


Article Figures & Tables
Figures
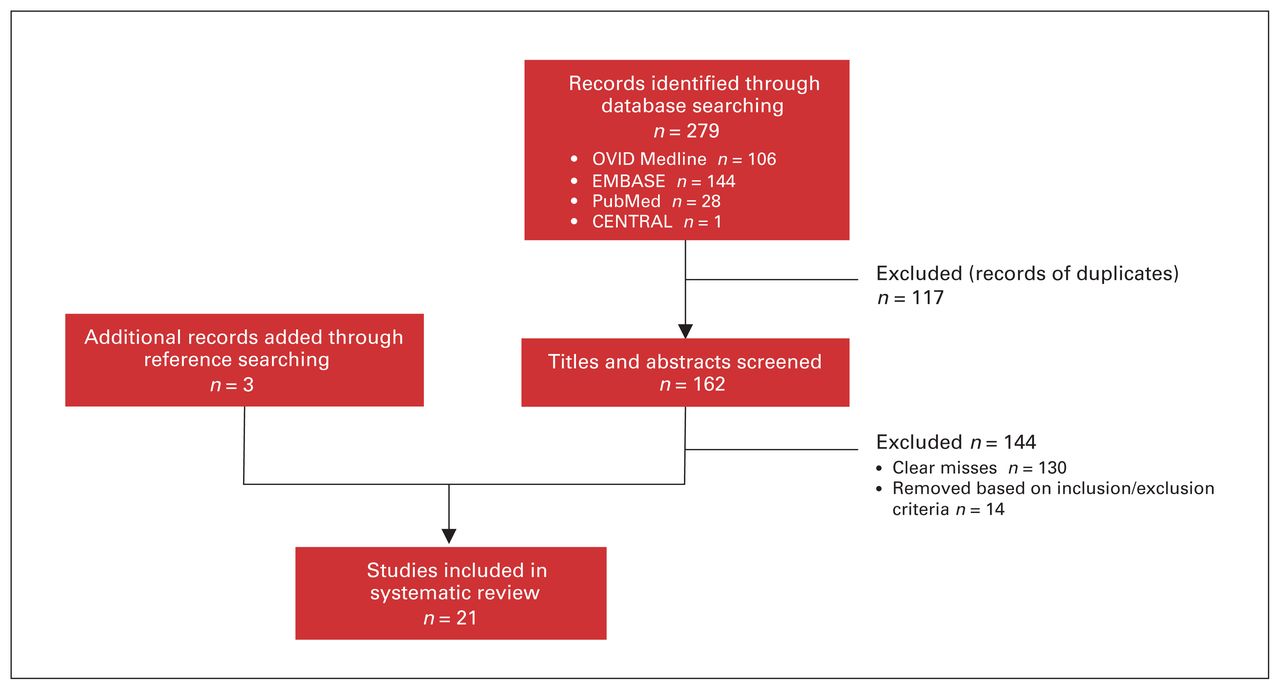
- Fig. 1
Selection of studies included in the systematic review.
Tables
- Table 1
Summary of results from a narrative systematic review of studies to improve morbidity and mortality conferences (MMC) in general surgery and subspecialties (part 1 of 3)
Study Summary MMC intervention(s) Outcome(s) Comment(s) Abu-Zidan and Premadasa (11) Single surgical department identified perception of MMC, implemented changes, and used a postintervention 5-point questionnaire Notification of cases to present 2 days before MMC
Presentation limited to 15 minutes
Mandatory literature summary
Increased presentation quality and communication clarity
Increased satisfaction
Increased identification of remediation strategies
Very small sample size
Small absolute difference on postintervention questionnaire
Antonacci et al. (41) Three hospitals and 1 ambulatory care facility implemented an error analysis methodology and provided report cards to individual surgeons Standardized case critique (what, who, why, when)
Analysis of adverse events for quality-dependent factors
Potential quality issues were identified via consensus and graded<
Adverse events caused by quality issues were sent to surgeons and chairperson as a report card
Reduction in age-adjusted mortality
Privileges restricted or removed for surgeons (3%)
Pushback from surgeons
Three times greater identification of quality issues
Implementation of error analysis may be difficult at community hospitals
Lacks cost–benefit analysis and analysis among institutions
Lacks preintervention comparison
Auspitz et al. (19) Single surgical department retrospectively reviewed all cases submitted to MMC and compared results to local NSQIP registry NSQIP database (used for a 30-day follow-up period) was compared with MMCs
Similar reporting in portion of major and minor complications between NSQIP and MMC
NSQIP identified a higher proportion of wound site infection and readmissions
NSQIP identified 30-day postoperatiove outcomes
MMC captured nonoperative cases
Retrospective review
Bhalla et al. (32) Single academic centre’s department of surgery compared traditional MMC format to the matrix format and assessed improvement with pre- and postintervention questionnaires PGY 1–3 assigned weekly readings and PGY 4–5 assigned evidence-based literature reviews
Presentations assigned 2–5 days in advance
Audience response system
Post-MMC matrix newsletter
Standardized case selection by MMC moderator
Residents spent less time preparing and reported learning more
Enhanced learning reported from other presentations
Matrix format was significantly more preferred
Faculty and resident perceived greater presentation quality
Small sample size with drop-off in responses
Potential for Hawthorne effect
Increased MMC presentation may be because of enhanced MMC appreciation not format change
Clarke et al. (35) Single hospital retrospectively reviewed MMC format change and analysis using error taxonomy MMC was run by a dedicated moderator
Standardized PowerPoint template
Taxonomic analysis (domain, impact, type, cause and prevention) of adverse events for human-related error
Enhanced identification of the contribution of error to adverse events
Descriptive results that lack a preintervention comparison
Small sample size
Limited generalizability
Cromeens et al. (20) Single pediatric surgical service retrospectively compared NSQIP-P to morbidity and mortality identified by MMCs Increased MMC frequency from bimonthly to weekly
Reported straightforward complications
Retrospective use of NSQIP-P to identify complications
No difference in mortality identified between MMCs and NSQIP-P
Increased MMC reporting of morbidity with format changes
Increased reporting of morbidity by NSQIP-P as compared with MMCs
Generalizability may be limited to pediatric surgery
NSQIP-P has exclusion criteria that did not capture all morbidity and mortality identified by MMC
Cromeens et al. (42) Single pediatric surgical service implemented a taxonomic error analysis strategy and standardized MMC structure Consistent and multidisciplinary MMC
Established documentation system using taxonomic error analysis
Taxonomic system enabled identification of errors into categories beyond surgical and patient diseases
