


Abstract
Background: It has recently been reported that mismatch repair (MMR) status and microsatellite instability (MSI) status in gastroesophageal carcinomas predict surgical, chemotherapeutic and immunotherapeutic outcomes; however, there is extensive variability in the reported incidence and clinical implications of MMR/MSI status in gastroesophaegal adenocarcinomas. We characterized a Canadian surgical patient cohort with respect to MMR status, clinicopathologic correlates and anatomic tumour location.
Methods: We investigated MMR and BRAF V600E status of gastroesophaegal adenocarcinomas in patients who underwent gastrectomy or esophagectomy with extended (D2) lymphadenectomy at a single centre between 2011 and 2019. We correlated patterns of MMR expression in the overall cohort and in anatomic location–defined subgroups with treatment response and overall survival using multivariate analysis.
Results: In all, 226 cases of gastroesophaegal adenocarcinoma (63 esophageal, 98 gastroesophageal junctional and 65 gastric) were included. The MMR-deficient (dMMR) immunophenotype was found in 28 tumours (12.3%) (15 junctional [15.3%], 13 gastric [20.0%] and none of the esophageal). The majority (25 [89%]) of dMMR cases showed MLH1/PMS2 loss without concurrent BRAF V600E mutation. Two MSH2/ MSH6-deficient gastric tumours and 1 MSH6-deficient junctional tumour were detected. The pathologic response to preoperative chemotherapy was comparable in the dMMR and MMR-proficient (pMMR) cohorts. However, dMMR status was associated with significantly longer median overall survival than pMMR status (5.8 yr v. 2.4 yr, hazard ratio [HR] 1.91, 95% confidence interval [CI] 1.06–3.46), particularly in junctional tumours (4.6 yr v. 1.9 yr, HR 2.97, 95% CI 1.27–6.94).
Conclusion: Our study shows that MMR status has at least prognostic value, which supports the need for biomarker testing in gastroesophageal adenocarcinomas, including junctional adenocarcinomas. This highlights the clinical significance of determining the MMR status in all adenocarcinomas of the upper gastrointestinal tract. Response to induction chemotherapy, however, was not influenced by MMR status.
Upper gastrointestinal malignant diseases represent close to 9% of all new cancer cases and 14% of all cancer deaths worldwide.1 Of their 2 main histologic subtypes, squamous cell carcinoma and adenocarcinoma, the latter predominates among tumours of the distal esophagus, the gastroesophageal junction (GEJ) and the proximal stomach, and continues to rise in incidence, particularly in high-income countries.2–4 Emerging mutational analysis data show that adenocarcinomas of the distal esophagus and proximal stomach are genomically indistinguishable and thus should be considered as 1 disease — gastroesophageal adenocarcinoma — and treated similarly.5 A 2014 study by the Cancer Genome Atlas Research Network showed that, in order to improve therapy response and survival, treatment protocols need to take tumour genetic and molecular profiles into account.6 Molecular characterization of gastric adenocarcinomas yielded several distinct subtypes, including a subset deficient for DNA mismatch repair (MMR). This deficiency results in microsatellite instability (MSI) and the development of hundreds to thousands of somatic mutations in MSI-high (MSI-H) tumours.7,8
There is substantial variability in the reported incidence of the MMR phenotype, ranging from about 5% to 30% in gastric cancers, and from 0% to 8% in esophageal and junctional cancers.8–11 This variability is at least partially explained by intercountry variability, which highlights the importance of expanding the geographic distribution of data collection. Most contemporary series have focused on Eastern Asian and European populations,10 with North American patients remaining largely underrepresented.
It is becoming increasingly important to obtain MMR status for clinical and surgical decision-making. Post hoc analyses of 2 large randomized studies examining platinum-based chemotherapy in the neoadjuvant (Medical Research Council Adjuvant Gastric Infusional Chemotherapy [MAGIC] trial12) and adjuvant (Capecitabine and Oxaliplatin Adjuvant Study in Stomach Cancer [CLASSIC] study13) settings in gastric carcinomas suggest that patients with MSI-H tumours have better survival than those with micro-satellite stable tumours but experience no benefit, or even negative effects, from chemotherapy.14–16 In 2017, the immune checkpoint inhibitor pembrolizumab was approved for treatment of MSI-H/MMR-deficient (dMMR) unresectable gastroesophageal adenocarcinoma based on demonstration of overall response rates of about 55% in patients with MSI-H tumours.17–19 Despite these seminal advances, literature on the impact of MMR/MSI status on prognosis, its association with chemoresistance, and the impact on surgical, chemotherapeutic and immunotherapeutic outcomes remains scarce, particularly for esophageal/junctional cancers. The objectives of this work were thus to establish the proportion of dMMR tumours in a Canadian surgical cohort and to evaluate the clinical relevance of this biomarker.
