


Abstract
Background: Studies have shown that women present for surgery at an older age and with greater dysfunction than do men; however, the explanation for this finding is unclear. We investigated the impact living status (alone or with another person) and sex the on timing and outcomes of hip and knee replacement surgery.
Methods: We surveyed 1722 patients undergoing primary hip or knee replacement surgery. Relevant covariates including demographic data, body mass index, sex, living status and comorbidities were recorded. We assessed joint pain and functional status before surgery and at 3 months and 1 year after surgery using the Western Ontario McMaster University Osteoarthritis Index (WOMAC) scores for pain and function.
Results: In total, 22.9% (395) of all patients (29.3% of women and 14.1% of men) were living alone at the time of surgery. Compared with patients who lived with another person, those who lived alone were significantly older, had greater comorbidity and reported greater joint pain and dysfunction before surgery and 3 months and 1 year after surgery. Living alone and female sex independently predicted a greater preoperative WOMAC score, and living alone predicted an older age at the time of surgery and a poorer 1-year outcome.
Conclusion: Patients who live alone may delay joint replacement surgery until an older age and have greater joint pain and dysfunction than those who live with another person, leading to poorer 1-year outcomes.
Statistics Canada and the United States census both reported in 2006 that 26% of all homes were single-person households.1,2 A greater number of women than men live alone.1,2 In 2001 in Canada, over 1.5 million women (14% of the total female population aged 15 and older) were living alone, which was more than double the percentage from 1971. In the United States in 2000, 14.8% of all women lived alone, compared with 10.7% of men.2 Among people aged 65 years and older, 38% of all women live alone, compared with 16% of men.3 This is also the age group most likely to undergo hip or knee replacement surgery.4–7
Having greater social support at the time of surgery has been shown to contribute to improved clinical outcomes.8–11 Greenfield and colleagues12 suggested that being married, compared with not being married, at the time of surgery may improve outcomes after hip replacement.
Many studies have shown that women present for surgery at an older age and with greater dysfunction than do men; however, the explanation for this finding is unclear.13–15 Whether living status influences age at the time of elective surgery is not well understood. One group conducted focus group interviews with patients before joint replacement surgery and found that, compared with men, women who were living alone were fearful of having no one to care for them after surgery and they were less likely than men to choose surgery earlier in the course of their disease.16 Senior arthroplasty surgeons in our centre have observed that women delay surgery because of the fear of living alone.
We investigated whether living alone and sex affects age at the time of elective joint replacement surgery and whether living alone affects function after surgery. We hypothesized a priori that patients who lived alone would delay surgery until a later age and would have a greater level of dysfunction than those who lived with another person and that this effect would be most pronounced among women.
Methods
Study sample
We recruited patients on a waiting list for surgery from a hip and knee replacement registry at the Toronto Western Hospital. All patients gave informed consent for inclusion in the database. We included patients aged 18 and older with a diagnosis of primary or secondary osteoarthritis. We reviewed data from consecutive patients between 2001 and 2005.
Data collection
An independent assessor not involved in the medical care of the patients collected all data. Baseline demographic characteristics (age, sex, body mass index [BMI] and living status) were collected by patient self-report. Living status was a dichotomous variable of either living alone or living with another person. Baseline medical health was scored using the Charlson Comorbidity Illness Index.17 Given the low incidence of comorbidity in this sample, we grouped the scores into 4 categories (0, 1, 2 or ≥ 3).
We assessed functional status and pain level before surgery and 3 months and 1 year after surgery by use of the Western Ontario McMaster University Osteoarthritis Index 1 (WOMAC) scores for function and pain.18 A greater score on the WOMAC scale represents poorer function or greater pain. The reliability, validity and responsiveness of the WOMAC score has been established in an osteoarthritis population.18 We assessed quality of life by use of the Medical Outcomes Study 36-Item Short Form (SF-36).19–21
Statistical analysis
We performed univariate analyses of hip and knee replacement data separately. Both groups demonstrated a similar pattern of functional improvement whether they lived alone or with someone. Because we found the same significant differences for WOMAC scores both before and after surgery between those living with someone or alone, we present the combined analyses for hip and knee replacement patients.
