


Abstract
Background Obesity is an important comorbidity affecting outcomes after total joint arthroplasty. Consequently, surgeons may delay care of obese patients to first address obesity through different care pathways. The effect of obesity on patient wait times for total joint arthroplasty has not been explored. The purpose of this study was to evaluate the effect of obesity on access to total hip (THA) and knee (TKA) arthroplasty.
Methods The study data set was constructed from the Nova Scotia Health Authority’s Horizon Patient Folder system and the Patient Access Registry Nova Scotia. Wait time was measured as days between the decision to treat and date of surgery. Body mass index (BMI) was calculated from a preoperative assessment, and patients were grouped into BMI categories. Multivariate log-linear regression was used to test for statistical differences, controlling for confounding factors.
Results We observed longer wait times for TKA with increasing BMI weight class. Patients with BMIs greater than 50 had 34% longer waits than reference weight patients. However, THA recipients showed no statistical difference in wait times across weight categories. Furthermore, there was variability among surgeons in the wait times experienced by patients.
Conclusion The finding of longer wait times for TKAs, but not THAs, among patients who were obese was unexpected. This shows the variable wait times for THA and TKA that patients who are obese can experience with different surgeons. It is important to understand the variability in wait times so that efforts to standardize the patient experience can be accomplished.
Total hip arthroplasty (THA) and total knee arthroplasty (TKA) are successful surgical procedures for the management of end-stage arthritis of the hip and knee, respectively. Patient access to THA or TKA can be variable for a number of reasons; however, the effect of obesity on wait times is not known. It is clear that the presence of obesity is an independent contributor to postoperative complications, including postoperative infections, wound problems, deep vein thrombosis, fracture and premature loosening of the implants.1–4 This has led to a suggestion to delay access to care for obese patients so that their health can first be optimized.1,5 One of the suggested strategies is losing weight before surgery. Weight loss is challenging for most patients and it can take a prolonged amount of time to accomplish meaningful weight loss before total joint arthroplasty (TJA) while a patient is suffering with arthritis.6,7 There has been no consensus in Canada on an appropriate body mass index (BMI) class to delay surgery. It is important to note patients who are obese gain substantial pain relief and functional improvements after TJA.8,9 This could lead to the unfortunate situation of denying care to patients who are obese because of potential complications that they might not actually experience.10
The development of orthopedic assessment clinics has led to efforts to standardize the assessment and management of patients referred for TJA. With the paucity of information around the effect of obesity on wait times for TJA, any efforts to make policy decisions on improving access to TJA will require the association between obesity and wait times to be ascertained. This is important for patients so that they can have an accurate estimate of expected wait time, particularly as these wait times are reported to the public by many provincial departments of health. The purpose of this study was to describe the association between BMI and wait time for THA and TKA. Furthermore, the study sought to determine the variation among surgeons with respect to BMI and wait times for TJA.
Methods
Study population
We constructed the study data set from the Nova Scotia Health Authority’s Horizon Patient Folder (HPF) system and the Patient Access Registry Nova Scotia (PAR NS). The HPF contains information on patient history and physical examination as of the time of the orthopedic clinic visit. The PAR NS provides the date the surgeon and patient decided to proceed with surgery and the actual date of surgery. We used patient postal codes to generate a residential dissimination area identifier, used to link our study data with aggregate census data from Statistics Canada.
The study population included all patients undergoing primary knee and hip replacement surgeries at 2 institutions in Nova Scotia, completed from April 1, 2011, to March 31, 2016. We excluded revisions, arthroscopies and fractures, as well as patients with a BMI < 15. After exclusions for missing information, 4837 patients undergoing THA and 3043 patients undergoing TKA were included in the database.
Outcomes
Our primary outcome was wait time to surgery, with patient BMI as the key variable. We calculated wait time as the date of surgery minus the decision-to-treat date, and is reported in number of days. We calculated BMI based on measurements from the patient’s visit to the orthopedic clinic about 2 weeks before surgery. We included the following covariates: age, sex, year of surgery, hospital identifier, anonymized surgeon identifier and a measure of socioeconomic status, specifically, median neighbourhood household income from Census data.
