


Abstract
Background: I conducted a prospective study to assess the effectiveness of an absorbable calcium hydroxyapatite (Hac) layer mixed with vancomycin applied to the articular surface of prosthetic implants in preventing deep infections after non-cemented total knee arthroplasty (TKA). This severe complication of TKA occurs in 2%–7% of cases.
Methods: In all, 135 consecutive noncemented TKAs were performed in 126 patients, who were divided into 2 groups. Group 1 comprised 73 knees that received a non-cemented implant without any local anti-infection treatment. Group 2 comprised 62 knees that received a noncemented implant with the local anti-infection agent, which consisted of a pasty mixture of 2 g absorbable Hac and 1–2 g vancomycin. The paste was spread in a thin layer on the articular surface of the implants. Patients in both groups received systemic antibiotic therapy.
Results: In group 1 (no local anti-infection agent), there were 3 deep infections (4.1%) in the early (< 2 mo) or intermediate (2 mo to 2 yr) period after surgery, but no signs of loosening. The infections were treated by arthroscopic debridement and antibiotic therapy. There were no infections or loosening of joints in group 2.
Conclusion: This study shows that a local anti-infection treatment is an effective supplement to systemic antibiotic therapy for the prevention of deep infections in noncemented TKA.
Deep infection in total knee arthroplasty (TKA) is a serious and expensive side effect with serious functional consequences. Many studies on the prevention of deep infection after cemented TKA, in which the articular implants are fixed with acrylic cement (polymethylmethacrylate), have been reported.1–12 The infection rate ranges from 1% to 23%.14–31 These studies analyzed the results of systemic perioperative antibiotic prophylaxis, continued for 1 or 2 days after surgery, as well as cement impregnated with antibiotics. Studies on this double prophylaxis, with optimal conditions in terms of asepsis of the operative field and surgical technique, showed that the incidence rate of deep infection was reduced to 2%–7%.
Perioperative antibiotic administration is effective in reducing deep infection rates, but the prevalence is still 2%–7% in most studies. One recent study showed the superiority of double antibiotherapy prophylaxis over systemic antibiotics alone.13 It has been experimentally shown that, with use of cement containing vancomycin, the bone concentration of vancomycin was 100 times the minimum inhibitory concentration (MIC) for infection after surgery and up to 4 times the MIC 6 months after surgery.15
Infection in cemented TKA can lead to prosthetic loosening and bone destruction. Adapted antibiotic treatment alone is not effective because the cement acts as a barrier to osseous diffusion of the antibiotic, and revision surgery, in 1 or 2 sessions, is hard on the patient. Infection in non-cemented TKA, the type of implant I have used since 1988, is easier to treat and does not always require prosthetic revision.
Because the infection rate after knee arthroplasty is still high, I analyzed the results of a prospective series of 135 noncemented TKA patients to assess the effectiveness of a new local anti-infection system consisting of a mixture of absorbable calcium hydroxyapatite (Hac) and vancomycin in preventing of infection after surgery.
Methods
From 2002 to 2006, 148 patients received 157 consecutive primary noncemented TKAs (9 bilateral). The non-cemented TKAs were all of the same type, with tibial stem and condylar plots, with incorporation of the bone into the prosthesis by bone regrowth on a microporous metallic articular surface coated with calcium hydroxyapatite, and with a mobile polyethylene platform without conservation of the cruciate ligaments (types of implants included LCS by DePuy, Score by Amplitude and TKS by Aston Medical).
I systematically performed all kneecap replacements with polyethylene implants that were either cemented (123 cases) or not cemented (implanted in press-fit for TKS in 24 cases). The surgical technique used was identical to the medial parapatellar approach and midvastus, without tourniquet, with electrocoagulation and recovery of the blood loss (Cell Saver by Haemonetics), using deep sutures with Vicryl (Ethicon) and continuous subcutaneous sutures (Vicryl) with fast resorption, in a standard operating room under ultraviolet light without laminar flow ventilation.
The 135 noncemented TKAs were assigned to 1 of 2 groups: without (group 1) or with (group 2) anti-infection local treatment. The first 12 TKAs were randomly assigned to a group (7 to group 2), and then the subsequent TKS were alternately assigned to group 1 or 2. A pasty mixture of 2 g of an absorbable Hac (either biologic Hac Pro Osteon or synthetic Hac and collagen Collapat II, which is a sponge-like material and easily manipulated; both by Bio-met) with 1–2 g vancomycin (powder), and a few drops of physiologic serum were used. The preparation of the mixture was fast (< 1 min). The paste was spread into a thin layer before setting the implants. At the beginning of the study, the paste was spread on the articular surface of the femoral and tibial prosthetic devices. I now spread the paste on the tibial implant or the tibial bone layer.
