


Summary
Multiple studies confirm that point of care ultrasound (PoCUS) has a high sensitivity and specificity for cholelithiasis and cholecystitis. However, there is poor perceived reliability of biliary PoCUS by surgeons. This survey was performed to assess surgeons’ opinions on using PoCUS in gallstone disease and barriers that exist for its institution. The majority (60.3%) of respondents reported a total lack of confidence in PoCUS for the diagnosis of biliary disease. Most felt the sensitivity of PoCUS was poor and had concerns about the user-dependent nature of the test and the lack of imaging details provided. If offered ideal clinical/laboratory findings with PoCUS results, only 4.7% of surgeons would definitely operate for unremitting biliary colic and 5.4% for cholecystitis. The ability to replicate findings independently increased confidence in clinical decision-making. Our findings suggest there is substantial distrust in biliary PoCUS but that specific ultrasound training for the surgical workforce may prove tremendously beneficial for its utilization.
Gallstone disease affects more than 20 million Americans yearly.1 In Ontario, 260 elective cholecystectomies per 100 000 patients are performed each year.2 Point of care ultrasound (PoCUS) has a growing role in the diagnosis of gallstone disease.3 Results of PoCUS are similarly accurate compared with formal radiology-performed ultrasounds.4 Emergency physicians who use biliary PoCUS improve emergency department (ED) throughput and reduce length of stay in the ED.3 However, surgeons still depend on formal radiology-performed imaging for the management of biliary disease.5
We surveyed surgeons about their opinions of biliary PoCUS. Our objectives were to quantify surgeon confidence in biliary PoCUS and elucidate possible barriers to use in order to improve surgeon utilization.
Our approach
A cross-sectional survey was emailed to general surgery program directors from the 14 primarily English-speaking academic programs in Canada. They were asked to distribute the survey to all general surgery residents, fellows and staff associated with their centre and to provide us with the number of survey recipients so we could determine the overall response rate.
To explore the factors associated with confidence in biliary PoCUS, we dichotomized confidence by considering everyone who answered “slightly confident” to “extremely confident” as having some confidence with PoCUS and those who answered “unconfident” as being unconfident with PoCUS. All other variables were dichotomized as seen in Box 1.
Dichotomization of factors used in data analysis
| Factor | Responses considered staff level, frequent, high sensitivity or management altering | Responses considered trainee level, infrequent, low sensitivity or not altering management | ||||
|---|---|---|---|---|---|---|
| Level of training | — | Staff surgeon (> 10 years practice) | Staff surgeon (< 10 years practice) | Fellow | Senior resident (years 3–5) | Junior resident (years 1–2) |
| Frequency that PoCUS results are used in practice | Very often | Somewhat often | Occasionally | Rarely | Never | — |
| Frequency of performing PoCUS personally in practice | Very often | Somewhat often | Occasionally | Rarely | Never | — |
| Frequency of referrals based on PoCUS-diagnosed biliary disease | > 20 times | 10–20 times | 5–10 times | 3–5 times | 1–2 times | Never |
| Perceived sensitivity of PoCUS for cholelithiasis | 90%–100% | 80%–90% | 70%–80% | 60%–70% | 50%–60% | < 50% |
| Perceived sensitivity of PoCUS for cholecystitis | 90%–100% | 80%–90% | 70%–80% | 60%–70% | 50%–60% | < 50% |
| Ability to admit, diagnose and/or operate based on PoCUS findings | Yes, definitely | Likely yes | Maybe | Likely no | No, definitely not | — |
PoCUS = point of care ultrasound.
We also distilled 5 potential barriers to applying the results of biliary PoCUS in clinical practice: perceived poor test characteristics, user-dependent nature of the technology, poor documentation of results, lack of personal ability to replicate the test, and lack of detailed imaging findings. We analyzed the response data to model the relationships between the survey respondents’ attitudes and experience of PoCUS in diagnosis and management of biliary disease.
