


A 71-year-old woman with new onset end-stage renal failure of unknown origin presented with symptoms of uremia (nausea, vomiting, purities, dyspnea, fatigue). Physical examination revealed an area of dry gangrene on the left leg. Laboratory investigations demonstrated a urea of 47.6 mmol/L, creatinine level of 884 μmol/L, hemoglobin of 60 g/L, calcium of 3.5 mmol/L, a phosphate level of 2.15 mmol/L, a calcium phosphorus product of 93 ([Ca] × [PO3] in conventional units) and a parathyroid hormone of 1138 pg/mL. The patient was placed on hemodialysis. The gangrenous lesion was presumed to be related to the patient’s venous insufficiency.
Over the next 2 months, there was progression of the dry gangrene involving the anterior and posterior aspect of both upper legs, the posterior and lateral aspect of the lower legs, the lower back and the buttocks (Fig. 1). A thromboembolic etiology was considered, and the patient was placed on heparin. A skin biopsy of the lesion showed no evidence of emboli, and an echocardiogram failed to reveal a source.

Photograph taken at operating room showing the extent of the necrotic skin lesions.
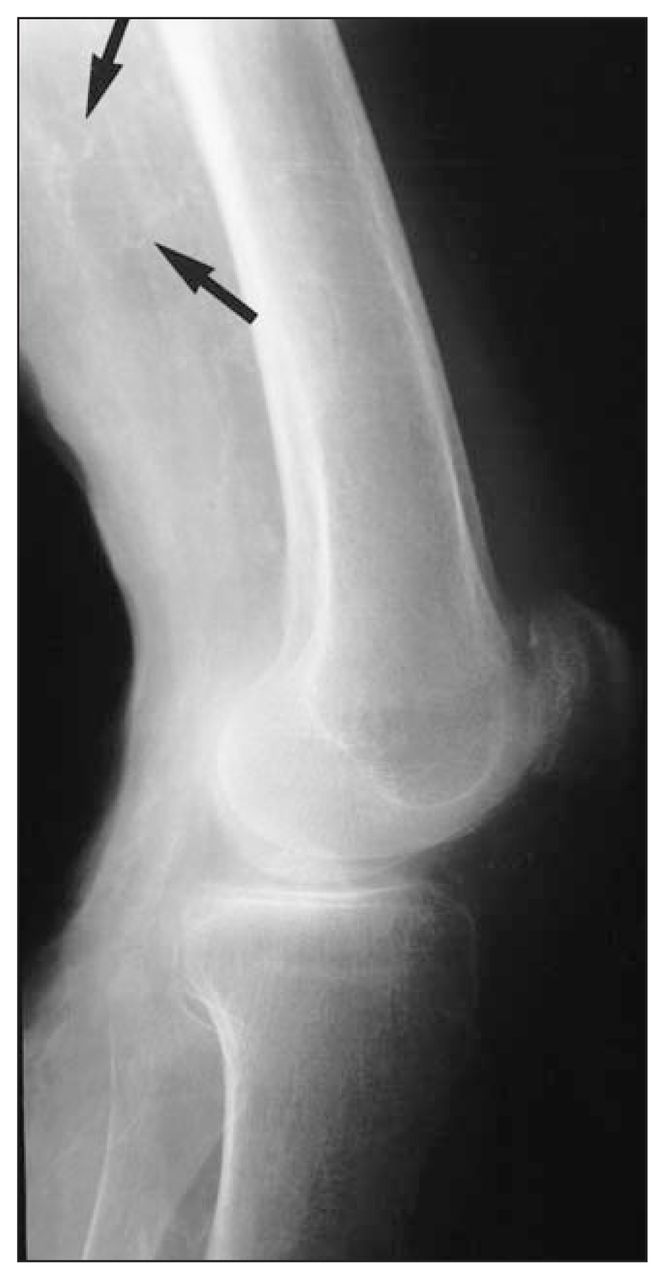
The patient was referred to our centre, where a bilateral leg x-ray revealed calcification of the small arteries of both legs (Fig. 2). A second skin biopsy established the diagnosis of calcinosis cutis (Fig. 3) due to hyperparathyroidism. An urgent parathyroidectomy was performed. At parathyroidectomy, a large, fixed, right superior parathyroid gland and a normal looking right inferior gland were visualized and removed.