I measured parameters such as length of surgery, draining and hospital stay, blood loss, transfusions, long-term results, and pre- and postoperative International Knee Society (IKS) scores.
Before surgery, all patients received intravenous antibiotic therapy (cefazoline 500 mg), which was continued during the first 48 hours after surgery (2 g/d). The anesthesia was either regional (spinal) or general (51 patients in group 1, 42 patients in group 2). A crural block was added for 68 knees in group 1 and 56 knees in group 2. For 4 patients in group 2, I obtained samples on day 3 or 4 (the day the drain was removed) of the drained fluid for measurement of vancomycin concentration in the fluid.
After surgery, functional control was measured after 3 and 6 weeks, 3 and 6 months, and then every second year. Radiography was done during the sixth week after surgery, at 6 months and at the last visit. Early (within 2 mo after surgery), intermediate (2 mo to 2 yr) or late (> 2 yr) infections were classified as superficial or deep intra-articular. Deep infections were confirmed by articular fluid culture. I used the Student t test to compare the results between the groups.
Results
Of the 148 patients (157 knees) who underwent TKA, 22 were excluded from the study (Fig. 1). Patients lost to follow-up were also excluded. In total, 126 patients who received 135 noncemented TKAs were enrolled in the study. Patients had no signs (no clinical symptoms, normal erythrocyte sedimentation rate and C-reactive protein level) of infection before or during the surgery.
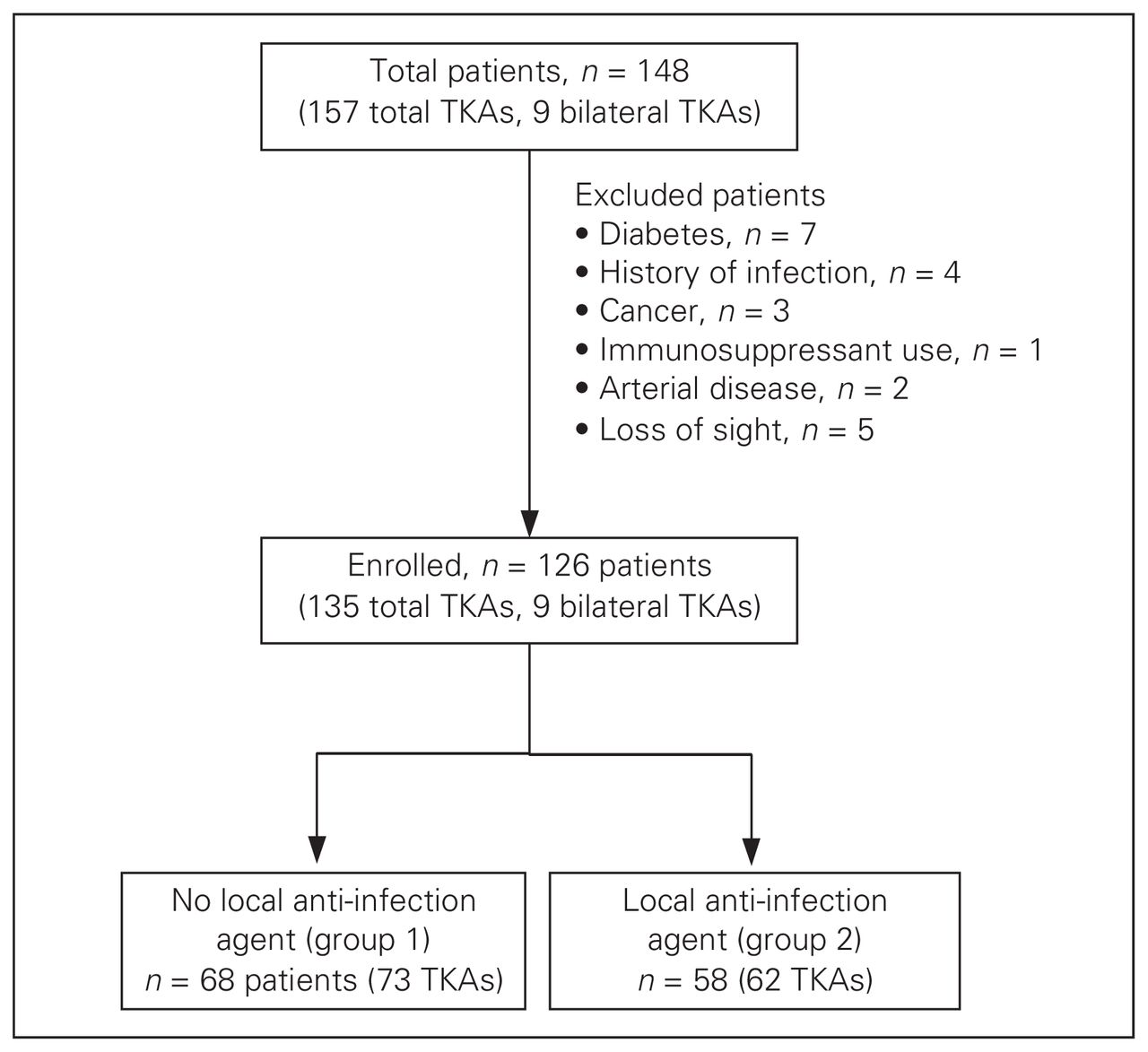
Flow of patients through the study. TKA = total knee arthroplasty.