Statistical analysis
We used univariate analysis to test for unadjusted associations between wait time and BMI, followed by multivariate linear regression analysis to control for confounders. To account for nonlinearity, we categorized BMI into 7 groups (< 20, 20–24, 25–29, 30–34, 35–39, 40–49 and ≥ 50). BMIs in the 25–29 category were considered pre-obese, and BMIs ≥ 30 were considered obese, in accordance with the World Health Organization (WHO) classification system (http://apps.who.int/bmi/index.jsp?introPage=intro_3.html). We included year of surgery, hospital, individual surgeon and patient sex as individual categorical variables; we included patient age and neighbourhood income as continuous variables. Because of the relatively few patients who had very long wait times, we performed tests for non-normality to assess for right-hand skewness. To test whether there was variation across surgeons in the association between BMI and wait time, we ran separate multivariate models for each individual surgeon.
We conducted statistical analysis using SAS 9.4. Ethics approval was granted by the Capital Health Ethics board.
Results
In general, patients experienced longer waits for TKA than THA. The mean and median wait times for knee replacement were 397 days and 276 days, respectively. For hips, the mean and median wait times were 276 days and 184 days, respectively. The mean BMI was slightly higher for knee replacement patients at 32.7, compared with 29.1 for hip replacement patients. These results show that the mean BMI for patients undergoing knee replacement was in the obese category, and the mean for hips was in the pre-obese category. The mean age was 66.1 for the TKA group and 64.7 for the THA group, and the median neighbourhood income was slightly lower in the TKA group. Table 1 shows patient characteristics.
Patient characteristics
As shown in Table 1, the modal BMI category was 25–29 (pre-obese) for both the TKA and THA groups. More females than males underwent both procedures over the period and there was a relatively even distribution over time. The same 8 surgeons (surgeons A–H) completed 87% of TKAs and 92% of THAs. Among those surgeons, however, there was variation across the distribution, as results showed 1 surgeon carried out 5.5% of TKAs and another did 20.2%. Similarly, for THAs, 1 surgeon completed 6.4% of the procedures and another did 23.5%.
The considerably larger mean wait time relative to the median wait time for both procedures suggests a right-skewed distribution. Figure 1 shows the distribution of the number of wait days for knees and hips, which also indicates non-normality due to data skewness. The Kolmogorov–Smirnov and Anderson-Darling statistical tests showed that the assumption of normality should be rejected with 95% confidence. As a result, wait times were log-transformed and log-linear regression models were run.

Distribution of wait time (in days). TKA = total knee arthroplasty, THA = total hip arthroplasty.
For TKAs, in regressions of wait time on BMI categories without including other covariates, higher BMI was associated with a longer wait time. Specifically, patients with a BMI of 35–39 had a 26% longer wait, those with a BMI of 40–49 had a 35% longer wait and those with a BMI of ≥ 50 had a 44% longer wait, compared with the reference category of 20–24.11 When control variables were added in the multivariate model, the association was smaller, yet statistical significance was maintained. With covariates, patients in the 35–39, 40–49 and ≥ 50 BMI categories had 11%, 17% and 34% longer waits, respectively (Figure 2). Univariate models for THAs showed that patients in the 30–34, 35–39 and 40–49 categories had longer wait times than those in category 20–24. Those in the highest category, however, showed no statistical difference. Multivariate results show there was no statistical difference between BMI categories once control variables were added (Figure 2).

Percentage difference in wait time by obesity category, relative to reference category (body mass index [BMI] 20–24). TKA = total knee arthroplasty, THA = total hip arthroplasty.
*Statistically significant with 95% confidence.