Methods
Study population
This single-centre study included patients with adenocarcinoma of the esophagus (Siewert classification type 1), GEJ (Siewert classification type 2) or subcardial stomach (Siewert classification type 3) who underwent gastrectomy or esophagectomy with extended (D2) lymphadenectomy between 2011 and 2019 at the Montreal General Hospital of the McGill University Health Centre, a high-volume referral centre for upper gastrointestinal malignant diseases in Montréal, Quebec. The main exclusion criteria were histologic subtype (squamous cell carcinoma) and absence or unavailability of tumoral tissue for analysis, including no residual tumour tissue on surgical resection (complete pathologic response). Patient demographic characteristics, tumour characteristics, treatment details, operative variables and survival data were collected from electronic medical records.
The study protocol was approved by the McGill University Health Centre Institutional Review Board (2019-4965; 2021-6906), and all procedures involving human participants were performed in accordance with the 1964 Helsinki declaration and its later amendments. All patients gave informed and written consent before enrolment.
Preoperative treatment
Neoadjuvant chemotherapy was used in the majority of patients with stage 3 disease and those with stage 2 disease at high risk. The predominant regimen used consisted of a docetaxel-based triplet (DCF [docetaxel, cisplatin, 5-fluorouracil] or FLOT [docetaxel, oxaliplatin, 5-fluorouracil, leucovorin]), initially based on a local phase 2 investigator-initiated trial20 and subsequently on the FLOT4 trial.21 Chemoradiation (ChemoRadiotherapy for Oesophageal cancer followed by Surgery Study [CROSS] protocol22) was administered in a small minority of cases.
Surgical technique
The surgical approach for tumour resection was selected according to tumour localization and patients’ characteristics. Patients with esophageal or junctional tumours underwent Ivor–Lewis, McKeown or left thoracoabdominal en bloc esophagectomy, and those with subcardial tumours underwent total or subtotal gastrectomy. Extended lymphadenectomy was performed in all cases. Minimally invasive approaches were used according to surgeon preference.
Tumour staging and evaluation of treatment response
Staging was performed according to the AJCC Cancer Staging Manual.23,24 Tumour anatomic location was confirmed according to the definitions in the 8th edition of the manual, with GEJ tumours defined as lesions with the epicentre located within 2 cm of proximal stomach and extending into the GEJ for all cases reported after 2017.24 We reclassified all tumours reported before or during 2017 using 8th edition AJCC criteria when sufficient information was available. Response to neoadjuvant therapy was determined histologically on the resected specimens and graded with the Modified Ryan Scheme for Tumor Regression Score.25 Classifications were as follows: 0 (complete response) = no viable cancer cells; 1 (near-complete response) = single cells or rare small groups of cancer cells; 2 (partial response) = residual cancer with evident tumour regression, but more than single cells or rare small groups of cancer cells; and 3 (poor or no response) = extensive residual cancer. For the purpose of this study, patients with a score of 0 or 1 were classified as good responders, and those with a score of 2 or 3 as poor responders.
Tissue microarray construction
Tissue microarrays (TMAs) were constructed with tissue from primary tumour, lymph node metastases, distant metastases, intestinal metaplasia and nonneoplastic tissue, depending on tissue availability. For all TMAs, tumoural tissue duplicate cores (1 mm) were punched from each region. Tissue microarray paraffin-embedded tissue blocks were prepared with the TMA Grand Master (3DHISTECH) at the Rosalind and Morris Goodman Cancer Research Centre, McGill University.
Mismatch repair status determination and BRAF V600E mutation analysis
Immunohistochemical analysis for MMR status was carried out on 3-μm sections prepared from TMA blocks and subjected to immunohistochemistry for the mutL homologue 1 (MLH1; G168-15, Roche Diagnostics), mutS homologue 2 (MSH2; G219-1129, Roche Diagnostics), mutS homologue 6 (MSH6; SP93, Roche Diagnostics) and postmeiotic segregation increased 1 homologue 2 (PMS2; A16-4, Roche Diagnostics) with the Ventana Benchmark Ultra (Roche Diagnostics). We defined dMMR as complete absence of nuclear staining with 1 or more of the 4 antibodies in the tumoural cells in the presence of positive internal control (nuclei of lymphocytes and stromal cells). BRAF mutation status was assessed by immunohistochemistry with anti-V600E-mutant-BRAF antibody (VE1, Roche Diagnostics). Positive results were defined as granular cytoplasmic staining of the tumoural cells.
