


Abstract
Background: It is well established that female physicians in Canada are reimbursed at lower rates than their male counterparts. To explore if a similar discrepancy exists in reimbursement for care provided to female and male patients, we addressed this question: Do Canadian provincial health insurers reimburse physicians at lower rates for surgical care provided to female patients than for similar care provided to male patients?
Methods: Using a modified Delphi process, we generated a list of procedures performed on female patients, which we paired with equivalent procedures performed on male patients. We then collected data from provincial fee schedules for comparison.
Results: In 8 out of 10 Canadian provinces and territories studied, we found that surgeons were reimbursed at significantly lower rates (26.7%) for procedures performed on female patients than for similar procedures performed on male patients.
Conclusion: The lower reimbursement of the surgical care of female patients than for similar care provided to male patients represents double discrimination against both female physicians and their female patients, as female providers predominate in obstetrics and gynecology. We hope our analysis will catalyze recognition and meaningful change to address this systematic inequity, which both disadvantages female physicians and threatens the quality of care for Canadian women.
Gender bias is prevalent in medicine worldwide, and women experience poorer health than men as a result.1,2 The disparities in the health outcomes of men and women are due to a variety of issues, including missed diagnoses, minimized symptoms, greater burdens of specific diseases and poorly targeted treatment.3 Health care systems continually disadvantage their female patients by underestimating their pain and downplaying other symptoms.4 Women are also under-represented in clinical trials and there is inadequate incorporation of sex- and gender-based analyses into research.5 Recently, attention has turned to the effect of gender bias on medical practitioners. There is a persistent and substantial gender-based gap in physician remuneration, both in Canada and internationally. An Ontario study of physician reimbursement showed that female surgeons are reimbursed 24% less than male surgeons on an hourly basis, even within the same surgical discipline.6 A 2021 study that used Ontario billing and administrative health data found a daily payment gap of 13.5% between female and male physicians after controlling for practice characteristics, region and specialty.7
While the proportion of female physicians in Canada has increased substantially over time, inequity in medicine still exists for women. Female physicians still earn less than their male counterparts, are under-represented in the highest paying medical specialties and tend to enter specialties with lower rates of compensation.8,9 Even within the same specialty, women earn less than their male colleagues, as they are more likely to perform procedures that are less well compensated.10 Indeed, in other highly skilled professions, as the proportion of women increases, remuneration correspondingly declines.11 This phenomenon has been observed in obstetrics and gynecology12 in the United States, where overall reimbursement has fallen as women have filled a higher proportion of positions.13 Thus, there is a prevalent systemic remuneration bias against female physicians in the fee-for service system.
This systemic bias against female physicians has important implications for patient care. Almost 60% of Canadian obstetrician–gynecologists (OB/GYNs) are female, compared with 29% of all surgical specialists and 11% of all urologists.14 As female physicians are more highly represented in obstetrics and gynecology, the care of female patients could suffer because of the wage discrimination against female physicians. Data from the United States have shown that procedures performed on female patients are systematically valued at lower relative value units (RVUs) than equivalent procedures performed on male patients,15 and a recent analysis showed that the use of biased surgeon-reported data has further contributed to a relative undercompensation of the surgical time of American gynecologists compared with that of urologists.16 An informal comparison by Dossa and colleagues of surgical procedures in Ontario demonstrated an analogous trend, although similar analyses for other provinces are lacking.6 Our objective in this study was to determine whether Canadian provincial health insurers reimburse physicians at lower rates for surgical care provided to female patients than for similar care provided to male patients.
Methods
We created a study committee of Canadian clinicians to perform a cross-sectional analysis of data obtained from provincial physician fee schedules. Members of the committee were recruited to ensure a mix of Canadian clinicians trained in the specialties of obstetrics and gynecology and of urology, with representation across provinces and work environments.
We created a list of common gynecologic procedures performed exclusively on female reproductive anatomy, which would correspond to a patient population of predominantly cisgender women, as well as nonbinary people, transgender men and transgender women with ovaries, a uterus, a vagina and/or a vulva. We then analyzed the procedures to identify a comparable procedure performed exclusively on male reproductive anatomy. Through an expert review process, the committee identified procedural pairs for analysis in this study. First, they were asked to independently review a list of gynecologic surgeries and a list of urologic surgeries. The panellists considered each surgery according to the following factors: surgical complexity, type of anesthesia required (general v. regional v. local), surgical time, whether or not a major body cavity was entered and whether or not the surgeon typically required subspecialty training to perform the procedure. We then engaged in a 2-step modified Delphi process. In the first step, the list of gynecologic procedures was confirmed and a list of paired procedures was generated separately by each participant and then collated by the group. In the second step, the collated list was reviewed in 2 separate meetings, where the pairs were discussed according to the above criteria and disagreements were resolved by consensus. After these meetings, a finalized list of 23 procedural pairs was generated by consensus.