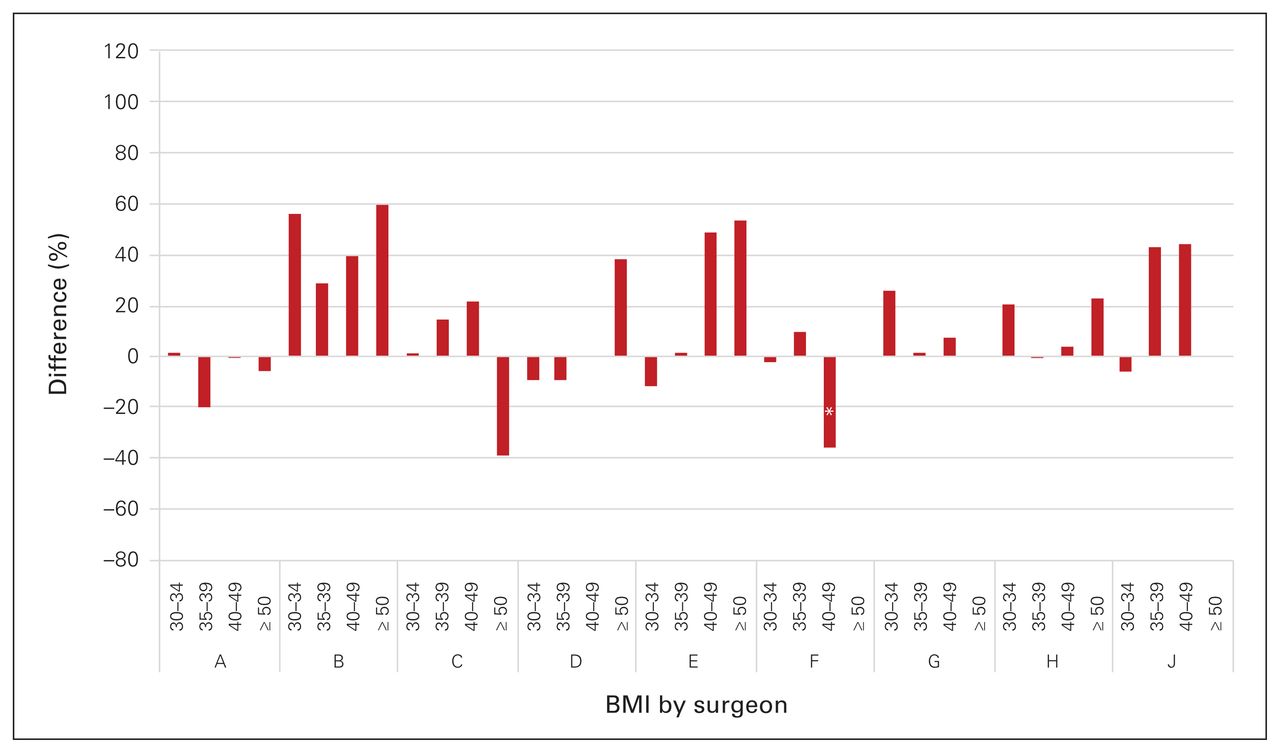
Figure 3 and Figure 4 show individual surgeon results for TKAs and THAs, respectively. Although we ran multivariate regressions, only BMI category coefficients are reported. For TKAs, results for surgeon F showed a longer wait time for patients with a BMI of ≥ 30. For example, those with a BMI of 30–34 had a 26% lengthier wait than those in the 20–24 category, and those with a BMI of ≥ 50 waited more than twice as long. There is also evidence that patients of surgeon E with a higher BMI, specifically the 40–49 category, had a longer wait. Of the remaining surgeons, patients who were obese did not have a statistically longer wait for a TKAs. For THAs, Figure 4 shows that patients who were obese did not wait longer under the care of any individual surgeon. However, patients of surgeon F with a BMI of 40–49 experienced a shorter wait than those in the 20–24 category. As shown in Figure 3 and Figure 4, for TKAs, 3 surgeons had significantly longer waits for patients in 1 or more of the obesity categories than the reference category, whereas with THAs, there were no statistical differences.

Percentage difference in wait times for total knee arthroplasty by obesity category, relative to reference category (body mass index [BMI] 20–24) and by surgeon (A–J). *Statistically significant with 95% confidence.