Case selection may not have been comprehensive
Small sample size
Lacks pre-intervention comparison
Falcone and Watson (38) Multiple campuses at a single medical centre used teleconferencing to improve MMC attendance and provided a cost–benefit analysis Implemented a teleconferencing system
Increased faculty attendance
Travel time reduction resulted in positive net cost–benefit analysis
Retrospective study reliant onself-reports
Generalizability may be limited to centres with multiple campuses and long commute times
Greco et al. (39) Single division of general surgery invited a clinical librarian to MMC and assigned research questions to MMC attendees, to be completed with librarian assistance Clinical librarian invited to attend MMCs
Residents assigned relevant questions from MMC to be researched and presented at next MMC
Presentation of assignments increased perceived continuity between MMCs
Speculation that librarian assistance increased resident research skills
No objective analysis of outcomes
Limited to centres with access to a clinical librarian
Limited postintervention feedback
Gurien et al. (17) Single department of surgery retrospectively compared NSQIP and MMC registries for commonality NSQIP employed to identify incidence of morbidity and mortality
NSQIP increased reporting comprehensiveness of morbidity and mortality
Limited generalizability as not all institutes subscribe to NSQIP
NSQIP limited to sampling process that does not capture nonoperative procedures
Hutter et al. (18) Single general surgery service retrospectively compared data from MMC and NSQIP registry for commonality NSQIP used to identify incidence of morbidity and mortality
NSQIP demonstrated increased incidence of morbidity and mortality compared with MMCs
NSQIP captures only operative patients, whereas MMC also captures nonoperative
Small sample size limited subgroup analysis
Suggested creation of an NSQIP integrated Web-based reporting for MMC
Kim et al. (29) Five divisions from 1 department of surgery employed format changes to their MMC and assessed efficacy with a pre- and postintervention questionnaire Presenters instructed to provide brief clinical histories and literature reviews
Presentation limited to 15 minutes
Instruction to analyze case presented for underlying cause of complication(s)
Electronic sample presentation template provided
Presentations lasted 15–20 minutes owing to questions
Increased specificity of the cause of complication
Increased specificity of future practice change(s)
Increased positive response from residents
Small sample size
Drop-off in participants from pre- to postintervention questionnaires
Prospective study
Kong and Clarke (34) Single metropolitan trauma service introduced a structured MMC and HEMR to report morbidity and mortality HEMR used to capture routine data, generate reports on morbidity and mortality, and compare with MMC data
Introduction of a multidisciplinary MMC
HEMR increased morbidity, specifically for systemic complications
Increased identification of common clinical scenarios associated with error and morbidity
Retrospective study
Lacks preintervention comparison
Lewis et al. (37) Single department of surgery conducted a prospective study in which participants were randomly assigned to attend MMC live or via televideoconference and response was assessed with an anonymous survey Implemented televideoconferencing system
No significant difference in learning among faculty, residents, and students
No significant difference in perceptions
Increased favourable perceptions for televideoconferencing as commuting distance increased
Potential for decrease in audience interaction with televideoconferencing
Uneven representation in faculty, residents and student participants
Number of questions to detect learning may have been inadequate
McVeigh et al. (21) Single department of surgery conducted a prospective comparative study over 6-mo period concerning reporting of adverse events comparing MMC and a proforma Prospective proforma used to identify incidence of morbidity and mortality
Increased capture of morbidities with proforma
Increased capture of mortalities with proforma
Differences may be due to surgeons not reporting all complications
Potential Hawthorne effect