We compared continuous data such as age, BMI and WOMAC pain and function scores between groups using t tests because the data were normally distributed. Means and standard deviations are reported for all continuous variables. Categorical data such as sex, living status and Charlson Index are reported with frequencies and groups and were compared by use of the Fischer exact test.
We used multivariable linear regression modelling to determine the impact of living status and sex on age at the time of surgery and on preoperative WOMAC scores. We created further models to determine the impact of living status and sex on patient outcomes after surgery by analyzing the 3-month and 1-year WOMAC scores as the dependent variables. We entered into the model the covariates age, BMI, Charlson Index, preoperative WOMAC score, mental component score and joint affected (hip v. knee). The mental component score variable was not statistically significant and was excluded from the final model presented.
We performed all statistical analyses with SPSS (version 13.0). Parameter estimates for regression modelling and their 95% confidence intervals are reported. All reported p values are 2 tailed with an α of 0.05.
Results
In our registry, we had complete data for 1722 of the 2390 (72.0%) patients who made up our study cohort. Responders were not significantly different from nonresponders in terms of age, BMI, sex or Charlson Index (data not shown).
At the time of surgery, 329 of 1722 (22.9%) patients lived alone. Of the men, 102 of 722 (14.1%) lived alone, compared with 293 of 1000 (29.3%) women (p < 0.001). Compared with patients who lived with someone, patients who lived alone were significantly older, had more medical comorbidities and reported greater pain and dysfunction on all sections of the WOMAC scale at baseline and at 3 months and 1 year after surgery (p < 0.05) There was no difference in baseline mental component score between the groups (p > 0.05, Table 1). Figure 1 shows the standardized WOMAC scores at baseline and at 3 months and 1 year after surgery. Living alone and being female independently predicted a greater preoperative WOMAC score at the time of surgery after adjustment for age, BMI and Charlson index (Table 2).