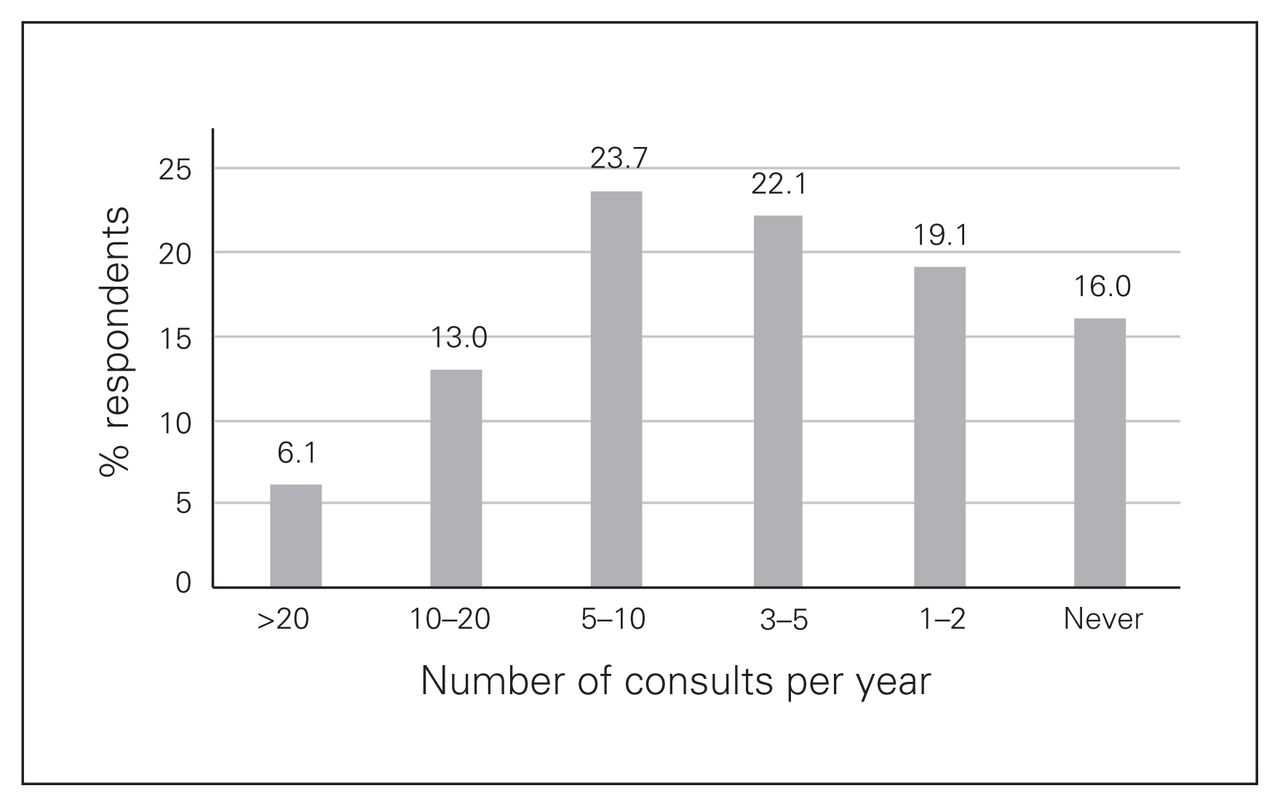
Eleven of 14 schools responded to our request to participate, totalling 132 general surgery staff and residents. The overall national response rate was 25.2%. Responses indicated most surgeons had previous experience with PoCUS. Almost half had some form of PoCUS training (43.5%). Most occasionally used the results of PoCUS (25.9%), though they rarely/never personally performed the test (58%). Surgeons were familiar with PoCUS done by emergency physicians (88.5%), and most received 5–10 consults per year based on biliary PoCUS (23.7%) (Fig. 1).