Statistical analysis
We compared clinical variables, including demographic characteristics, tumour characteristics, treatment response and survival data, among patients with dMMR tumours and those with MMR-proficient (pMMR) tumours. We calculated overall survival from the time of diagnosis to death or the time of the last recorded contact before statistical analysis, using the Kaplan–Meier method and Cox proportional hazards regression. Data were presented as mean and standard deviation or 95% confidence interval (CI). Linear mixed-effects analysis was first conducted as a bivariable analysis, followed by multivariable analysis. We adjusted multiple comparisons using Tukey post hoc tests. Statistical significance was set at p < 0.05. We performed all statistical analysis using R v.3.4.1 software (R Foundation for Statistical Computing) at a CI of 95%.
Results
Clinicopathologic parameters and dMMR status in the overall cohort
A total of 226 patients (175 men [77.4%] and 51 women [22.6%] with a mean age of 68 yr) with gastroesophageal adenocarcinomas present on surgical resection specimens were included in the study (Table 1). Neoadjuvant therapy was administered in 153 cases (67.7%) (chemotherapy in 146 cases [64.6%], chemoradiation in 7 [3.1%]). No patients were known to have germline MMR gene mutations or a family history of Lynch syndrome.
Clinicopathologic characteristics of patients with adenocarcinoma of the upper gastrointestinal tract who underwent gastrectomy or esophagectomy with extended (D2) lymphadenectomy
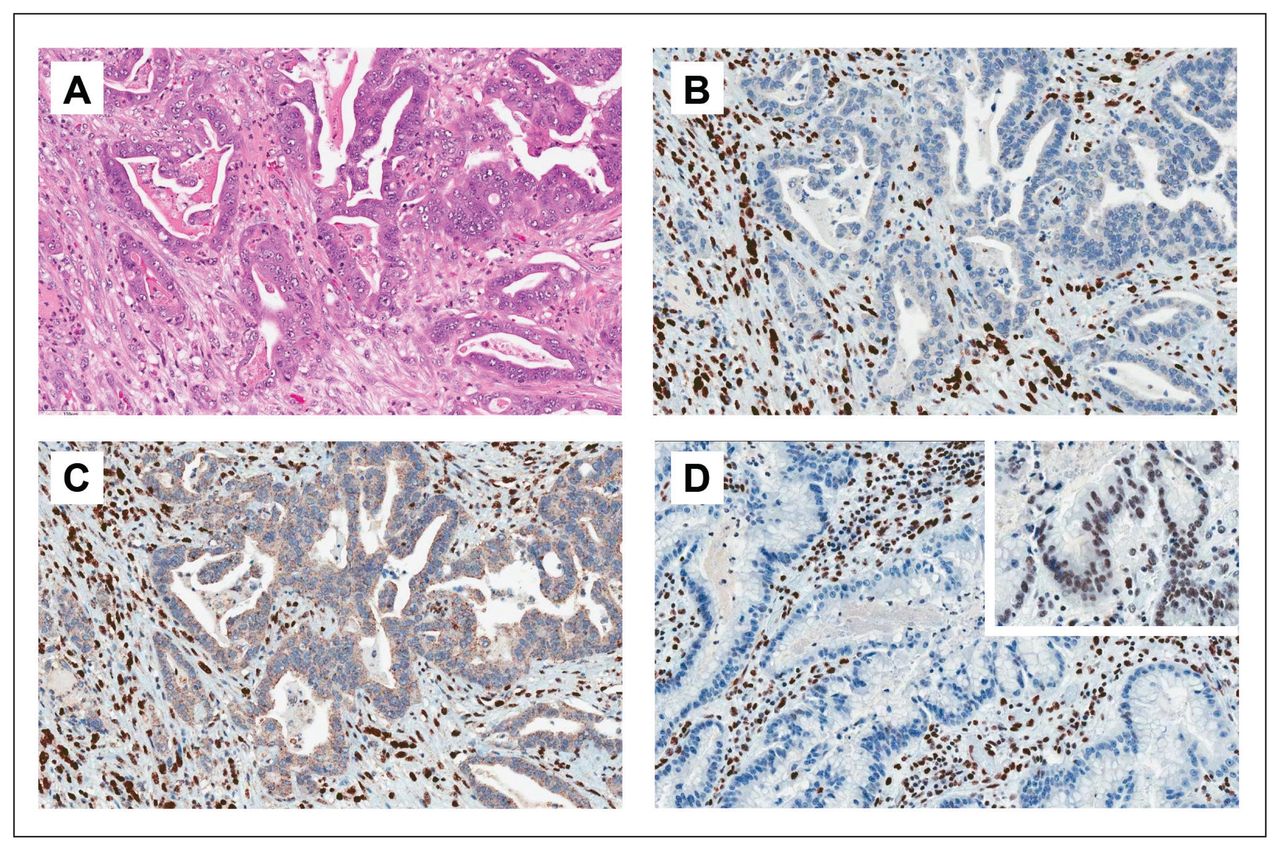
Immunohistochemical analysis of patient TMAs showed that 28 patients (12.4%) had dMMR tumours. Tissue microarray immunohistochemistry results were confirmed on full sections of the patients’ respective tumour blocks. The sections showed diffuse MMR protein loss in all cases. A total of 25 tumours showed a combined loss of MLH1/ PMS2 proteins (Figure 1A–C). The 3 remaining dMMR cases consisted of 2 subcardial tumours with MSH2/MSH6 loss and 1 MSH6-deficient junctional tumour (Figure 1D). Anti-BRAF V600E analysis showed presence of the mutation in 1 patient (0.4%) with pMMR status (Appendix 1, Supplementary Figure S1, available at www.canjsurg.ca/lookup/doi/10.1503/cjs.017021/tab-related-content). None of the patients with dMMR tumours had a BRAF V600E mutation on immunohistochemical analysis.