Our data source was publicly available provincial fee schedules in the year 2020; we sought compensation details to record total physician fees for the relevant billing codes for each procedure on a provincial and territorial basis. We did not include data for the Northwest Territories or Nunavut, as there were no fee-for-service specialists in obstetrics and gynecology or urology practising there. There was a published fee code for the Yukon, so data were included despite the territory having an alternative payment plan. Most of our procedural pairs involved single-code procedures (e.g., hysterectomy as opposed to hysterectomy plus oophorectomy) so that we could collect consistent data across jurisdictions. When multiple billing codes were associated with a procedure, the total fee was recorded, with appropriate adjustments for each jurisdiction’s fee schedule. For example, in Ontario, any additional code beyond the main procedure code was paid at a rate of 85%. The data from each province and the Yukon were either collected or reviewed by a physician with experience with that jurisdiction’s fee code schedule. If the data for a given procedure were not available within the jurisdiction’s fee schedule, then the procedural pair was excluded from the analysis of fees for that jurisdiction.
After data collection, the fees for each pair were compared and differences were calculated in dollars and as percentages. The mean percentage difference between reimbursement for procedures for female patients and those for male patients was then calculated for each jurisdiction. The mean difference in fees within each procedural pair across all jurisdictions was also calculated.
Results
Through the modified Delphi process, we developed a list of paired surgical procedures exclusive to female and male reproductive anatomy (Table 1). This list included pairs representing all surgical approaches across the surgical spectrum, including 2 ambulatory procedures, 7 minor surgical procedures, 7 major surgeries performed with same-day discharge and 6 major surgeries performed with overnight stay.
Paired gynecologic and urologic procedures
Figure 1 shows the mean reimbursement difference within each procedural pair for all of the study jurisdictions. For 70% of the procedural pairs, the procedure for female patients was reimbursed at a lower rate; the average billing fee for procedures for female patients was 28.1% (standard deviation [SD] 11.1%) lower than the fee for the corresponding procedure for male patients. This corresponds to a mean difference of Can$43.91 for procedures for female versus male patients. After removing Yukon data from the analysis of paired procedures by jurisdiction owing to the alternative payment plan there, the overall difference for all of Canada decreased from 28.1% to 26.7%.

Mean reimbursement differences across Canada within each procedural pair. Negative values indicate higher reimbursement of procedures for male patients; positive numbers indicate higher reimbursement of procedures for female patients. FGM = female genital mutilation.
Figure 2 shows the mean reimbursement difference for all paired procedures by jurisdiction. In most jurisdictions, reimbursement was significantly lower for procedures for female patients than for the matched procedure for male patients. The provinces with the largest discrepancies were Saskatchewan (mean percentage difference in fees of 67.3% [SD 18.4%]), and British Columbia (61.2% [SD 30.1%]). Smaller but still significant differences were seen in Alberta, Manitoba, Ontario, New Brunswick and Prince Edward Island. Notably, there were no statistically significant differences in the average fees in Nova Scotia, Newfoundland and Labrador or Quebec.
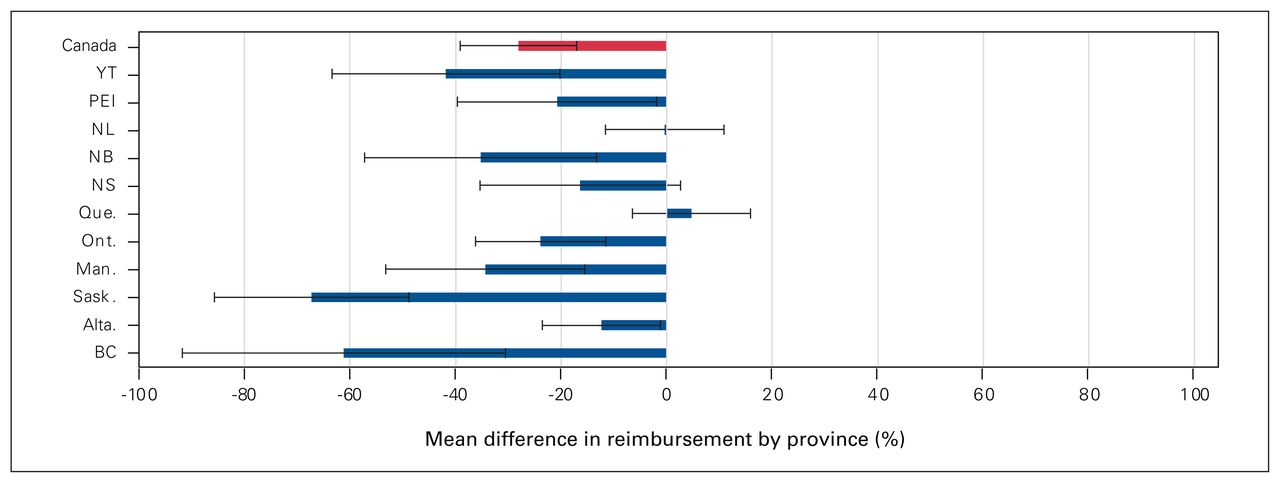
Mean reimbursement difference for all paired procedures in each province or territory. Negative values indicate higher reimbursement of procedures for male patients; positive values indicate higher reimbursement of procedures for female patients.