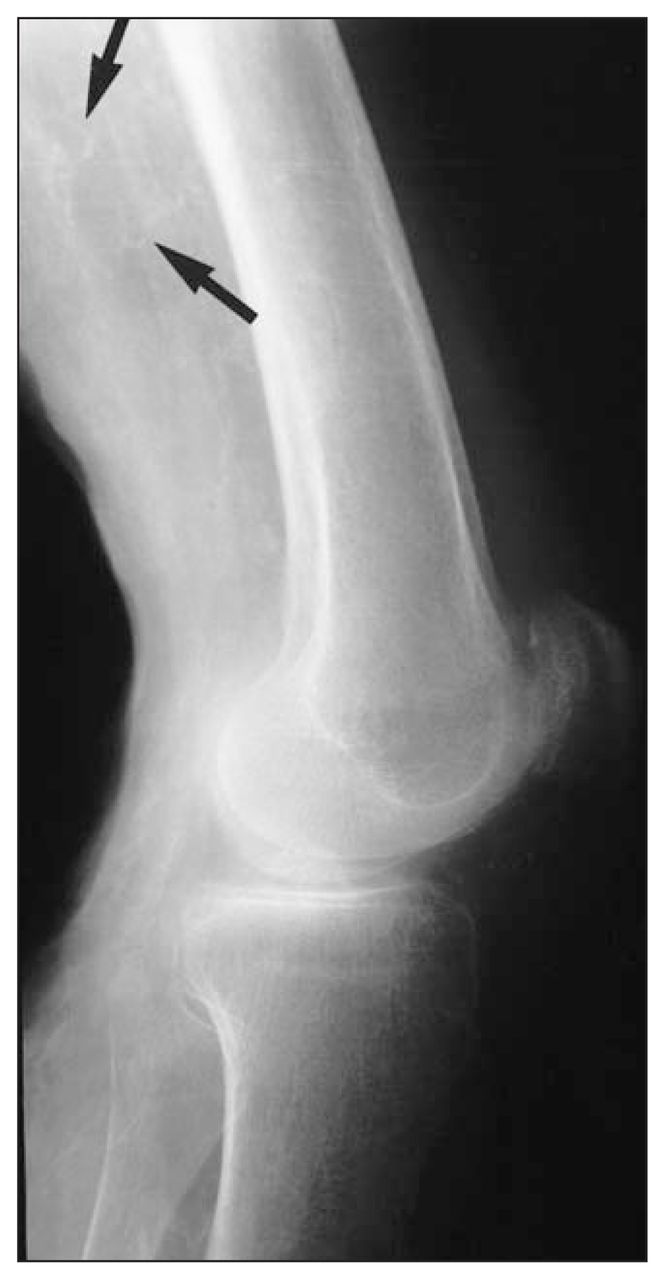
Radiograph of the left leg. The arrow shows calcified small blood vessels.
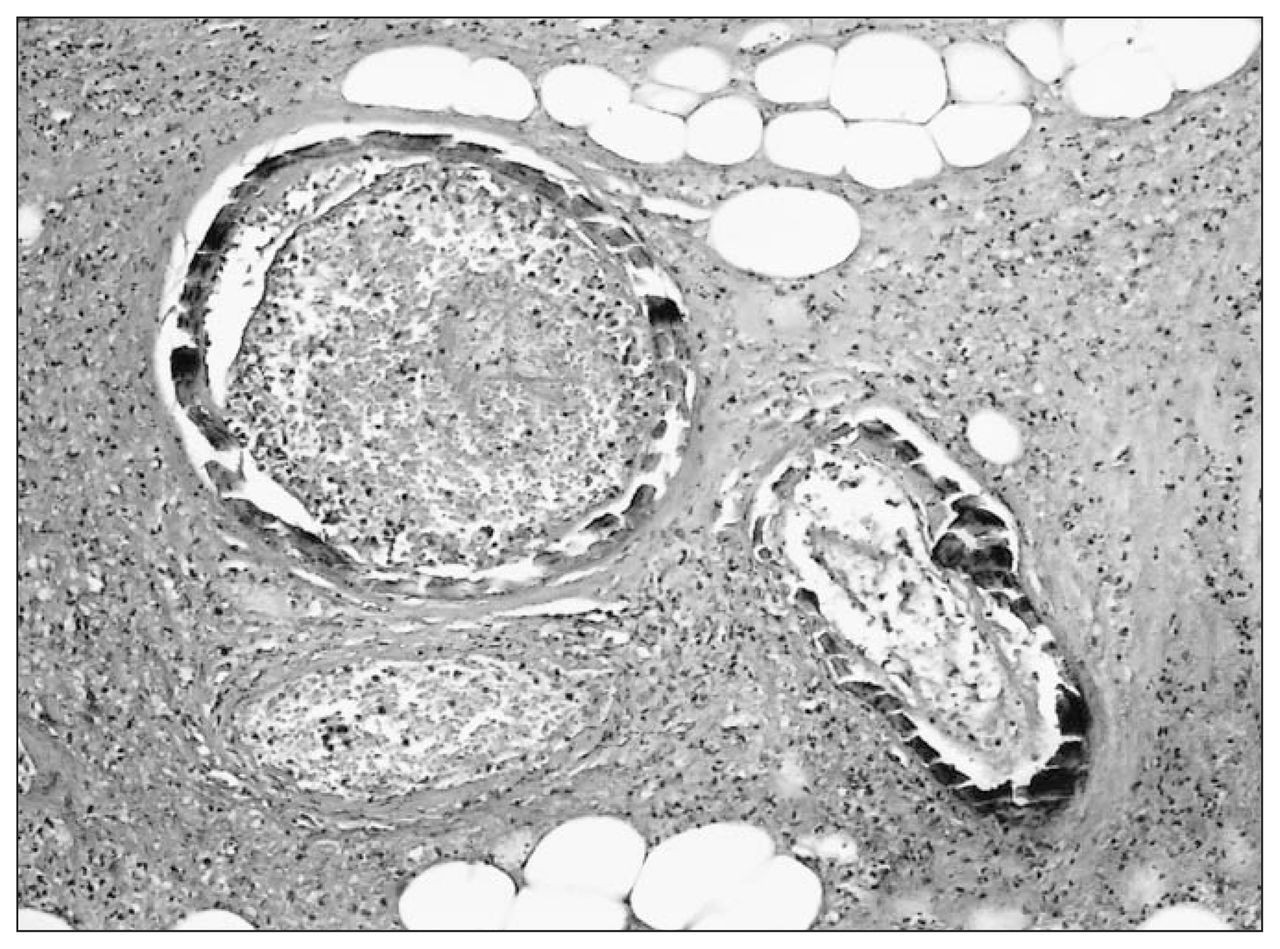
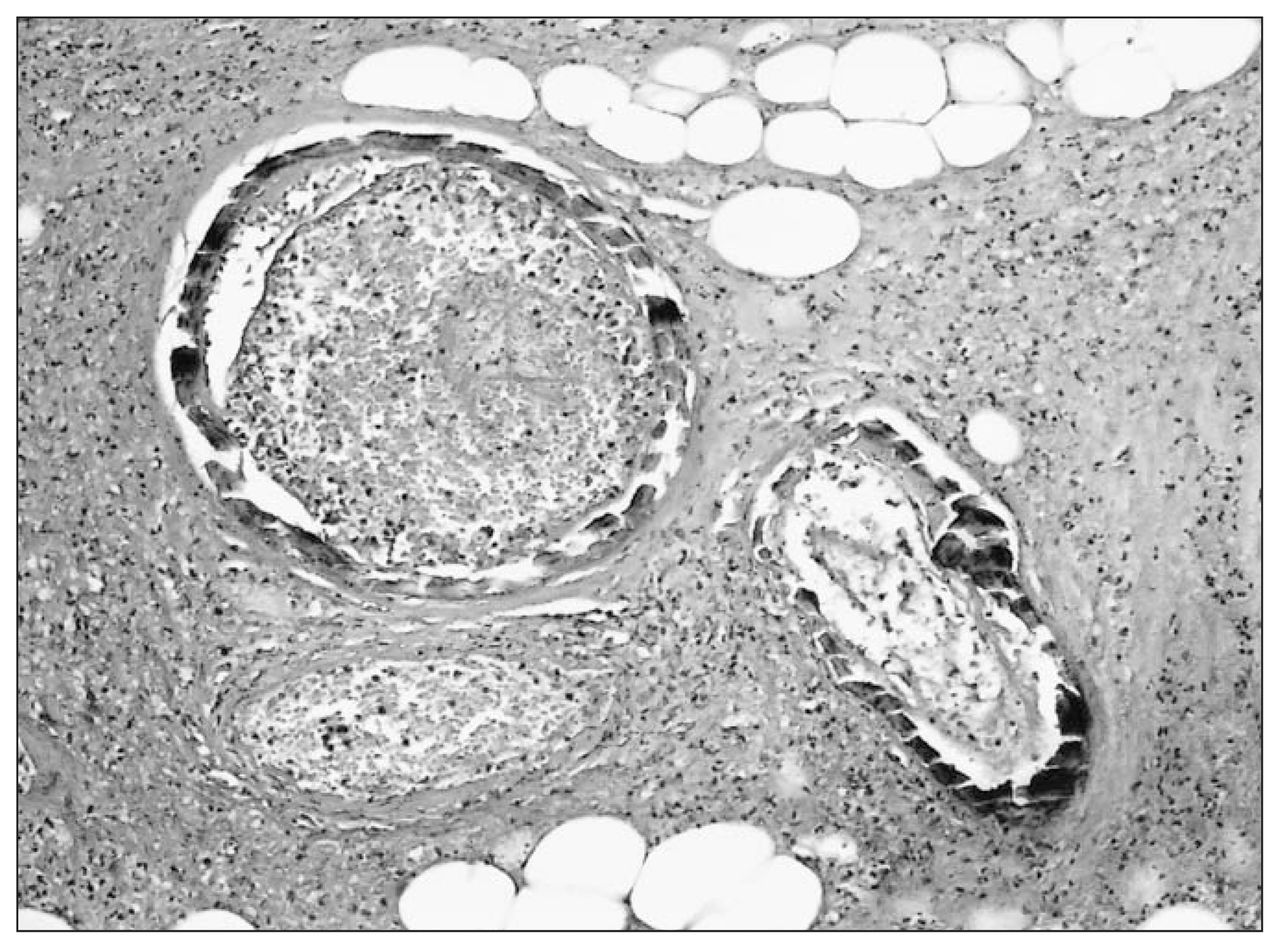
100 × (hematoxylin and eosin) micrograph of cutaneous arteries showing extensive mural calcification, luminal thrombosis and necrosis of surrounding tissue.
On gross examination, the right superior specimen weighed 3.96 g, with the gland measuring from 2.7 × 2.1 × 1.5 cm in size (Fig. 4). The inferior parathyroid gland measured 1 × 0.65 × 0.4 cm and weighed 0.073 g. Microscopic examination of the right superior gland demonstrated hypercellularity and calcification. Gross and microscopic findings were consistent with parathyroid adenoma.
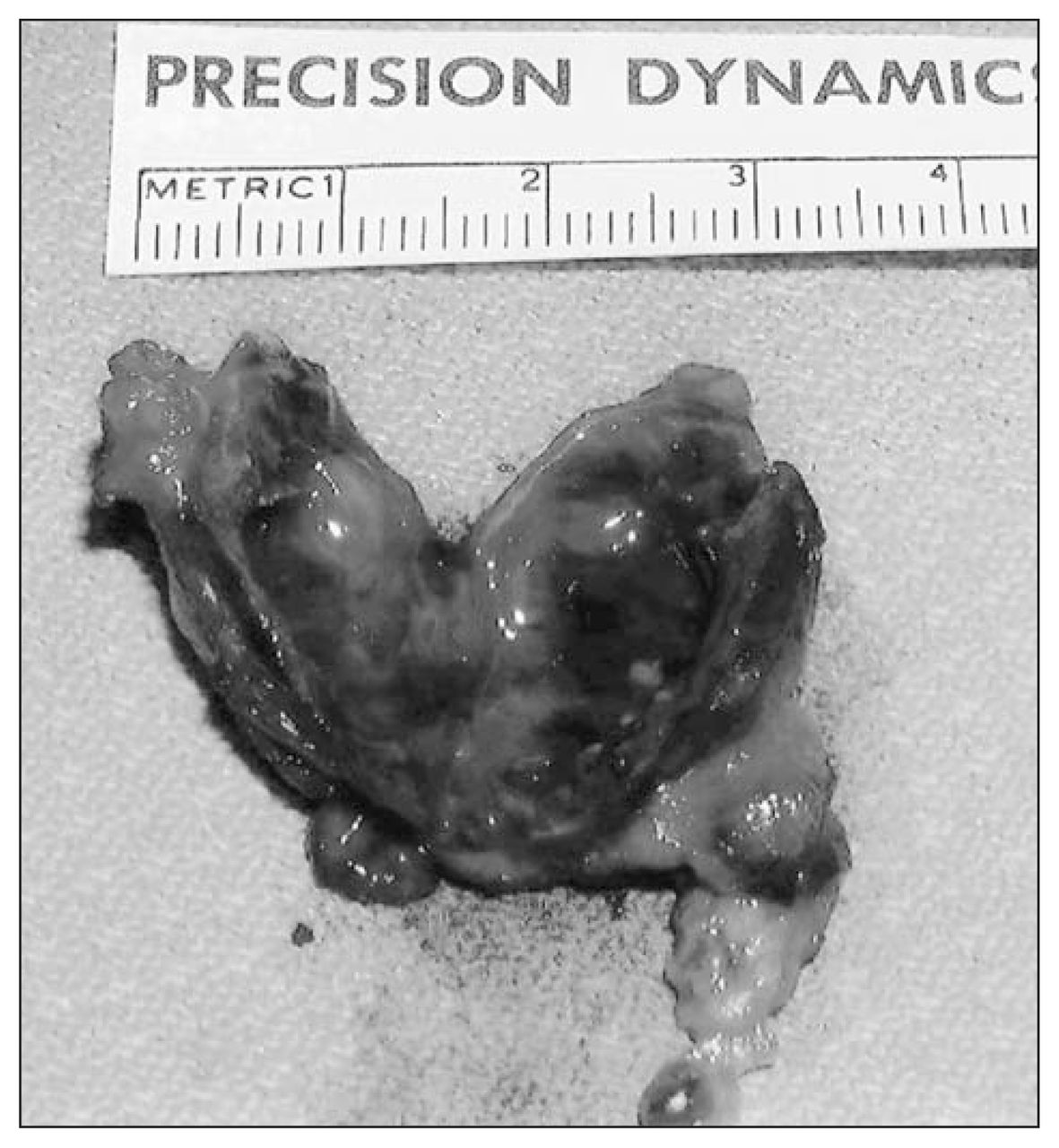