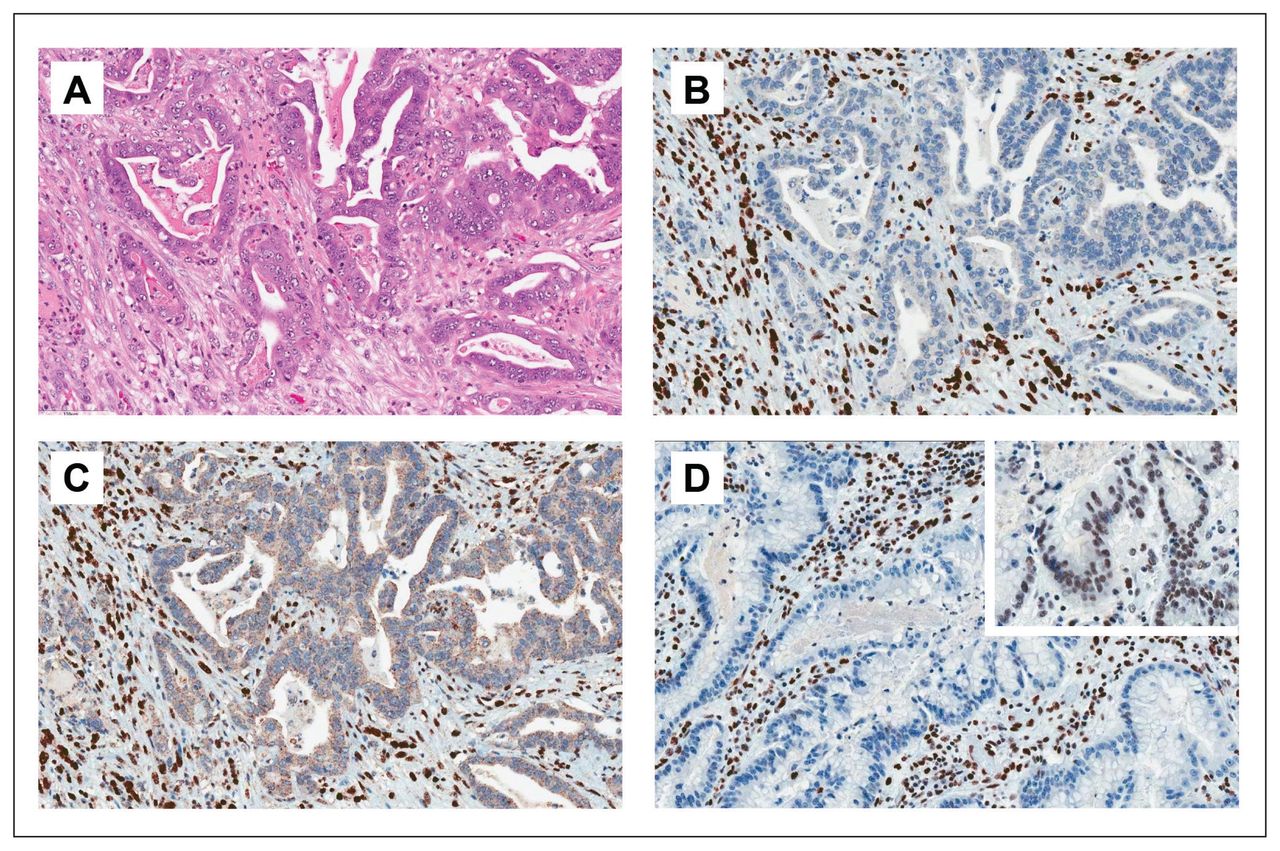
Variable combinations of patterns of loss of mismatch repair (MMR) protein in upper gastrointestinal tract malignant tumours. (A–C) Most MMR-deficient cases exhibited intestinal-type morphology (A, hematoxylin–eosin, 200×), nuclear loss of MLH1 (B, immunohistochemical staining for MLH1, 200×) and nuclear loss of PMS2 (C, immunohistochemical staining for PMS2, 200×) in the presence of appropriately staining lymphocytes. (D) A single case of MSH6 loss (immunohistochemical staining for MSH6, 200×) with intact MSH2 expression (inset, immunohistochemical staining for MSH2, 200×) was identified.