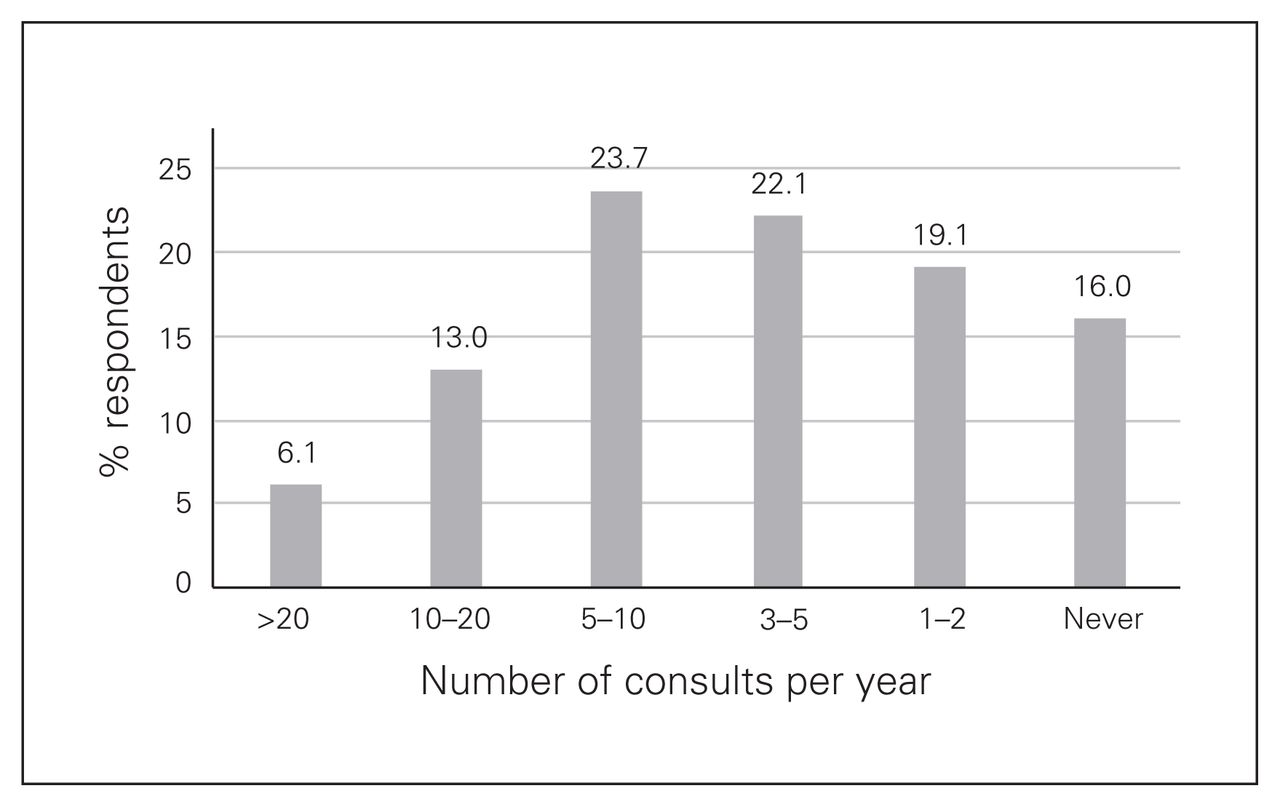
Number of consults per year from emergency department on the basis of point of care ultrasound for suspected biliary disease.
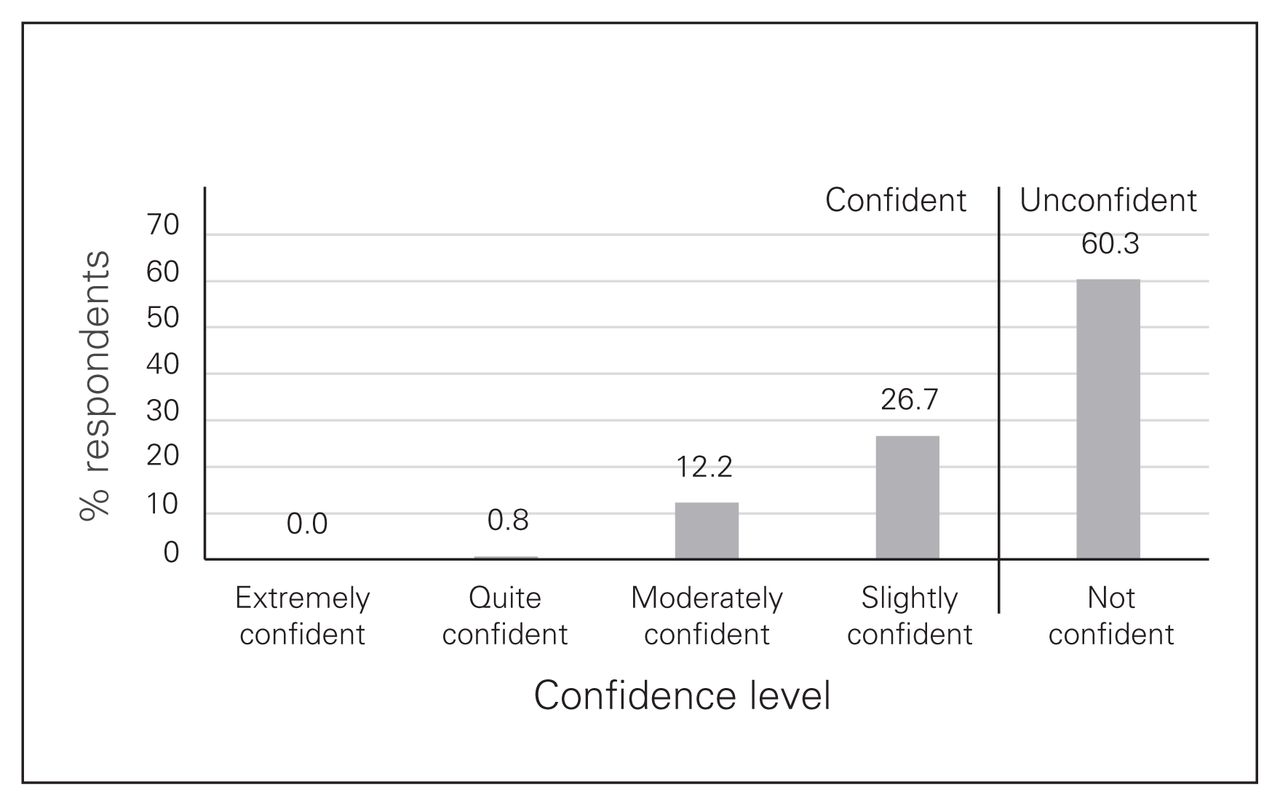
The majority (60.3%) of respondents