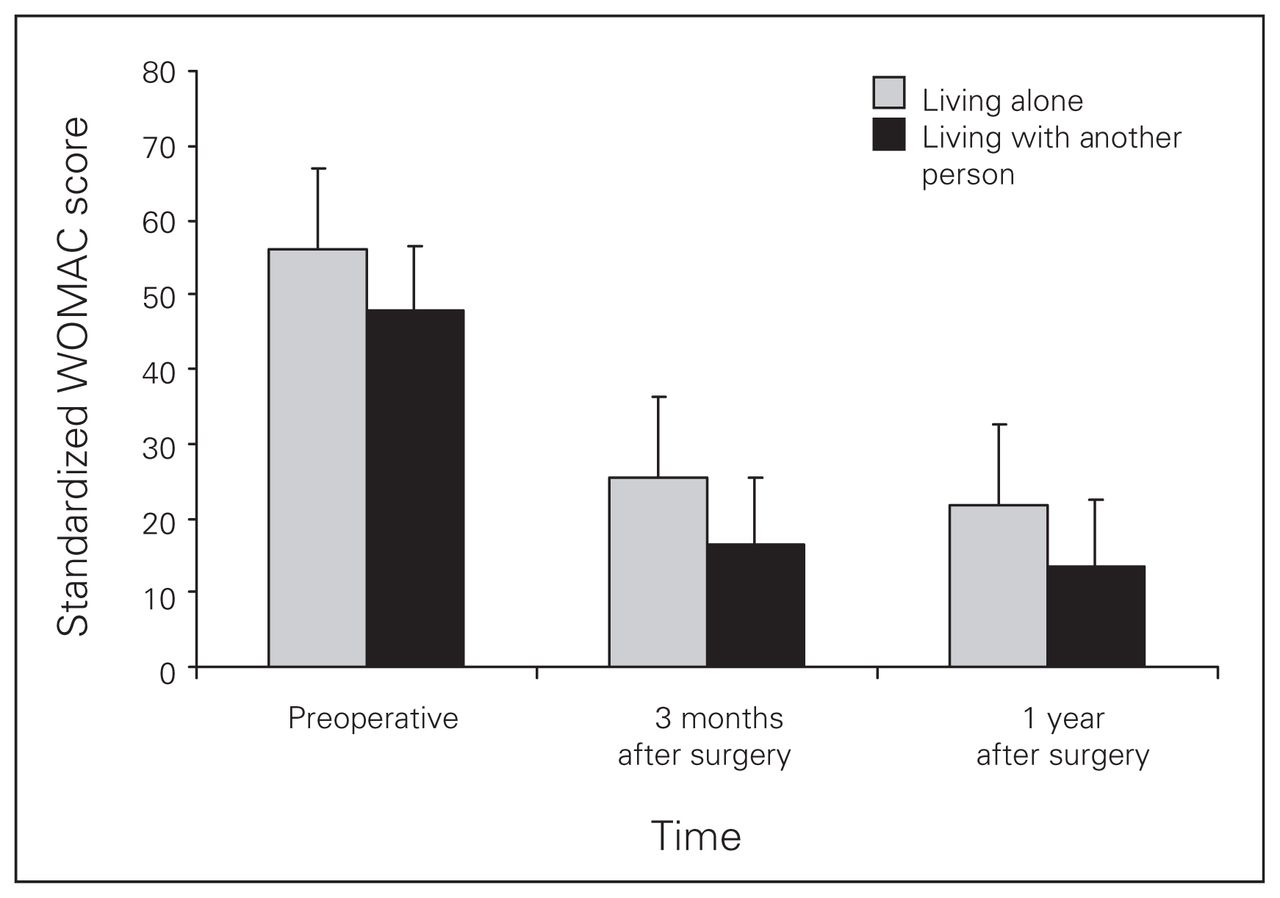
Total scores on the Western Ontario McMaster University Osteoarthritis Index (WOMAC) at baseline and 3 months and 1 year after surgery for patients who lived alone and those who lived with someone. The WOMAC scores were standardized to female sex, age 50 years, body mass index 30 kg/m2 and Charlson Index score of 1.
Unadjusted analysis of the demographic characteristics and outcome data for patients who lived with another person and those who lived alone
Linear regression model predicting preoperative scores on the Western Ontario McMaster University Osteoarthritis Index
Living alone also predicted an older age at the time of surgery, independent of sex, BMI, Charlson Index and baseline WOMAC score (p < 0.001, Table 3).
Linear regression model predicting age at the time of surgery
Living status also impacted the degree of recovery after surgery, independent of baseline WOMAC score. Patients who lived alone had significantly greater WOMAC scores at 3 months (p = 0.04) and 1 year (p < 0.001) after surgery, independent of age, sex, BMI, Charlson Index, affected joint and baseline WOMAC score (Table 4). Sex was an independent predictor of a greater WOMAC score at 3 months (p = 0.03) but not 1 year (p = 0.81, Table 4) after surgery.
Linear regression model predicting scores on the Western Ontario McMaster University Osteoarthritis Index 3 months and 1 year after surgery
Discussion
We found that women and people who lived alone had greater WOMAC scores at the time of surgery and that patients who lived alone presented for surgery at an older age. Furthermore, we found that patients who lived alone received less relative benefit from joint replacement after 1 year than did patients who lived with another person.