The mean age was significantly different between the pMMR and dMMR cohorts (Table 1). There did not seem to be any sex difference. Only adenocarcinomas of the GEJ (15/98 [15%]) and stomach (13/65 [20%]) showed dMMR; none of the 63 adenocarcinomas of the distal esophagus showed this phenotype. There was no difference in dMMR status between early-stage disease (stage I–II) and locally advanced disease (stage III) (p = 0.9). Retrospectively, dMMR status did not influence the choice of neoadjuvant therapy or surgery.
The dMMR phenotype was not associated with differences in tumour grade (p = 0.2). However, the dMMR immunophenotype was associated with less advanced pathologic staging compared to pMMR: dMMR was associated with lower stages and pMMR with higher stages (p = 0.01). This was reflected in nodal status: patients with pMMR tumours had a significantly greater overall median number of positive lymph nodes than patients with DMMR tumours (p = 0.02), which translated to significantly higher pathologic lymph node status staging groups in the pMMR group (p = 0.03).
Postoperative and long-term survival in the overall cohort
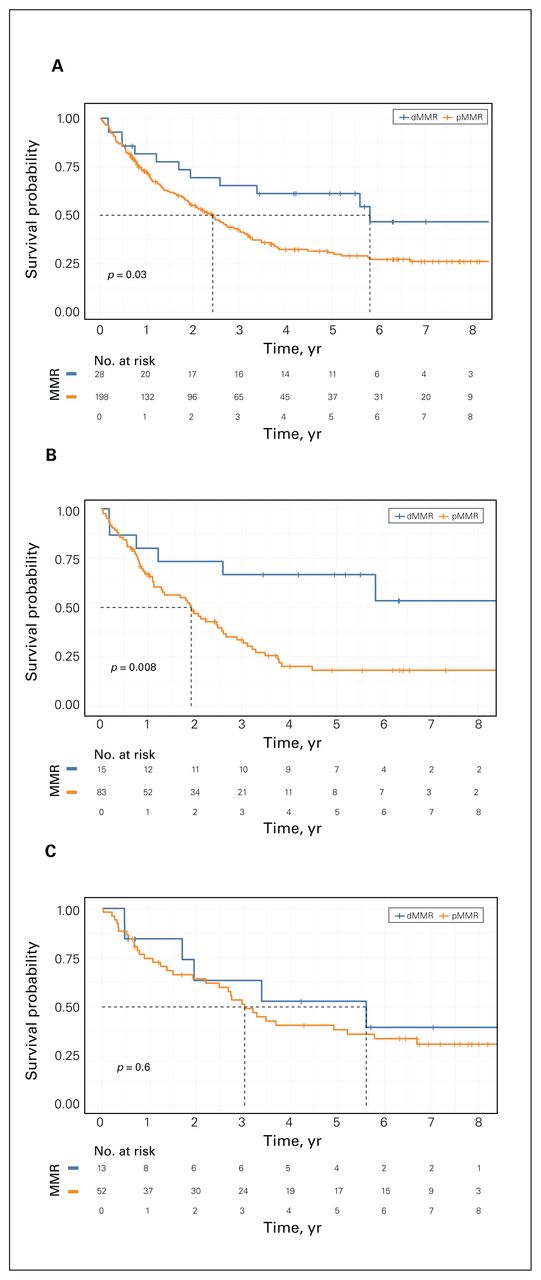
The 90-day mortality rate for the study cohort was 8.0%. It was comparable between the dMMR group (3 patients [10.7%]) and the pMMR group (15 patients [7.6%]) (p = 0.3). However, the dMMR immunophenotype was significantly and independently associated with better long-term survival than the pMMR phenotype (median overall survival 5.8 yr v. 2.4 yr, hazard ratio [HR] 1.91, 95% CI 1.06–3.46) (Table 1, Figure 2 and Appendix 1, Supplemental Figure S2).