had a total lack of confidence in biliary PoCUS, and 26.7% were slightly confident (Fig. 2).
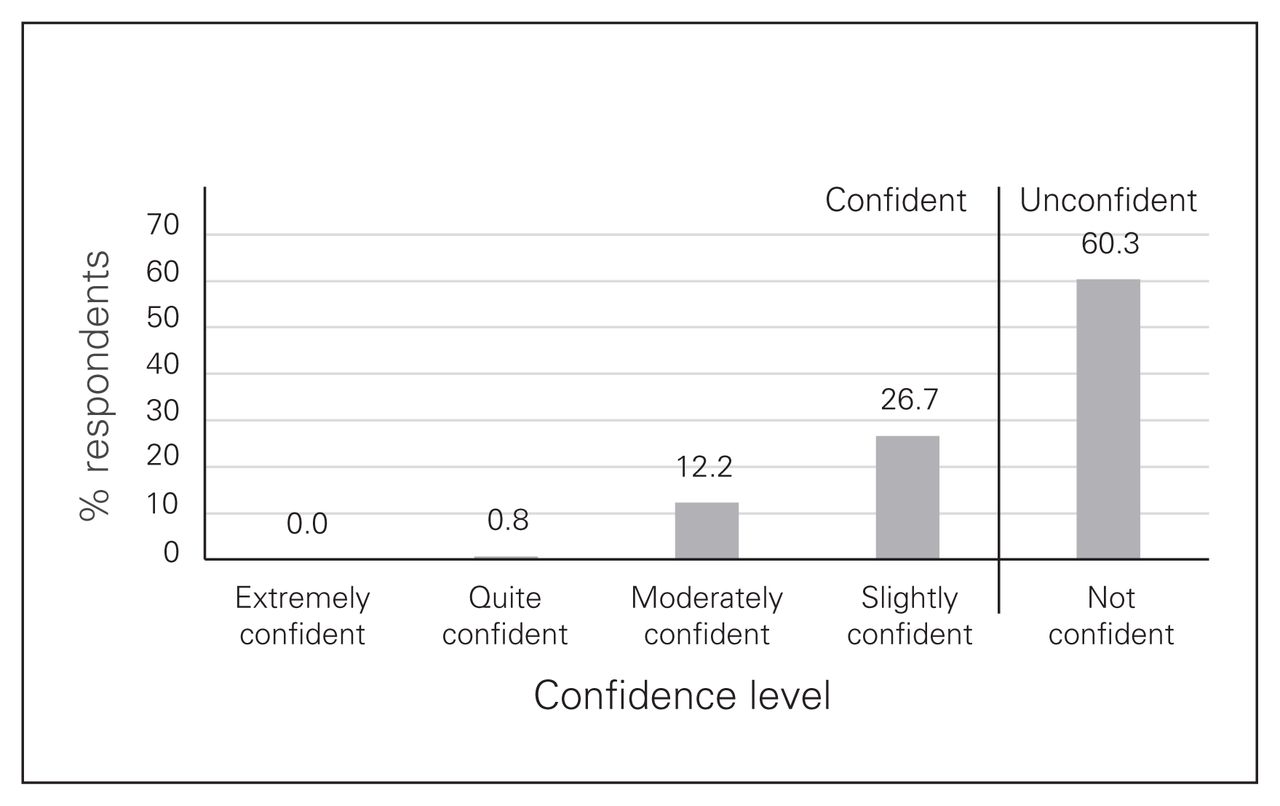
Confidence in diagnostic information on the basis of point of care ultrasound in patients with biliary disease.
