


Abstract
Background: The Consultation and Relational Empathy (CARE) Measure, a validated questionnaire designed to assess patients’ perceptions of their physician’s communication skills and empathy, has been used to assess empathy in medical specialties but has seldom been applied to surgery. We assessed empathy and communication skills among a group of surgeons within a single academic institution.
Methods: All surgeons within our department of surgery were invited to participate. Patients seen in clinics of participating surgeons were recruited prospectively from July 2018 to February 2019. At the end of each clinical encounter, they were asked to complete a CARE survey. Surveys were analyzed according to previously validated inclusion and exclusion criteria. We calculated mean scores for each surgeon and surgical division. About 6 months after study completion, surgeons were provided with their individual score and de-identified division scores, and were asked to complete a follow-up survey assessing their attitudes toward the CARE Measure.
Results: Of the 82 surgeons invited, 51 (62%) agreed to participate; 7 had fewer than 25 completed surveys and were excluded from analysis. A total of 1801 surveys for 44 surgeons (33 male and 11 female) were included in the final analysis. The average CARE score across the department was 46.9 (95% confidence interval [CI] 46.6–47.1). Female surgeons received significantly higher scores than male surgeons (mean 47.6 [95% CI 47.1–48.0] v. 46.7 [95% CI 46.4–48.0]). Of the 35 surgeons who responded to the follow-up survey, 31 (89%) felt that the questions in the CARE Measure applied to their practice, and half of these reported that they intended to make changes in response to the feedback.
Conclusion: We found high communication and empathy scores among surgeons in the outpatient setting, with enough variability to encourage continued improvement. The CARE Measure appears to have face validity among surgeons, and the vast majority found it relevant to their practice. Further study is needed to formally assess the relevance, performance, reliability and construct validity of this measure.
The interaction between clinician and patient remains the cornerstone of medical care. In recent years, there has been increased emphasis on patient-centred care and attention paid to the patient’s perspective on their own health and wellness.1 Physician empathy and good communication skills improve both clinical and patient-reported outcomes.2,3 Empathy — the ability to understand and share the feelings of another — has become a quality that patients desire and expect from physicians.1 Physicians also benefit from improved communication skills. Errors in communication have been described as the root cause of medical malpractice claims,4 and sustained decreases in physician burnout after mindful communication training have been reported.5
The Consultation and Relational Empathy (CARE) Measure is a patient-rated measure of the interpersonal skills of health care practitioners. Initially described and validated by Mercer and colleagues,6 in 2004, this measure aimed to “provide a tool for the evaluation of the quality of consultations in terms of the ‘human’ aspects of medical care.” Those authors sought to develop a process based on a broad definition of empathy that is meaningful to patients regardless of their socioeconomic status or other confounders. The CARE Measure may be of considerable utility to many institutions, academic and community alike, seeking objective measures by which to grade their clinicians and give meaningful feedback. Its use has been described among primary care physicians and medical specialists.7 However, its use has not been well described among surgeons. We aimed to describe the pilot implementation of the CARE Measure across various divisions of our department of surgery, report and compare our findings, and assess the face validity of using the CARE Measure among surgeons.
Methods
We obtained permission from our institutional research ethics board and chief medical officer to conduct this prospective study in surgery outpatient clinics. The proposal was discussed with the quality-improvement leads from each division as well as the division and department head(s). A decision was made that individual surgeon scores would be shared only with that participating surgeon; all other data would be de-identified. Emails were sent to all surgeons in the department in July 2018 requesting voluntary participation in the study. All surgeons were treating adults; no pediatric surgeons were included in this study.
We obtained the CARE Measure survey (Appendix 1, available at www.canjsurg.ca/lookup/doi/10.1503/cjs.003721/tab-related-content) from its original source; permission was obtained for its use. The survey included evaluation of 10 discreet areas, each evaluated on a 5-point scale ranging from “poor” (1 point) to “excellent” (5 points). In addition to these standard questions, patients were asked to provide their age and gender, and indicate whether this was their first time seeing this surgeon.