Group 1 comprised 73 knees (68 patients) that received noncemented TKA without the anti-infection agent. The mean age of patients in group 1 was 72 (51–87) years. Most of the patients in this group were female (56 knees). The preoperative diagnosis was primary degenerative arthritis in 67 knees, posttraumatic arthritis in 4 knees and aseptic necrosis in 2 knees.
Group 2 comprised 62 knees (58 patients) that received noncemented TKA; these patients received the anti-infection agent. The mean age in group 2 was 73 (55–89) years, and most were female (46 knees). The preoperative diagnosis was primary degenerative arthritis in 57 knees, posttraumatic arthritis in 3 knees and aseptic necrosis in 2 knees.
There was no significant difference between the 2 groups (p > 0.05) for parameters such as age, sex and pre-operative diagnosis (Table 1). There were also no significant differences between group 1 and 2 for the duration of surgery (mean 75 and 80 min, respectively), blood loss (mean 450 and 500 mL), length of draining (3–5 d), duration of hospital stay (6–9 d), knee IKS score before (mean 39 and 41) and after (mean 95 and 96) surgery, and length of follow-up (3–7 yr). The postoperative follow-up was identical for each patient, with walking with a cane and complete support on the second day, active knee mobility and no immobilization device used.
Demographic and surgical characteristics of patients included in the study of the effectiveness of a local anti-infection agent during total knee arthroplasty
Superficial and localized infections caused by Staphylococcus epidermidis were noted in both groups in the early stages of healing (2 infections in group 1 and 1 in group 2). These infections were treated with local and oral antibiotics, without any consequences or significant differences.
At the last follow-up, there were no infections or loosening of implant in either group. The vancomycin concentration in the drained fluid, sampled from 4 cases in group 2, was about 12 times the MIC. In group 1, there were 3 deep infections caused by Staphylococcus aureus (4.1%) during the early and intermediate stages; the infections were treated by arthroscopic debridement and antibiotics. The difference between the 2 groups for infection was significant (p = 0.014).
Discussion
Perioperative antibiotic treatment is effective in decreasing the rate of deep infections, but the infection prevalence remains between 2% and 7% in most series. A recent study showed the superiority of double antibiotic prophylaxis (systemic and in the cement) compared with systemic antibiotic prophylaxis alone.
Infection in noncemented TKA is easier to treat, sometimes without the need for a change of prosthetic device. I began performing noncemented TKA in 1988 because experience with noncemented total hip prosthesis coated with calcium hydroxyapatite (Landos Corail; Landanger/DePuy)26,27 demonstrated its longevity.27–32 Between 1988 and 2001, I performed 439 noncemented TKAs, with a global infection rate of 3.8% (17 cases, data not shown).
In the present study, the main objective was to assess the effectiveness of a new anti-infection agent in preventing deep infections after noncemented TKA. Three infections (4.1%) developed in the group that did not receive local antibiotic protection; these infections were treated by arthroscopic debridement and antibiotherapy. No infections developed in the group that received the anti-infection agent. The articular concentration of antibiotics, measured in 4 cases, was above the MIC. The difference in infection rate between the 2 groups was significant.
The lifetime of noncemented TKA is at least equal to that of cemented TKA, as long as there is perfect alignment of the implant and the lower limb and good frontal ligament stability. One advantage of noncemented implants is the easier treatment of aseptic or septic loosening, with less bone destruction due to the presence of cement, which is also a barrier for systemic antibiotic therapy. The use of an antibiotic in an absorbable Hac paste that covers the articular face of the implant allows for stronger resistance to infection during the postoperative period because of the bone concentration of antibiotic and the progressive dilution of antibiotic in the articular liquid, coupled with systemic antibiotic therapy. This is a simple procedure that increases the resistance to infection, with no mechanical consequences such as loosening. An additional study involving more patients and a longer follow-up time (10–15 yr) should be performed, and the articular antibiotic concentration should be measured in the first year after surgery.
Conclusion
The effectiveness of a new anti-infection system as a complement to systemic antibiotic therapy in the prevention of deep infection after TKA has been demonstrated. Because this method is simple to use and has an extremely low cost, I encourage its use and believe that its use can be extended to include patients at risk of infection (patients with diabetes or previous surgeries).
Footnotes
Competing interests: None declared.
- Accepted September 30, 2009.
References
In this issue

{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.