Mitchell et al. (12) Single department of surgery conducted prospective study concerning standardization format for MMC using preand postintervention questionnaires and a multiple-choice questionnaire (MCQ) to assess knowledge Standardized SBAR presentation format
Mandatory resident and faculty attendance
Decreased defensiveness and blame
Mandatory use of PowerPoint
Radiographic images encouraged
Focused analysis of error
Integration of evidence-based literature
Facilitated audience participation
Facilitation of the conference by a moderator
SBAR was positively regarded by presenters and reported as easy to implement
Modified MMC format did not add to preparation time
Presentation quality improved significantly in background, assessment, and recommendation
Improved MCQ scores from all learners
Large sample size
Potential Hawthorne effect
Assessor bias
Absolute increases reported on Likert scale were small but significant
Mitchell et al. (33) Single department of surgery conducted a prospective observational study testing a modified MMC presentation format Implementing SBAR MMC tool at weekly departmental MMC
Increased presentation quality
Increased communication clarity
Increased attendee satisfaction
Increased identification of remediation strategies
All assessors were familiar with residents so there was potential bias
Murayama et al. (30) University medical school conducted a prospective observational test using a 23-item survey before and after implementation of a modified MMC format Quicker summary of pertinent aspects of cases (5–10 min)
Limited literature review (5–10 min)
Discussion stimulated by moderator
Moved from 6 pm to 7 am
Residents encouraged to discuss case with attending prior
Increased faculty and resident attendance
Increased faculty contribution and analytical thinking
Residents preferred modified formats
Attending surgeons disliked shorter literature review
Small sample size
Single centre
Drop-off in survey response between pre- and post
Greater resident response, skewed to juniors
Possible Hawthorne effect
Prince et al. (36) Single department of surgery at a tertiary academic medical centre implemented an interactive MMC format and analyzed the effectiveness using a questionnaire Directed questions to audience
Provided explanations during session
Asked questions to attending faculty members
Included illustrative slides and videos
Moderator stimulated and facilitated discussion
Increased perceived educational value
Increased clinical confidence related to MMC cases
Incomplete or missing data
Hawthorne effect and practice effect may have been confounding
Prospective longitudinal analysis
Lacks preintervention comparison
Risucci et al. (31) Single department of surgery conducted a prospective study in which a modified MMC was investigated using pre- and postintervention questionnaires Conference lengthened from 60–90 min with 3 cases presented
Mandatory PowerPoint use that followed a uniform format concerning timing of diagnostic inquires, consultations, and procedures
Mandatory brief literature review
Increased multi-disciplinary attendance
Error discussion is focused on timeliness and appropriateness of diagnosis and treatments
Consensus was reached more often
Complications were perceived as more often avoidable
Strategies for prevention were more likely to be identified
Increased percentage of complications attributed to errors in judgment
Speculation that modified MMC facilitates more detailed description and analysis of a patient’s entire clinical course
Small sample size
Prospective study
Small number of nonsurgical personnel included in survey, which may limit generalizability
No faculty surveyed
Vogel et al. (40) Single department of surgery conducted a prospective study which incorporated MMC findings into a PDCA cycle Conducted MMC within a PDCA cycle format
Significant reduction in anastomotic leak rate
Authors report potential for random errors at each step in the PDCA cycle
May not be generalizable beyond colorectal surgery
HEMR = hybrid electronic medical registry; MMC = morbidity and mortality conference; NSQIP = National Surgical Quality Improvement Program; NSQIP-P= National Surgical Quality Improvement Program-Pediatrics; PDCA = plan-do-check-act; PGY = postgraduate year; SBAR= situation, background, assessment, recommendation.