The survey was conducted from July 2018 to February 2019, typically with a 4-week period of collection in each division. Nursing managers, nursing staff and ward clerks in all participating clinics were informed about the purpose of the survey. Nursing staff was specifically requested to provide surveys to all consecutive patients aged 18 years or older. Blank surveys were attached to individual patient charts after check-in with the ward clerk. Patients were not advised of the survey or its purpose before their appointment. Clinical encounters were carried out in the usual fashion; they included both consultation and follow-up visits. At the conclusion of the clinical encounter, patients were asked by nursing staff to complete the survey and submit it to the ward clerk before leaving the clinic. Patients were assured that they would remain anonymous. Informed consent for participation in the study was obtained from all participants included in the study.
We analyzed the completed surveys according to specific CARE Measure instructions. The 10 items were added, giving a maximum possible score of 50 and a minimum possible score of 10. Up to 2 “Does not apply” responses or missing values are allowable and are replaced with the average score for the remaining items. Questionnaires with more than 2 missing values or “Does not apply” responses were removed from the analysis. Surgeons who accrued fewer than 25 completed surveys were excluded from the analysis; this exclusion criterion was arrived at after discussion with the author of the CARE Measure. The total scores for each survey were input into Microsoft Excel. We calculated mean scores and 95% confidence intervals (CIs) for each surgeon and division. We used 2-sample t tests to compare CARE scores between subpopulations; a preceding 2-sample F test determined whether variance was equal between groups and dictated which t test was used.
About 6 months after study completion, we provided all participating surgeons with their mean CARE scores and corresponding percentiles, as well as de-identified division and department scores. We also provided a list of resources for improving communication and empathy available to surgeons at our hospital.
A follow-up survey (Appendix 1) regarding the utility of the CARE Measure was distributed to participating surgeons when they received their scores and at 2-week intervals after the scores were received for a total of 2 additional reminders; a reminder was also posted in the department of surgery newsletter. The survey was developed in collaboration with the scientific director of the Ottawa Hospital Research Institute Centre and their team of statisticians. It was disseminated and analyzed with Microsoft Forms.
Results
Six of 7 surgical divisions participated in the study. Of the 82 surgeons invited, 51 (62%) agreed to participate. A total of 1955 surveys were completed; the number per surgeon ranged from 4 to 55. Seven surgeons (6 general surgeons and 1 plastic surgeon with a total of 67 surveys) had fewer than 25 completed surveys and were excluded from analysis. Among the remaining 44 surgeons (33 male and 11 female), 87 surveys (4.6%) contained fewer than 8 answered questions and were excluded. Therefore, 1801 surveys for 44 surgeons were included in the final analysis (Table 1).
Frequency of responses to the Consultation and Relational Empathy Measure
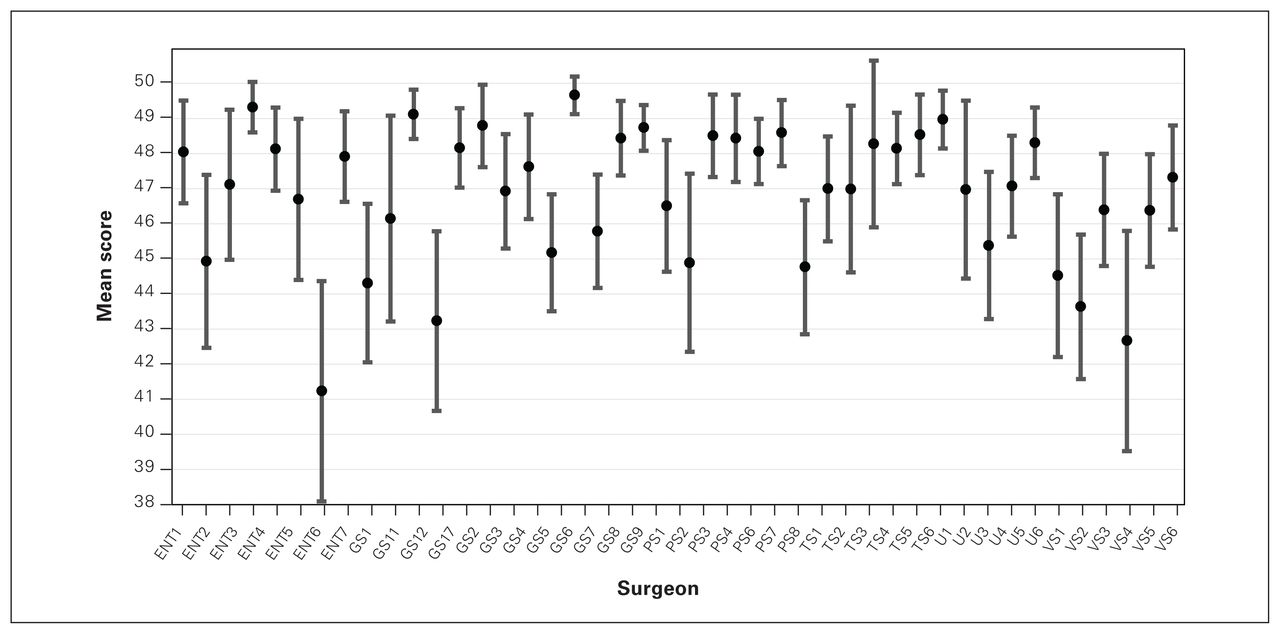
Mean CARE scores for the 44 surgeons ranged from 41.2 to 49.7 (Figure 1). The average CARE score calculated across the entire department was 46.9 (95% CI 46.6–47.1). Calculated by division, the mean CARE scores ranged from 45.3 to 47.7 (Figure 2). One-way analysis of variance showed that there were statistically significant differences between divisions (p < 0.001).
