray) views.
Unstable slips
There were 14 unstable slips in 14 patients; 7 were males. The side affected and other data are presented in Table 1. In 11 cases (79%), acute symptoms occurred as the result of a fall. Seven slips were acute and 7 were acute-on-chronic, according to the older classification system.
Two days was the average period from the onset of acute symptoms to arrival at the hospital (range 1–3 d); average time from presentation to operation was 28 hours (range 3.5– 72 hr). There was a reduction of the slip in 11 hips (79%): 2 spontaneous (14%) and 9 by manipulation (64%). Three were pinned in situ with no reduction. Three of the slipped epiphyses were fixed with 2 Knowles pins, 1 with 2 cannulated screws and 10 with a single cannulated screw.2,7
No child was immobilized in a cast after the operation. The average duration of follow-up was 35 months (range 24–72 mo).
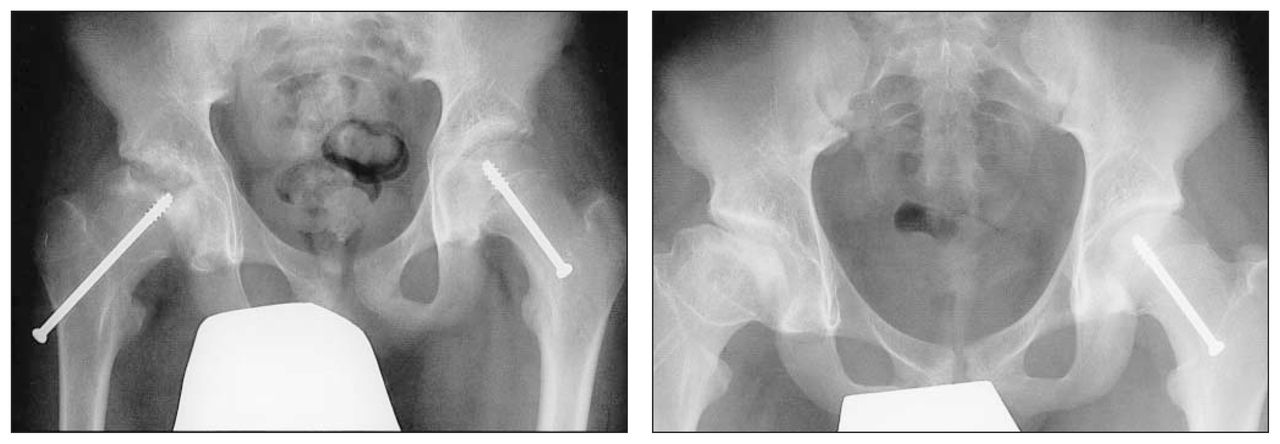
Four of the children, 2 females and 2 males, developed AVN (Fig. 3). Three of those 4 patients underwent gentle reduction intraoperatively with hip flexion, internal rotation and extension, whereas the fourth patient had her slip reduced with the application of skin traction (Table 2).2,5

Left, a radiograph of a child with bilateral slipped capital femoral epiphysis, stable on the child’s left and unstable on the right, who developed AVN. Right, a radiograph taken after removal of the right screw, 2 years later.
Descriptions of the 4 patients who developed postoperative avascular necrosis
Comparison between the stable and the unstable groups
As indicated in Table 1, group differences for patient age, sex and weight were not significant (p > 0.05). The same was true for the side affected by the slip and the duration of follow-up. There was also no significant difference in number of screws used for fixation, or in slip severity (mild, moderate or severe).
Differences between the groups were significant for postoperative flexion, extension and external rotation, with the stable group achieving a better range of motion. Applying the traditional classification to the 2 groups also showed a significant difference between the stable and the unstable groups (p = 0.002): although most slips in the stable group were chronic (70 cases, 78%), none were chronic in the unstable group (50% acute and 50% acuteon-chronic). Four slips in the stable group were acute-on-chronic, 1 of which had AVN (Table 2).
AVN developed in 1 stable slip and 3 unstable slips with a statistically significant difference between the 2 groups (p = 0.001).