Surgeons felt the test characteristics of PoCUS for cholelithiasis was modest (median 70%–80%). Almost half (48.9%) felt the sensitivity for cholecystitis was less than 50%. Other barriers to using PoCUS included how the test is documented and the user-dependent nature of the test. Most felt that if they were able to perform biliary PoCUS themselves, their confidence would increase (79.8%).
Hypothetical clinical decision-making using PoCUS in patients with classic biliary colic and cholecystitis also showed low confidence in the technology (Table 1).
Clinical decision-making using biliary PoCUS
On univariate analysis, multiple factors were found to significantly affect the confidence of surgeons using biliary PoCUS (Table 2). A regression analysis was additionally performed to assess which modifiable factors independently affected clinical decision-making. Ability to personally replicate the test independently affected a surgeon’s willingness to diagnose unremitting biliary colic (odds ratio [OR] 3.57, p = 0.02), operate for unremitting biliary colic (OR 8.53, p = 0.05) and diagnose cholecystitis (OR 2.87, p = 0.05).
Factors associated with level of confidence in biliary PoCUS results
Differences between trainees and staff were evaluated. Residents more frequently used the results of PoCUS (74.0% v. 51.9%, p = 0.01) and performed their own ultrasounds (50.6% v. 29.6%, p = 0.02). They were more aware of the ED use of PoCUS (96.1% v. 77.8%, p = 0.002) and received more referrals (53.2% v. 27.8%, p = 0.004). Their confidence in the test was, however, the same (40.2% v. 39.9%, p > 0.99). Additionally, trainees were less willing to treat patients based on the results of biliary PoCUS.
Discussion
To our knowledge, we were the first to investigate how Canadian general surgeons are using biliary PoCUS results in their practice and the barriers to its adoption.
Currently, there is a lack of confidence in the results of biliary PoCUS. A potential source of hesitation among surgeons may be incomplete knowledge translation from the literature. Recent reviews have shown that PoCUS sensitivity for cholelithiasis and cholecystitis is 89.8%5 and 87%, respectively.4 In our survey, most surgeons believed the sensitivity for cholelithasis and cholecystitis was 70%–80% and < 50%, respectively.
This study identifies modifiable factors that may affect surgeons’ confidence in biliary PoCUS. Education around the documented sensitivity of biliary PoCUS, training to replicate the test, and the availability of an online report would all be beneficial. The time commitment required to achieve this training is likely small, as evidence shows surgeons developed PoCUS skills quickly after a short didactic and hands-on education session.6
There were multiple differences between the responses of residents and staff. Trainees appeared to have greater exposure to biliary PoCUS than staff. However, their confidence in the test was the same as staff. Additionally, they were less willing than staff to operate based on a PoCUS study. We speculate that this may stem from a lack of confidence in their clinical diagnostic skills or from a concern that their staff would require formal imaging before proceeding to operate. However, more research is required to explain these discrepancies.
Conclusion
Our survey shows an opportunity for improvement in surgical care. Surgeons are missing an opportunity to provide efficient care when biliary disease is identified by emergency physicians. Our study identifies a knowledge translation gap that, if bridged, may lead to more efficient patient care.
Footnotes
Competing interests: R. Leeper is an associate editor of CJS; he was not involved in the review of or decision to accept this paper for publication. No other competing interests were declared.
Contributors: All authors contributed substantially to the conception, writing and revision of this article and approved the final version for publication.
- Accepted April 24, 2019.
In this issue

{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.