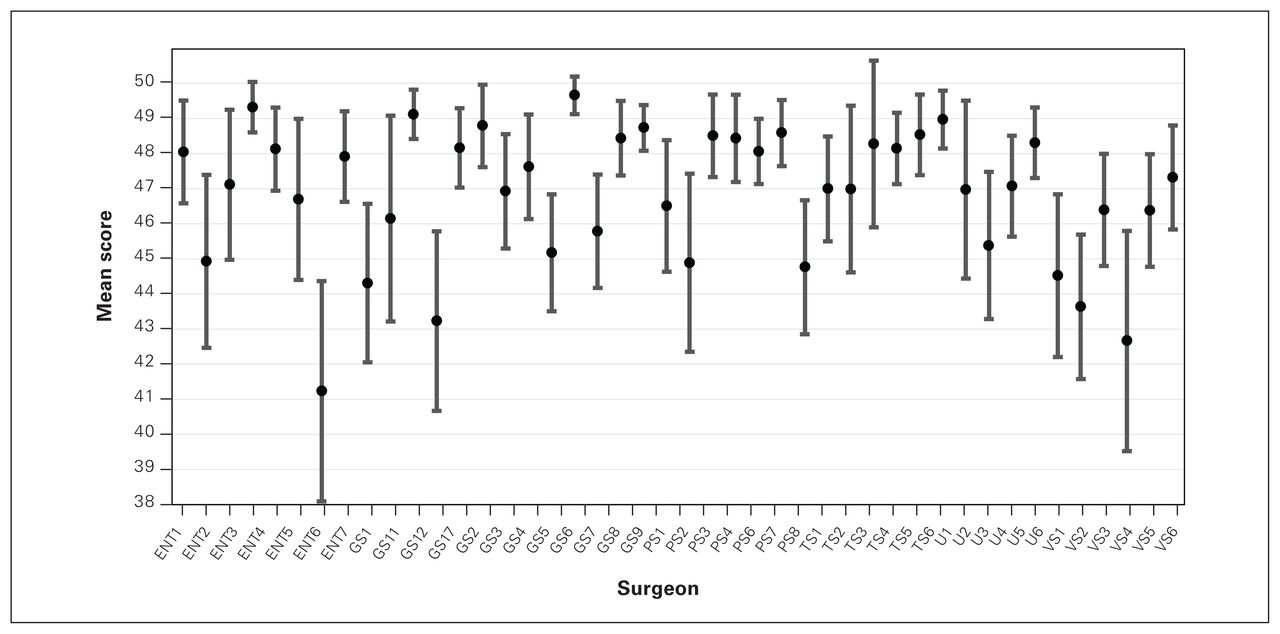
Mean Consultation and Relational Empathy Measure scores by surgeon. Error bars represent 95% confidence intervals. ENT = otolaryngology; GS = general surgery; PS = plastic surgery; TS = thoracic surgery; U = urology; VS = vascular surgery.