An association was found between the traditional classification and the development of AVN (p = 0.001; correlation coefficient –0.352). Whether stable or unstable, all the hips that developed this complication were acute-on-chronic, with an average of 30 hours between presentation in the emergency department and the operation. No significant correlation was found in either group between AVN and the degree of displacement, nor between AVN and surgical delay from either symptom onset or emergency-room presentation (Table 2).1
The average duration of symptoms was 3 months in the stable group and 1.5 months in the unstable group, with no statistical difference between the 2 groups (p = 0.115). The time from the arrival at hospital to the operation averaged 29 hours (3.5–72 h).8,9
Repinning was required for 4 slips, 2 stable and 2 unstable slips. The stable slips that required repinning were due to a joint penetration in 1 case that was later complicated by AVN, and the second repinning was for a patient who had a grade I slip that was fixed with 2 pins, and 3 months postoperatively, radiographs revealed further slippage compared with the immediate post-operative x-ray. The child was not complaining of any pain at that time.10
Two unstable slips required repinning. One patient fixed with a single screw experienced continued slippage. The other, fixed with 2 screws, occurred in a patient with growth hormone deficiency. Despite good initial positioning, follow-up radiographs 10 months postoperatively showed the screws out of the epiphysis because of continued physeal growth.
Chondrolysis developed in 1 unstable slip fixed with 2 screws that had no evidence of joint penetration on the follow-up radiographs or at the time of fixation. The joint space narrowing was evident on x-ray 1 year postoperatively; the patient had symptoms for 1 day and was operated upon within 5 hours after presentation. The patient is now asymptomatic with full range of motion at the most recent follow-up (3 yr postoperative). 5,11
One patient in the stable group was found to have some lucency around the screw 24 months after fixation, for which the screw was removed. 12,13 There was no evidence of infection.
Other complications that we encountered were trochantric bursitis in 1 child, limb length discrepancy of less than 2 cm in 5 (stable slips), and the head of the screw broke at the time of screw removal in 1 child. Of the 87 patients, 36 underwent screw removal.
The overall complication rate was higher in the unstable group (36%) versus stable group (20%) with a statistically significant difference between the 2 groups (p = 0.030).
Discussion
Development of AVN remains a devastating and disconcerting complication. Loder and coauthors2 reported an AVN rate of 47% for unstable slips; in our series, it was much lower (21%). With stable slips, Loder’s group had satisfactory results in 96% of their cases and no AVN, whereas we had 1 case of AVN (1.4%). When slipped capital femoral epiphysis is classified according to physeal stability, the correlation of acute/unstable slips with osteonecrosis was very good.14
Placement of pins in the anterolateral portion of the epiphysis has been reported to increase the risk of AVN,11,15 and our 1 case of AVN was probably pin-induced.
Maeda and colleagues16 and other clinicians8,9 have suggested that in unstable slips the vascular damage occurs at the time of injury, before reduction, and that the reduction does not necessarily contribute to the risk of AVN. We would concur with their view. Indeed, 1 patient in our series with an unstable slip was anatomically reduced in bed with Buck’s traction while awaiting surgery, but nevertheless later developed total head AVN.
Rattey and associates15 also believe that a gentle reduction will not cause AVN and that the previously reported association of AVN with the reduction of the slipped epiphysis may be due to the confounding effect of the severity of the slip, in that a patient who had a severe slip may be more likely to have a reduction.
Although the number of patients in our unstable group was small, no correlation was found between AVN and reduction, timing of the reduction or severity of the slip. All 4 patients who developed AVN in our series (1 with a stable slip and 3 with unstable) were acute-on-chronic in the traditional classification.
It has been reported that AVN develops in unstable slips only.2,17 Our patient with the stable slip who developed AVN had a mild slip that was fixed in situ; he had had hip pain for 4 months that was exacerbated by a minor fall 1 week before presentation. We changed this patient’s fixation to a single screw the day after his operation because of joint penetration; the avascular area was localized to the antrolateral area of the epiphysis, and AVN was probably secondary to a pinning complication.
The transient penetration of the joint in that patient was unassociated with chondrolysis.18 In 4 other patients, transient penetration of the joint was noted and corrected during the procedure, with none exhibiting any symptoms or signs of chondrolysis. Our 1 case of chondrolysis did not have pin penetration and within 1 year recovered complete range of motion.
Slip progression secondary to continued physeal growth resulted in the epiphysis growing off the pins in 3 patients (1 in the stable and 2 in the unstable group). Their slip progression required repinning.10
The youngest patient in our group (5 years old) had bilateral slips; the right side was pinned and the left, closely observed. Both joints had favourable outcomes.
This retrospective study of 114 slipped capital femoral epiphyses showed no association between the severity of the slip, the time to operation and the development of AVN. The case of avascular necrosis in the stable slip could have been related to the operative fixation. Gentle manipulative reduction appears to be a safe procedure that does not contribute to the development of AVN.
Acknowledgement
The authors are very appreciative of the secretarial support of Ms. Sue Ziebel in the typing of the drafts of this paper.
- Accepted December 15, 2003.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.