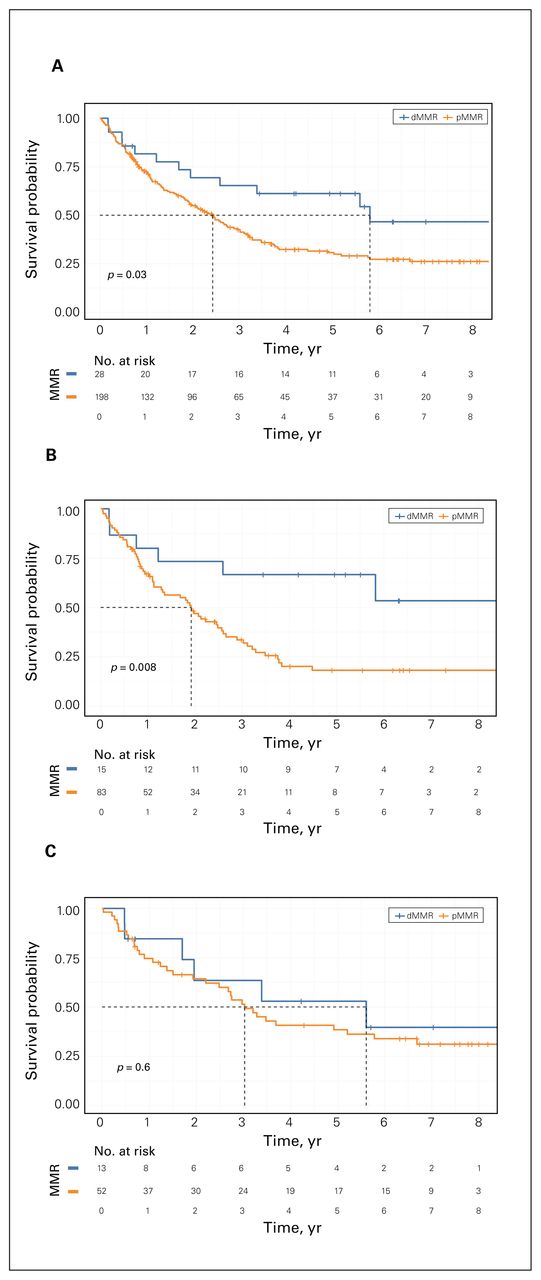
Median overall survival after diagnosis in the overall cohort (A), in patients with junctional tumours (B) and in patients with gastric tumours (C), comparing the prognosis of patients with mismatch repair-deficient (dMMR) tumours and those with mismatch repair-proficient (pMMR) tumours.
Treatment response in the overall cohort
A total of 153 patients (67.7%) had received neoadjuvant therapy. There was no difference between the dMMR and pMMR groups in receipt of neoadjuvant therapy (16 [57.1%] v. 137 [69.2%], p = 0.4). Tumour regression scoring was available for 130 (85.0%) of these patients. Among the 118 pMMR cases, pathologic near-complete response was observed in 8 patients (6.8%), partial response in 37 (31.4%) and poor response in 73 (61.9%). None of the 12 patients with dMMR tumours showed a near-complete histologic response, 4 (33%) showed a partial response, and 8 (67%) showed a poor response. Although the absence of a near-complete response in the dMMR group was notable, there was no statistically significant difference between the 2 groups.
Substratification by anatomic site
The cohort was classified based on tumour location into a GEJ group and a gastric group (Table 2). Since no dMMR cases were observed in the esophageal group, this set was excluded from site-specific differential analyses.
Clinicopathologic characteristics substratified by tumour location
The GEJ group consisted of 98 patients, 15 of whom (15%) had dMMR tumours (Table 2). The dMMR immunophenotype was associated with slightly but significantly older age (p = 0.02); there was no difference in sex distribution (p = 0.7). Similarly, although the dMMR immunophenotype was comparable to the pMMR immunophenotype with respect to clinical stages (p = 0.09), the former was associated with lower pathologic stages (p = 0.04), lower median number of positive lymph nodes (p = 0.005) and higher proportion of node-negative tumours (p = 0.008). As in the overall cohort, dMMR status was associated with longer median overall survival than pMMR status (4.6 yr v. 1.9 yr, HR 2.97, 95% CI 1.27–6.94), despite no significant difference in treatment response between the 2 groups (66 cases with available tumour regression scores) (Table 3 and Appendix 1, Supplemental Figure S2).
Treatment response substratified by tumour location
The gastric group (65 patients) had 13 dMMR cases (20%). There was a nonsignificant trend toward older age in the patients with dMMR tumours, but no difference for sex. Similarly, there was no significant difference between the dMMR and pMMR phenotypes in clinical and pathologic staging, nodal status, survival data or treatment response.