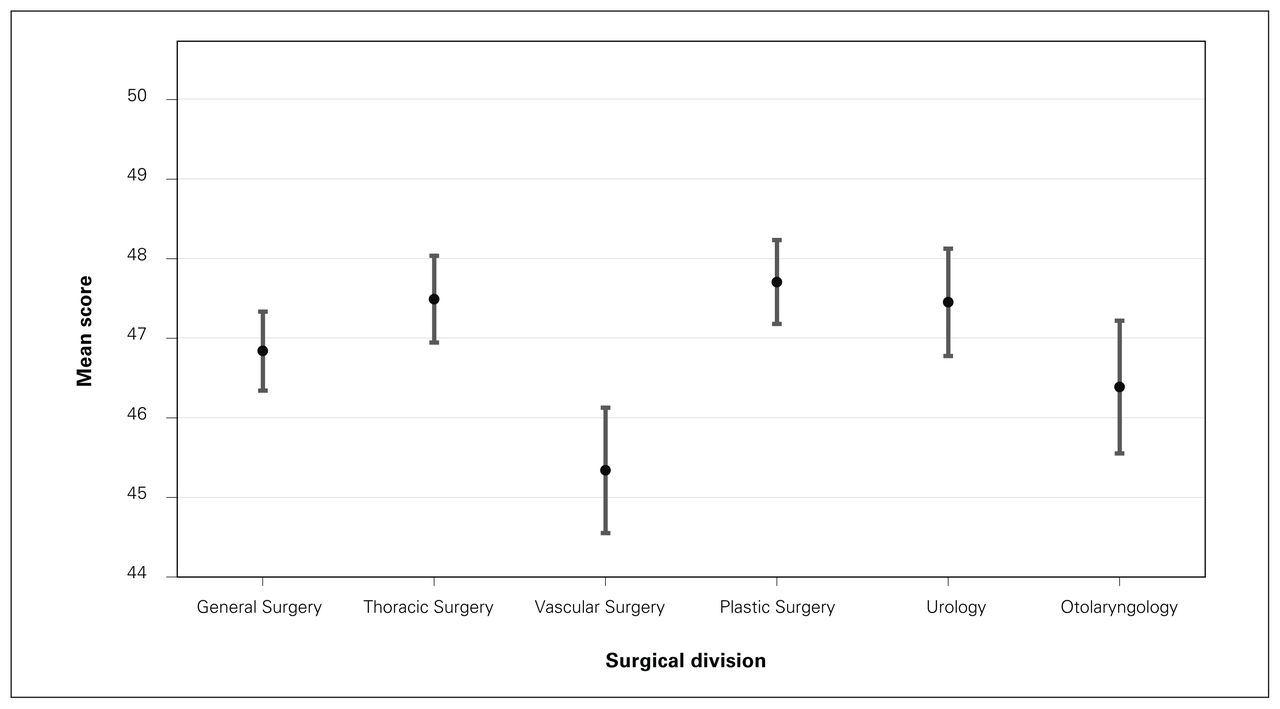
Mean Consultation and Relational Empathy Measure scores by division. Error bars represent 95% confidence intervals.
We compared CARE scores for the male and female surgeons using a 2-sample t test (Table 2). On average, female surgeons received scores 1 point higher than male surgeons (47.6 [95% CI 47.1–48.0] v. 46.7 [95% CI 46.4–48.0]). There was also a significant difference between consultations and follow-up visits, with patients at follow-up rating their surgeons higher by 1 point on average than those meeting their surgeon for the first time (47.4 [95% CI 47.1–47.7] v. 46.3 [95% CI 45.8–46.8]). There was no difference in scores assigned by male and female patients (46.9 v. 47.0, p = 0.7).
Subpopulation comparisons*
Thirty-five of the 51 surgeons responded to the follow-up survey, for a response rate of 69%. Of the 35, 31 (89%) felt that the questions included in the CARE Measure applied to their practice. They reported that the most useful item on the survey was “Making a plan of action with you,” and the least useful was “Helping you to take control” (Table 3). Twenty-four respondents (69%) felt that the feedback they received was useful to them; half of these reported that they intended to make changes in response to the feedback.
Surgeons’ responses to the follow-up survey*
Discussion
This study describes the successful implementation of the validated CARE Measure to assess empathy and communication skills in single academic surgical department. Surgeons in our department had a mean CARE score of 46.9, which is above average8 and shows that patients perceived them to have great empathy and communication skills. We observed variability among surgeon- and division-level scores, and higher scores among female surgeons than male surgeons.