Right superior parathyroid adenoma (3.96 g).
The patient’s condition deteriorated postoperatively; she developed pneumonia and bilateral pleural effusions and became hypotensive. Due to the extent of the necrotic tissue in her legs, the need for surgical débridement and amputation, and her concomitant medical problems, the family decided to withdraw care. The patient died of overwhelming sepsis.
Calcinosis cutis (also known as calciphylaxis), the progressive deposition of calcium in the skin and small blood vessels with associated thrombosis and necrosis, is a rare and life-threatening illness. It most commonly results from hyperparathyroidism secondary to renal failure and most commonly occurs in women.1 Calcinosis cutis typically presents with ulcerating painful purplish lesions in the extremities and trunk. These lesions often progress to necrosis and act as a portal for infectious agents leading to wound sepsis and death.2 The etiology of this disease remains unclear, however, and elevated calcium phosphorous product ([Ca] × [PO3] > 70 in conventional units) is thought to act as a sensitizer, promoting calcification. Elevated levels of parathyroid hormone have also been implicated as a sensitizer.1 Treatment is difficult, with such medical therapies as phosphate binders and steroids having little effect.3 The best current therapy is systemic antibiotic drugs, débridement of necrotic tissue and semi-urgent parathyroidectomy.1–4 Early parathyroidectomy has been shown to significantly reduce mortality in a study of 104 patients with calcinosis cutis and renal failure.4 Despite these results, the literature would agree that the current therapy remains unsatisfactory. 1–3 Calcinosis cutis can be difficult to diagnose on pathology; thus, if the clinical suspicion of calcinosis remains high after a negative skin biopsy, it is wise to repeat it.
Footnotes
Submissions to the Surgical Images, soft-tissue section, should be sent to the section editors: Dr. David P. Girvan, Victoria Hospital Corporation, PO Box 5375, Station B, London ON N6A 5A5 or Dr. Nis Schmidt, Department of Surgery, St. Paul’s Hospital, 1081 Burrard St., Vancouver BC V6Z 1Y6.
Competing interests: None declared.
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.