Discussion
To investigate the distribution of MMR deficiency/MSI and its associated clinical outcomes in North American surgical patients with upper gastrointestinal tract malignant tumours, we used immunohistochemical analysis to screen 226 gastroesophageal tumours for integrity of MMR protein expression. We found MMR deficiency in 12.4% of cases (28/226) in the overall cohort, with 15.3% (15/98) in the GEJ group, 20.0% (13/65) in the gastric group and none in the esophageal group. Although the results observed in the gastric cohort were within the previously published range, the rate of dMMR immunophenotype in the GEJ tumours was higher than the previously reported rate of 0%–8%.8–11 Most important, our study showed that the dMMR immunophenotype was predictive of longer median overall survival in the overall cohort, independent of clinical staging or chemo(radio)therapy response. These results validate the growing literature showing the association between dMMR/MSI-H status and positive outcome in upper gastrointestinal tract cancer. Furthermore, our study shows that this association is recapitulated when evaluating the GEJ group independently. These findings highlight the importance of determining the MMR status in junctional lesions and its value in prognostication of these tumours. Given the absence of dMMR cases in the esophageal group in our cohort and in previous studies,5,9,11 systemic MMR testing in adenocarcinomas of the esophagus appears unwarranted at present.
Although a growing body of literature has focused on clinicopathologic correlates of dMMR/MSI-H gastric adenocarcinomas, the data specific to esophageal/junctional tumours remain sparse. In our study, the dMMR immunophenotype was associated with increased age, lower pathologic staging and node-negative tumours. Our results are in line with the clinical correlates described in gastric carcinomas and corroborated in a meta-analysis.10 In our data set, the dMMR gastric tumours recapitulated the trends seen in the overall cohort, although without achieving statistical significance, possibly owing to a smaller sample.
Several studies have likewise outlined the predictive value of MMR status, both in colorectal adenocarcinomas and, increasingly, in their gastroesophageal counterparts. The dMMR/MSI-H carcinomas have been shown to be associated with no benefit and, in some instances, a negative effect of chemotherapy.14–16 In contrast to the findings reported by Smyth and colleagues15 in the post hoc analysis of the MAGIC trial, there was no difference in overall response rates to neoadjuvant chemotherapy in dMMR and pMMR tumours in our cohort. This difference may be related to our study design: since our analysis was carried out on resection specimens, cases with complete pathologic response were invariably excluded. Other factors explaining the difference include the distinct chemotherapy regimens used and cohort size. Although the regimen in both the MAGIC trial and our study included fluorouracil, we additionally used taxane-containing compounds. Better understanding of regimen-specific therapy response and toxicity profiles in upper gastrointestinal dMMR carcinomas is critical, particularly since this immunophenotype is more prevalent in older patients, who are more likely to present with other comorbidities. Omitting chemotherapy in locally advanced dMMR/MSI-H gastroesophageal adenocarcinoma, as has been considered by some authors,15,16 may be premature; our data do not support this notion, as some response to chemotherapy was seen in this cohort of patients. Chemoresponsiveness in these tumours requires further, prospective investigation with larger dMMR cohorts. The recent addition of immune checkpoint inhibitors such as pembrolizumab19 to the therapeutic arsenal for upper gastrointestinal tract carcinomas can open new therapeutic alternatives for a carefully selected population of patients. The option of neoadjuvant immunotherapy for patients with resectable dMMR tumours needs to be further investigated.
The predominant immunophenotype seen in our study was the combined loss of MLH1 staining and PMS2. In colorectal adenocarcinomas, this pattern of MMR deficiency is seen predominantly in sporadic carcinomas and is strongly associated with BRAF V600E mutation in the context of the classic hypermethylation pathway of carcinogenesis.26–28 Interestingly, however, this mutation is strikingly absent in MLH1-deficient gastric carcinoma6 and in upper gastrointestinal tract carcinomas overall.29 The absence of the classic BRAF alteration was also seen in junctional dMMR tumours in our study, which suggests an alternative mechanism of MLH1 loss in all upper gastrointestinal tract carcinomas. Non-V600E BRAF alterations such as codon 594-mutated and 596-mutated variants have rarely been described in colorectal adenocarcinomas.30,31 However, to our knowledge, no significant association between these mutations and MSI has been reported, which decreases the likelihood of their involvement in upper gastrointestinal tract tumours. Although a single BRAF V600E-positive case of pMMR GEJ adenocarcinoma was identified in our cohort, the biologic significance of this alteration remains to be determined, and systematic screening of upper gastrointestinal tract carcinomas appears to be unjustified given the currently available literature. On the other hand, 3 cases in our cohort showed a pattern of MMR deficiency that would be strongly suggestive of Lynch syndrome in a colorectal setting. Further molecular characterization of our cohort and study of additional upper gastrointestinal tract tumours are required to better understand the mechanistic basis and genetic underpinnings of MMR deficiency in upper gastrointestinal tract carcinomas.