Over the last 5 years, the number of single-person households in the United States and Canada has increased by about 10%, and more women than men live alone.1,2 Part of the explanation for this change in living status is the rising incidence of divorce and the drop in marriage rates. In 2006, the Canadian Census reported that 51.5% of all people over the age of 15 were unmarried, compared with 20 years ago when only 40% were unmarried.22 The same trend was seen in the US census, which showed that the divorce rate has increased by 10 times over the last century.23 One factor that may contribute to why more women than men live alone is the difference in life expectancy between men and women. In 1920, women had a life expectancy that was 3.4% longer than that for men; in 2006, this difference was 6.4%.24 The number of hip and knee replacements performed in Canada and the United States is growing rapidly. Our findings are, therefore, particularly relevant because they affect a very large and growing segment of the population; this is a demographic that requires extensive medical support.4–7
Our finding that women appear to delay surgical care of arthritis agrees with the findings in other areas of medicine. For example, Schmidt and Borsch25 showed that female sex was an independent predictor of a delay in seeking medical care for symptoms of a heart attack. Women tended to minimize the impact of their disease and did not want to bother others with their health problems.26,27 Social support in the recovery process, including personal encouragement, instrumental (household) support and open communication, has been shown to have high predictive value for affective and cognitive readjustment.28 Specifically in the case of surgery, patients who live alone may delay surgery for fear of having no one at home to care for them after surgery.13
Our study demonstrates that, although patients who lived alone presented with greater joint pain and dysfunction, they gained the same absolute benefit from surgery as did those who lived with another person. However, once we adjusted for their greater level of pain and dysfunction at the time of presentation, those who lived alone received relatively less benefit from surgery. Others have shown that preoperative function is a powerful predictor of postoperative function;29–31 however, we found that living status had an arguably greater effect. For example, the effect of living alone on WOMAC scores 1 year after surgery was greater than the impact of an increase of more than 1 standard deviation in preoperative WOMAC score. Therefore, an important component of any postoperative rehabilitation plan should include assessment of living status.
We believe that there is a need to proactively identify and to inform individuals who live alone of the support services available to those with arthritis, particularly after joint replacement surgery. Given that people who live alone present with greater preoperative pain and dysfunction, primary care physicians and allied health professionals need to encourage the use of available support services to patients at risk, even before the decision for surgical management is made.
An alternative interpretation of our results is that the level of support available to individuals who live alone is insufficient for their needs, rather than just being under-used. We suggest that, as part of discharge planning, the patient’s level of assistance at home should be considered and that those who live alone should receive greater in-home support after surgery, such as prolonged physiotherapy, assistance with homemaking and meal preparation. The nature and duration of support required to improve outcomes requires further study.
There are potential limitations of our study. The first is the 72% response rate among patients eligible to participate. However, we found no differences between responders and nonresponders in terms of age, sex, BMI or baseline comorbidity, and we believe that our conclusions are valid and generalizable. Second, our definition of living status does not take into consideration further social supports that a patient may have available to them, including a community network of friends and family. Third, we did not collect data about whether these patients were discharged home or to an inpatient rehabilitation facility after surgery; however, randomized trials have shown that the destination after discharge does not affect clinical outcomes.32,33 Fourth, we evaluated only patients who reported outcomes using the WOMAC index; however, future work should evaluate these findings using more objective outcomes such as the timed up and go test.34
Conclusion
To our knowledge, this is first study to show that patients who live alone may delay joint replacement surgery until an older age compared with those who live with someone. Patients who lived alone and those who lived with someone received enormous benefit from surgery; however, there is an opportunity to improve the care of patients who live alone after surgery. These findings merit the focus of our public health system to meet the demands created by the 2 trends: an increasing proportion of individuals living alone and a demographic transition that continues to increase the need for hip and knee replacement surgery.
Footnotes
Competing interests: None declared.
Contributors: Drs. Gandhi, Razak, Davey and Mahomed designed the study. Drs. Davey and Mahomed acquired the data, which Drs. Gandhi, Razak, Rampersaud and Mahomed analyzed. Dr. Gandhi and Razak wrote the article, which Drs. Davey, Rampersaud and Mahomed reviewed. All authors approved publication.
- Accepted August 8, 2009.
References
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.