Note: Surgeon I has been omitted for confidentiality.
Percentage difference in wait times for total hip arthroplasty by obesity category, relative to reference category (body mass index [BMI] 20–24), and by surgeon (A–J). *Statistically significant with 95% confidence.
Note: Surgeon I has been omitted for confidentiality.
Discussion
Findings from this study suggest that patients who are obese waited longer for knee replacement surgery but not for hip replacement over the 2011–2016 period. Results for individual surgeons show that there is some variation in wait times for patients who are obese and awaiting knee surgery, with 2 of 11 surgeons showing longer waits for patients with a BMI ≥ 30. There was no indication that patients who are obese waited longer for hip replacement for any of the individual surgeons.
Reducing wait times for total joint replacement is a priority in Canada, as prolonged waits to access to care are becoming unacceptable to patients and providers. However, optimizing surgical conditions, including considerations for the patient’s health and physical condition, must be taken into account. Because additional weight is associated with an increased likelihood of surgical complications, a longer wait time may provide the patient with more time to prepare for surgery, including losing weight. It is important to educate patients about the additional risks of an elevated BMI on the development of complications after joint replacements. Furthermore, patients who are obese need considerable support in accessing effective programs for losing weight before surgery. Meaningful weight loss will take time for most patients. Therefore, individual surgeons who show longer wait times for patients in higher BMI categories may not be an undesirable finding of this study. Finally, our results also showed considerable variation in wait times across surgeons for all patients, suggesting that there may be contributing factors beyond obesity affecting delays in surgery, including the referral and assessment system.
It is interesting that there was a difference in the wait times for TKA versus THA for patients who are obese. It is not clear why THA wait times were not as affected by obesity compared with TKA. One possible explanation is that patients may tolerate an arthritic knee better than an arthritic hip and so a hip disability will motivate surgeons to provide surgical intervention. It is also possible that there is a bias against patients who are obese and awaiting TKA. The distribution of adipose tissue may make surgeons more likely to delay surgery to obtain weight loss. One of the key findings from this study is that there is clear variability in how surgeons treat patients who are obese, which can lead to confusion for both the patient and their referring physician. The development of standardized treatment plans for patients with elevated BMI will be important to ensure that they are receiving the appropriate care.
Limitations
There are several limitations in this study. First, patient height and weight information was available only at a single point in time, namely the presurgical clinic visit which would have occurred approximately 2 weeks before surgery. BMI at first surgical consultation could provide a better measure to test for the associations with wait time, although it is expected that BMI at both time points would be highly correlated. Second, clinicians assess appropriateness for surgery differently. It is possible that individual surgeons may prefer not to operate on patients who are obese, resulting in those patients finding another surgeon. Some surgeons, therefore, may show no association between BMI and wait time due to selection bias. Finally, results could be strengthened with the inclusion of controls for comorbidities that may affect wait time for some patients. Despite the limitation, the main strength of this study was the large sample size of patients, collected over the specified time period. This allowed us to identify trends and create a relative picture of how patients who are obese are being treated over time.
Conclusion
We identified that groups of patients with elevated BMI were experiencing longer waits, and that this is a variable effect of a surgeon’s practice. For patients waiting for TKAs, those who were obese were likely to experience increased waits for surgery; however, these effects were not observed for patients who were obese and awaiting THA. Ultimately, this analysis will allow for targeted efforts to standardize the wait times experienced by patients who are obese.
Footnotes
This work was presented at the Canadian Arthroplasty Society Meeting, 2018, Toronto, Ont.
Competing interests: Glen Richardson discloses consulting agreements with Stryker and KCI, a speaking honararium from DePuy Synthes and research grants from Stryker and DePuy Synthes. No other competing interests were declared.
Contributors: Chris Dusik, Lynn Lethbridge and Michael Dunbar conceived of the study and acquired the data, which Glen Richardson and Chris Dusik analyzed. All authors contributed substantially to the writing and revision of this article and approved the final version for publication.
- Accepted March 16, 2021.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.