- Table 2
Stratification of literature review results into themes, goals, specific interventions and supporting studies
Theme Goal Intervention Supporting studies Educational value Standardized presentations Time limit < 15–20 min Abu-Zidan and Premadasa, (11) Kim et al., (29) Murayama et al. (30) Mandatory brief literature review Abu-Zidan and Premadasa, (11) Kim et al., (29) Mitchell et al., (12) Murayama et al., (30) Risucci et al., (31) Bhalla et al. (32) PowerPoint template Kim et al., (29) Risucci et al. (31) SBAR format Mitchell et al., (12) Mitchell et al. (33) Advanced notification of selection to present* Abu-Zidan and Premadasa, (11) Bhalla et al. (32) Matrix format† Bhalla et al. (32) Increased audience interaction Audience response system Bhalla et al. (32) Moderator facilitation of discussion Clarke et al., (35) Murayama et al., (30) Mitchell et al., (12) Prince et al. (36) Targeted questions to specific audience members Prince et al. (36) Enhanced morbidity and mortality continuity Assigned research for all unanswered questions to be reported at the next MMC Bhalla et al., (32) Greco et al. (39) Error analysis Improved error analysis Focused analysis on underlying cause of complication Antonacci et al., (41) Kim et al., (29) Mitchell et al. (12) Taxonomic error analysis‡ Clarke et al., (35) Cromeens et al. (42) Case selection and representation Comprehensive case selection Electronic database used to identify cases Auspitz et al., (19) Cromeens et al, (20) Gurien et al., (17) Hutter et al., (18) Kong and Clarke (34) Moderator selects cases Bhalla et al. (32) Prospective proforma McVeigh et al. (21) Attendance Improved faculty and resident attendance Teleconferencing Falcone and Watson, (38) Lewis et al. (37) Morning meeting time Murayama et al. (30) Dissemination Established systematic dissemination strategy Post-MMC newsletter Bhalla et al. (32) PDCA cycle Vogel et al. (40) Surgeon report cards Antonacci et al. (41) MMC = morbidity and mortality conference; PDCA = plan-do-check-act; SBAR = situation, background, assessment, recommendation.
↵* Advanced notice of selection to present ranged from 2 days (11) to 2–5 weeks (32) and included dissemination of the cases to be presented to prospective MMC attendees to allow time for background research.
↵† Matrix format is a cyclical MMC that involves a designated moderator selecting cases, helping residents with presentations, facilitating discussion, and testing the residents quarterly to create a learning environment that constantly reinforces MMC learning points. (43)
↵‡ Taxonomic error analysis involves categorizing errors to facilitate more specific reporting and analysis of the root cause. Examples of taxonomic categories include domain, impact, type/process, cause, and prevention (35) or more complex determination templates. (42)
Problem Recommendation How to improve education value of MMC Enforce a time limit < 15–20 min
Standardize presentations with a PowerPoint template or SBAR format
Dedicated moderator to facilitate discussion
Target discussion questions to specific audience members or use an audience response system
Assign all unanswered questions as a research question to learners to be reported at the next MMC
How to improve error analysis Focused discussion on causative factors
Taxonomic error analysis
How to better represent morbidity and mortality with case selection Use an electronic database (e.g., NSQIP) to identify cases for presentation
Dedicated moderator to select cases for presentation
How to improve MMC attendance Teleconferencing for geographically separated centres
Plan MMCs in the morning before operating hours
How to improve continuity and dissemination of MMC content Create and circulate newsletters that highlight salient points of each MMC
Distribute surgeon report cards that detail quality-dependent factors that may have contributed to adverse events
MMC = morbidity and mortality conference; NSQIP = National Surgical Quality Improvement Program; SBAR = situation, background, assessment, recommendation.
Element Description Sensitivity to operations Continuously work to identify variations and errors in complex processes. Reluctance to simplify Avoid overly simplified explanations of failure. Embrace and address complexity in analyses. Preoccupation with failure Work to predict and avoid catastrophes. Place high importance on near misses. Deference to expertise Teams and leaders defer to those with the most front-line knowledge, rather than to those with the most seniority, in analyzing processes and solving problems. Resilience Systems are designed to limit and contain errors before they escalate and to promote resourceful problem solving and improvization in order to maintain function even in the face of setbacks. Collective mindfulness Individuals at all levels and teams operate mindfully to make critical adjustments promptly. There is a culture of continuous evaluation and learning that enables continuous refinement of process and identification of potential problems.
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.