Discussion
Our study revealed a trend toward devaluation of the health care provided to female patients across Canada. This trend was pervasive across the country, with 7 provinces and 1 territory out of the 11 jurisdictions in the study showing a significant difference between the mean reimbursement for comparable procedures performed for the female and male reproductive tracts. Specifically, we have shown that across Canada, physicians performing procedures on female patients were remunerated at a lower rate than their colleagues performing comparable procedures on male patients. The provinces with the largest discrepancies were Saskatchewan (mean percent different in fees of 67.3% [SD 18.4%]), and British Columbia (61.2% [SD 30.1%]). Smaller but still significant differences were seen in Alberta, Manitoba, Ontario, New Brunswick and Prince Edward Island. There were no differences in the average fees in Nova Scotia, Newfoundland and Labrador or Quebec. The variation between jurisdictions reflects the fact that in Canada, health care is administered on a provincial and territorial basis, and each province or territory’s fee schedule was set at a different time using different processes. Across Canada, the average billing fee for a procedure for female patients was 26.7% (SD 11.1%) lower than the corresponding fee for male patients. While some of the procedural pairs may reflect different surgical approaches (e.g., ovarian detorsion is performed laparascopically whereas testicular detorsion is typically performed with a transscrotal approach), we felt it was important to look at the financial value assigned to a procedure to save female versus male gonads.
OB/GYNs, who operate exclusively on the female reproductive tract, constitute 3.2% of Canadian physicians and earn 3.2% of total service fees. In contrast, urologists, who provide similar care for men and some of whom care for women, constitute 1.0% of Canadian physicians but earn 1.3% of total service fees.14 The findings in the present study indicate that this discrepancy is probably a structural gender bias reflected in provincial and territorial remuneration schedules, rather than evidence that physicians operating on the male reproductive tract work harder or work longer hours. The fact that reimbursements for OB/GYNs are lower than for urologists does not reflect less rigorous training or lower practice expenses. OB/GYNs are surgical specialists who undergo the same length of training and have the certification requirements per the Royal College of Physicians and Surgeons of Canada17,18 as urologists. Moreover, gynecologists who also practise obstetrics pay the Canadian Medical Protective Agency nearly 400% higher premiums for malpractice insurance than urologists or most other surgical specialists.19 The high premiums reflect in part the high-risk nature of the conditions and care of OB/GYNs’ patients, but this is not at all reflected in the remuneration OB/GYNs receive for the high-risk procedures they perform. Instead, the lower reimbursements for OB/GYNs indicate a devaluation of the health care provided to female patients and, ultimately, a relative underevaluation of women’s health.
In a 2007 Norwegian survey, medical trainees were asked to rank different medical conditions according to the relative prestige of treating them and found that ovarian cancer was considered a less prestigious disease than testicular cancer.20 Fibromyalgia, a condition that is more commonly diagnosed in women, was ranked as having the lowest prestige among 38 conditions. These findings are echoed in the American literature, which has demonstrated a substantial difference in the relative value units (RVUs) assigned to procedures specific to female versus male patients.21 Although the Canadian health care system does not code procedures according to RVUs, the data presented here suggest that a similar pattern exists in Canada.
Certainly, this trend is influenced not only by patient sex but also by physician gender. Like Canada, in the US, obstetrics and gynecology has the highest proportion of female physicians among the surgical specialties, and it also has the lowest remuneration rate of all procedural specialties.22 Moreover, in the last 5 years there has been a 15%–20% decrease in fee-for-service fees for common procedures in obstetrics and gynecology.16 Indeed, there is a strong negative relationship between the proportion of female physicians in a specialty and the mean salary in that specialty, with gender composition correlated with 64% of the variation in salaries among the medical specialties in the US.23 Cohen and Kiran found a similar trend in Canada, where female specialists earned 40% less than their male counterparts.8 This gender bias may reflect inherent biases in the various provincial fee schedules, as suggested by previous studies.6,7 The authors emphasized that double discrimination is at play. While female physicians are devalued by provincial fee schedules, those who care for female patients are even further devalued. As female providers predominate in obstetrics and gynecology, this may reflect one form of structural sexism leading to decreased compensation for female surgeons.