Importantly, a large majority of surgeons found the assessment applicable and useful to their practice, and 34% planned on making changes based on participation in this intervention. In contrast, a 2017 review of 64 independent CARE studies showed that the average physician score was 39.68.7 All divisions in our study had a higher average CARE score than this. Compared to normative values published by the creators of the CARE Measure,8 our department scored in the 90th percentile overall, with the lowest-scoring division still in the 70th percentile.
We found 2 prior studies in which the CARE Measure was applied in a surgical setting. Steinhausen and colleagues2 compared assessments by 120 patients who had undergone trauma surgery of their physician’s empathy (using the CARE Measure) to their assessment of medical treatment outcome (using the Cologne Patient Questionnaire). They found that patients who rated their physician’s empathy higher tended to rate their medical outcome better. They reported an average CARE score of 38.0 (standard deviation [SD] 9.75). However, they did not report the number of surgeons assessed or individual surgeon scores. Dekker and colleagues9 compared 6 orthopedic surgeons’ self-assessment of their own empathy with their patients’ assessment using the CARE Measure and found that the two do not necessarily correlate. The average CARE score overall was 47 (SD 5); individual surgeon’s CARE scores were not reported.
To our knowledge, our study is the first to describe the logistics of implementing the CARE Measure in surgical clinics, the results of the measure at the surgeon, division and department level, and the attitudes of surgeons toward the measure. Several authors have suggested that surgeons have different personality types from their colleagues in medical specialties. Surgeons are at times portrayed as exhibiting ambition, leadership and guile, but often lacking in compassion, empathy and communication skills.10–13 Some authors have made direct comparisons, reporting that medical specialists have greater levels of empathy than surgeons.14,15 The present study refutes those findings, showing high communication and empathy scores across multiple surgical specialties. The cause of this discrepancy is not clear. Studies that directly compare patient satisfaction with communication skills between surgical and medical or primary care encounters are lacking; they should be performed to better understand the differences observed. White and colleagues16 performed an analysis of the structure of communication between surgeons and patients in the outpatient clinical setting and found that it differs from that in primary care encounters in subtle but important ways. Specifically, surgical encounters are unique in that they tend to start with establishing a mutual understanding of the referral and achieving alignment of goals between the surgeon and patient. This may explain some portion of the discrepancy in communication and empathy scores between our study and other reports.
We noted a statistically significant difference in CARE scores between male and female surgeons, with females scoring higher than males by about 1 point. However, it is difficult to assess whether this difference was perceptible by patients. The minimal clinically important difference has not been studied for the CARE Measure. It remains unclear whether this represents a true difference in male and female empathy, or a gender-based difference in empathy perceived by patients. In any case, this finding is consistently borne out in the literature. The review of 64 independent CARE studies, for example, showed that the 6 studies with a majority (> 50%) of female practitioners showed mean empathy scores that were 16% higher than those of the 6 studies with a majority of male practitioners (42.77 v. 34.85).7 This difference in empathy has been described in numerous other sociologic, psychologic, behavioural and neurodevelopmental studies.17
The finding that patients seeing their surgeon for a follow-up visit rated them higher, by 1 point on average, than those meeting their surgeon for an initial consultation was unexpected, as consultation visits typically last longer than follow-up visits and involve more in-depth discussion of diagnosis, treatment and prognosis. One possible explanation is that patients have higher expectations for initial visits than for follow-up visits, which are not entirely met. Alternatively, patients in follow-up are more familiar with their surgeon and may be more likely to score them higher. Another explanation is that consultations are often initially performed by a fellow, resident or medical student, who then reviews with the attending surgeon before the surgeon sees the patient to review the plan and answer any questions. Our instructions to the patients were to complete the survey based only on their interaction with the attending surgeon, not with the fellow or resident. As such, their interaction with the surgeon may be relatively brief and unsatisfying. This finding suggests that surgeons may want to allocate more time to new consultations.