Similarly, further studies are needed to expand our understanding of the link between MMR deficiency/MSI and improved survival. It is widely accepted in the setting of colorectal dMMR carcinomas, and increasingly in their gastric counterparts, that a dysfunctional MMR system results in an increased tumour mutational burden and, consequently, increased tumour immunogenicity.6,18,32,33 Accordingly, both colorectal and gastric dMMR/MSI-H tumours have been shown to induce a prominent adaptive immune reaction, as evidenced by the presence of tumourinfiltrating cytotoxic lymphocytes.34–37 In colorectal carcinoma, this immune phenomenon has been shown to explain at least in part the positive clinical outcome.34,35 Although the focus of our study was not mechanistic, it is reasonable to suspect that similar interplay between tumour immunogenicity and host response plays a critical role in the clinical outcome of patients with gastroesophageal dMMR/MSI-H adenocarcinomas. Further characterization of immune microenvironment in upper gastrointestinal malignant tumours is imperative.
Limitations
Our ability to extrapolate our data to a broader context is limited in that our cohort contained mainly patients from an urban setting. Another limitation stems from the study’s experimental design. As the immunohistochemical screening was carried out on surgical resections, we could not include cases with no residual tumour, thereby artificially excluding all the cases with a complete pathologic response. However, given that the latter cases are likely to represent only a minimal proportion of our defined study population, it is unlikely that their exclusion had a significant effect on our evaluation of treatment response. In addition, the immunohistochemical screening of the tumours was performed predominantly with TMAs, which can limit interpretation in the context of possible intratumoural heterogeneity of MMR protein expression, as seen in colorectal adenocarcinomas.38 To address this issue, we used multiple tumoural cores, both primary and metastatic, and confirmed the diffuse MMR loss on full sections of the tumours, and observed concordance. Although correlation between the MMR immunophenotype and MSI status was not confirmed on molecular testing, extensive data support a high rate of concordance between the 2 techniques and near-equivalent value in predicting underlying genetic mutations.39–41 Finally, we had difficulty determining the anatomic origin of the tumour accurately, particularly in patients who had received neoadjuvant therapy. Given that the distinction between esophageal/ junctional and gastric tumours was of particular interest in our study, we devoted an additional effort to reviewing the pathologic description of the resected lesions and correlating the described location with the radiologic localization.
Conclusion
Our findings show that the dMMR immunophenotype can be seen in a substantial proportion of upper gastrointestinal tract carcinomas and, most important, has meaningful prognostic implications. Although these findings have been previously limited to gastric adenocarcinomas, we found an association between the dMMR immunophenotype and overall survival, specifically in the GEJ cohort. This highlights the clinical significance of determining the MMR status in all adenocarcinomas of the upper gastrointestinal tract. However, the implication that dMMR status has for treatment strategies remains controversial, as our data do not show a differential chemoresponse according to dMMR status.
Acknowledgements
The authors thank the Histopathology and Biobank Technology Platforms of the Research Institute of the McGill University Health Centre (MUHC), and the Histology Platform at the Rosalind and Morris Goodman Cancer Research Centre and their staff for providing services and assistance with tissue microarray construction. The authors are likewise grateful to Alfred Cuellar, Louise Turcot and the MUHC Immunohistochemistry laboratory for their outstanding contribution to the immunohistochemistry experiments.
Footnotes
Competing interests: Lorenzo Ferri reports grants or contracts from the Cancer Research Society (grant # 25320). Lorenzo Ferri and Veena Sangwan report grants or contracts from the Montreal General Hospital Foundation. Amit Katz reports grants or contracts from the Israel Cancer Research Fund. Pierre Fiset reports grants or contracts from Bristol Myers Squibb, and payments and honoraria for expert consultation and presentations on biomarker testing and pathology at advisory boards from Amgen, Bristol Myers Squibb, F. Hoffmann-La Roche, Incyte Corp., Merck, Novartis, Pfizer and Precision Rx-Dx. No other competing interests were declared.
Contributors: G. Evaristo and A. Katz contributed equally to this study. P. Fiset, L. Ferri and V. Sangwan designed the study. G. Evaristo, A. Katz, M. Issac, D.-V. Thai, S. Camilleri-Broët, V. Marcus, N. Bertos, M.-C. Guiot, C. Mueller and J. Cools-Lartigue acquired the data, which G. Evaristo, A. Katz and J. Ramírez-GarcíaLuna analyzed. G. Evaristo wrote the manuscript, which L. Ferri, P. Fiset, A. Katz, J. Ramírez-GarcíaLuna, M. Issac, V. Sangwan, D.-V. Thai, N. Bertos, M.-C. Guiot, S. Camilleri-Broët, V. Marcus, C. Mueller and J. Cools-Lartigue critically revised. All authors gave final approval of the article to be published.
Funding: This study was funded by grant #25320 from the Cancer Research Society to Lorenzo Ferri, a grant from the Montreal General Hospital Foundation to Veena Sangwan and Lorenzo Ferri, and a grant from the Israel Cancer Research Fund to Amit Katz.
- Accepted July 25, 2022.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue

{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.