


Acute abdominal wall herniations following blunt abdominal trauma are rare despite the high prevalence of blunt trauma.1,2 In multitrauma patients, diagnosing a traumatic hernia can be challenging. We report the case of a 67-year-old woman who sustained a medial detachment of the diaphragm from the anterior portion of the abdominal wall with presternal space herniation (of her stomach and transverse colon) as a result of a motor vehicle collision.
Case report
A 67-year-old obese woman was a restrained driver of a vehicle that was struck on the driver’s side by a train. She initially presented to a remote community hospital where mechanical ventilation was started and she had bilateral chest tubes placed for hemopneumothoraces. She was subsequently transported by helicopter to Foothills Medical Centre (Calgary, Alta.). She had sustained multiple injuries, including multiple bilateral rib fractures, bilateral hemopneumothoraces, pulmonary and cardiac contusions, closed head injury, small splenic laceration and a right humerus fracture.
The initial computed tomography (CT) scan revealed substantial disruption of the anterior chest wall with disruption of the costochondral interfaces and open communication between bilateral pleural spaces and the soft tissues of the anterior chest (Fig. 1). There was no evidence to suggest herniation through the abdominal wall, clinically or radiographically. About 72 hours after admission, she underwent a repeat CT scan so we could further evaluate her splenic injury for pseudoaneurysm formation (Fig. 1). This scan revealed a flail rib cage involving the parasternal aspect of the right hemithorax and subxiphoid area with herniation of transverse colon, mesocolon, omentum and gastric antrum into the anterior presternal space, without evidence of wall thickening, obstruction or strangulation of the herniated structures. We determined that the patient should undergo surgery for repair of her traumatic hernia.
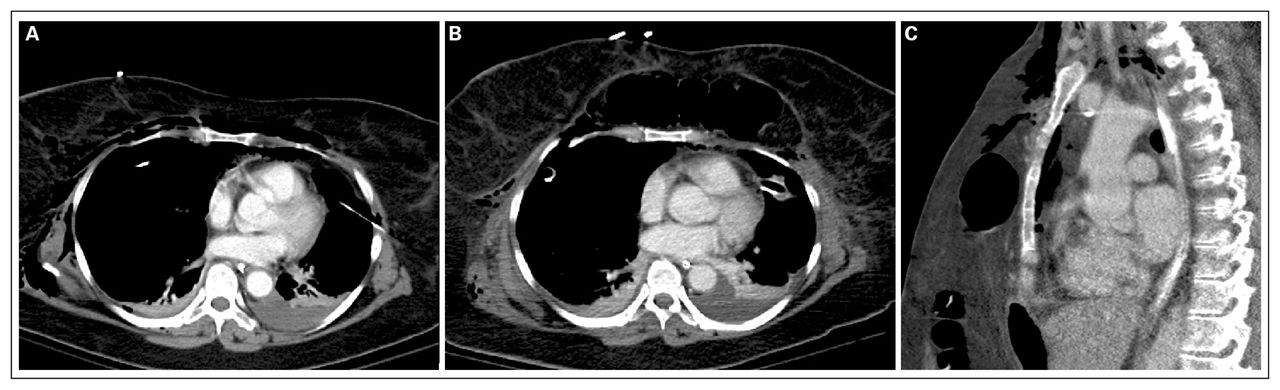
Thoracic computed tomography (CT) scans. (A) The initial scan, at the time of admission, shows right anterolateral tracking of subcutaneous air. (B) A scan taken 72 hours later demonstrates herniation of large bowel into the anterior presternal space. (C) A sagittal-view scan (taken at the same time that shown in panel B) demonstrates disruption of the abdominal wall: flail rib cage involving the parasternal aspect of the right hemithorax and subxiphoid herniation of a loop of transverse colon, mesocolon, omentum and the gastric antrum into the anterior thorax.
A midline laparotomy revealed bilateral disruption and avulsion of the superior insertions of the rectus abdominus muscles from the xiphisternum and medial costal margins in conjunction with bony fractures of the costal margin itself. Further dissection revealed herniation of abdominal contents through the disrupted area and into an extensive subcutaneous space anterior to the sternum and costal margins but posterior to the pectoralis muscle.
The herniation was due to medial detachment of the diaphragm from the anterior portion of the abdominal wall caused by traumatic rib fractures extending from the left costochondral margin to the middle portion of the ribs. Both hemidiaphragms were intact, with no communication to the thoracic cavity.
We performed a primary repair of the thoracic wall and reattached the anterior diaphragm over the costal margin (Fig. 2). We reapproximated the anterior abdominal wall to the lateral thoracic wall. A medial defect remained, which we filled using a composite GORE-TEX mesh sewn to the costal margin and anterior abdominal wall fascia.

An intraoperative photograph shows the repair of the thoracic wall, reattachement of the anterior diaphragm to the costal margin and the medial defect filled with composite mesh.
Discussion
Acute abdominal wall herniation and diaphragmatic ruptures are rare yet well described complications of blunt abdominal trauma. They are most commonly associated with motor vehicle collisions and with the use of seatbelts.1 The incidence of traumatic abdominal wall herniation is estimated at less than 1%3 and diaphragmatic rupture between 0.8% and 1.6%.2 Efforts to classify traumatic hernias have focused on low-versus high-energy types, type of muscle defect, size of defect and severity of injury and location. Low-energy hernias result from the impact of a small object such as a bicycle handlebar, whereas high-energy injuries typically are sustained during motor vehicle or vehicle versus pedestrian collisions.
Most traumatic herniations occur at the inferior (Petit) lumbar triangles, where seat belts typically transmit the force of an abrupt deceleration, and the superior (Grynfeltt–Lesshaft) area; anterior wall hernias are much less common.1 These injuries are most commonly seen following high-velocity motor vehicle collisions, pedestrian strikes, falls and handlebar injuries.4 Given these mechanisms of injury, traumatic abdominal wall herniation or diaphragmatic rupture are typically associated with other intra-abdominal injuries and necessitate a thorough workup.5 Computed tomography has become an important adjunct in the characterization of traumatic injuries and is useful in distinguishing rectus sheath hematomas from true herniation.
With traumatic hernias, rates of incarceration approach 25% and strangulation about 10%.4 Early surgical repair is necessary to avoid such complications and to identify other associated intra-abdominal injuries. Management should be individualized to include primary closure or repair with mesh if the defect is too large for primary closure.
Conclusion
In conclusion, abdominal wall herniation and diaphragmatic ruptures are rare complications of blunt abdominal trauma. Our patient’s case illustrates how a traumatic chest injury can result in detachment of the diaphragm from the anterior portion of the abdominal wall at the costal margin resulting in herniation of viscera into the anterior presternal space.
Footnotes
Competing interests: None declared.
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.