The assessment and training of physician empathy has important consequences. Breakdowns in communication are a major cause of malpractice litigation in the United States, Canada and elsewhere.18–20 A recent review by Shouhed and colleagues21 suggests an inverse relation between a surgeon’s emotional intelligence — defined as his or her ability to monitor and regulate his or her emotions as well as the emotions of others — and litigation rates. Other investigators have shown that communication training for physicians leads to improved patient satisfaction.22 This underscores the importance of assessing and teaching these skills like any other medical or surgical technique. Although most surgeons are extremely committed to the care of their patients, there appear to have been minimal efforts made to objectively measure surgeons’ empathy as judged by their patients.
Our results may provide valuable insights into the applicability of the CARE Measure in surgical practice. One finding was that surgeons and patients alike agreed that item 9 (“Helping you to take control”) was not particularly suitable: when asked which item was least useful, surgeons selected this question most frequently, and it received the greatest number of “Does not apply” responses by patients. Interestingly, this directly mirrors the findings of Mercer and Murphy23 in a study of CARE Measure validity in a secondary care population, where they also found the highest “Does not apply” rate (9.1%) for question 9. Perhaps this finding reflects the nature of surgical treatments, where patients often relinquish control to their surgeons.
A large majority of surgeons (69%) in the present study felt that the feedback they received was useful to them, and half of these reported that they intended to make changes in response to the feedback. As such, we appear to have demonstrated face validity of the CARE Measure in this population. We plan to readminister the study to assess for changes in our results and to formally assess relevance, performance, reliability and construct validity. We are also exploring hospital-wide implementation of the CARE Measure in all departments.
Limitations
One of the strengths of this study is the size of the data set. To our knowledge, only 2 prior studies collected more than 1801 responses: Mercer and colleagues24 used 3044 surveys to evaluate 26 general practitioners, and Price and colleagues25 used 2550 surveys to evaluate 36 general practitioners. Our study is therefore the largest evaluation by number of physicians assessed using the CARE Measure and certainly the largest such study of surgeons.7 This allowed us to form precise estimates of mean scores with narrow CIs and revealed statistically significant differences within the data.
A limitation of this study is the shared care of patients at an academic centre, with surgeons and learners both participating in clinics. This shared responsibility may result in surgeons’ spending less time with the patient in an absolute sense than they would otherwise. Conversely, patients may perceive that they have received more time with the team overall. The score a surgeon receives could also be biased by the quality of the interaction that a resident has with a patient. Studies have shown that, in both surgical and medical settings, patients who are seen by residents are less satisfied than those who see only the attending physician.26,27 Another limitation is that there may be contamination bias when comparing consultation and follow-up visits: the same patient may contribute to both, first during a consultation visit, then again in follow-up. This was impossible to mitigate given the anonymized nature of our data collection, but since the surveys were carried out over a relatively short time in each division, this bias is likely not substantial. In addition, the study design may have resulted in sampling bias in that patients with a positive interaction (are candidates for surgery, have a plan in place) may have been more likely than those with a negative interaction to complete the survey.
Conclusion
We have demonstrated the successful implementation of the CARE measure in an academic surgical department. Our results are encouraging, showing relatively high communication and empathy scores. In addition, our data show significant gender, surgeon-to-surgeon and division-todivision variation. This is also encouraging, as it indicates room for continuing improvement and makes a strong case for the utility of this measure for tracking changes in care over time. The CARE Measure also appears to be valid in a surgical setting, as many surgeons found it useful and reported that they intended to implement changes based on their results. Further study is needed to formally assess the relevance, performance, reliability and construct validity of the CARE Measure.
Footnotes
Competing interests: Nadia Khan is cochair of the Canadian Association of General Surgeons Resident Committee. Neal Rowe reports funding from AMT Surgical for travel to an educational course. He is a board member of the Canadian Urological Association and the Urologic Society for Transplantation and Renal Surgery. No other competing interests were declared.
Contributors: H. Moloo, A. Neville and M. Momtazi designed the study. E. Hopkins, N. Khan, R. Gilbert, D. Kubelik, N. Rowe and M. Odell acquired the data, which O. Solaja and D. Maziak analyzed. O. Solaja and H. Moloo wrote the manuscript, which E. Hopkins, N. Khan, R. Gilbert, A. Neville, D. Kubelik, D. Maziak, N. Rowe, M. Odell and M. Momtazi critically revised. All authors gave final approval of the article to be published.
- Accepted March 14, 2022.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See:https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue

{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.