More than just disadvantaging female physicians, this systematic oppression threatens the quality of care for women. A recent commentary in Obstetrics & Gynecology showed that poor reimbursement of gynecologic surgeons disproportionately affects female surgeons and also leads to a higher prevalence of low-volume surgeons and higher complication rates for their patients.24
Limitations
Because our study relied on publicly available data, we could not analyze individual patient and health system data when comparing procedural pairs. We relied on a Delphi protocol, rather than operating room data, to determine equivalency between procedures, especially with respect to complexity. Surgical complexity, which can be further compounded by patient complexity, is a subjective measure, and no empiric data on this are available. Furthermore, we did not have access to physician payment or salary data at an individual level, so we could not confirm that our findings reflect an actual difference in overall income between physicians who provide care for female patients and those who provide care for male patients.
The mechanism by which fee schedules are established varies by province and territory, but it usually includes some influence by individual medical or surgical disciplines, known as sections. In some provinces, like Alberta and British Columbia, the section receives an allocation sum and then determines how it is allocated for specific codes unique to that section. The relative allocation per section is 1 place where bias can occur. The sections also often “own” specific shared codes that are billed most frequently by that section. For example, a urology section may own the code for midurethral sling and therefore determine the level of compensation for this procedure in both urology and gynecology. Similarly, a family medicine section may own the code for vaginal delivery. If that section increases the compensation for this to encourage family physicians to offer primary maternity care, there will be an impact on the obstetrics and gynecology section, which must allocate more of its total sum to vaginal delivery, leaving less for gynecologic procedures. While the details of these policies clearly affect how reimbursements are determined, they should not detract from the underlying message of systemic bias in the provincial and territorial Canadian health care systems that has a negative impact on women and the providers who serve them. The mechanisms of this bias are complicated and they vary across Canada, but nevertheless this bias seems to be the norm.
The devaluation of health care provided to women should be further explored, starting with a focus on the individual provincial and territorial fee schedules. There should be investigations into how these were established, what biases underly them and how “relativity” is determined when defining physician remuneration. Finally, research should also focus on how the pay inequity revealed here affects the health outcomes for female patients and advocacy efforts should then be made to correct this discrimination. Hence, we advocate for closing the gap in the way OB/GYNs are trained, treated and renumerated relative to other surgical specialists. Physicians and researchers should advocate for further transparency at the provincial and territorial level, and interventions to further identify and remedy gender gaps in remuneration policies must be prioritized. With equity, diversity and inclusion criteria now mandated at many levels of government, it is time for our profession to march consistently with government policy and close the inequities revealed here and prioritize the health and health care delivery of the 50% of the Canadian population served by OB/GYNs.
Conclusion
Across Canada, surgical specialists treating women are reimbursed at a lower rate than surgical specialists treating men, for similar procedures. This reflects double discrimination both against the care providers who manage the care of female patients and against female patients themselves.
Footnotes
Presented at the annual meetings of the Canadian Society for Pelvic Medicine, Apr. 30, 2022, Toronto, Ont., and the International Urogynecological Association, June 14–18, 2022, Austin, Tex.
Competing interests: G. Cundiff has received book royalties from Wolters Kluwer and honoraria from AbbVie. He is the chief medical officer for Amara Therapeutics and has a patent pending with this company. F. Mohtashami has received educational grants from Medtronic, Hologic and Boston Scientific. E. Brennand has received speaking fees from Searchlight Pharma. C. McDermott is a medical advisor for Szio+ and COSM and has stocks or stock options in these companies. She is also a speaker for Pfizer.
Contributors: M. Chaikof, G. Cundiff, F. Mohtashami, A. Millman, E. Brennand and C. McDermott conceived the study. M. Chaikof, G. Cundiff, A. Millman, M. Larouche, M. Pierce, E. Brennand and C. McDermott acquired the data, which M. Chaikof, G. Cundiff, F. Mohtashami, A. Millman, M. Pierce, E. Brennand and C. McDermott analyzed. M. Chaikof, G. Cundiff, F. Mohtashami, E. Brennand and C. McDermott wrote the article, which G. Cundiff, F. Mohtashami, A. Millman, M. Larouche, M. Pierce, E. Brennand and C. McDermott critically revised. All authors gave final approval of the version to be published.
- Accepted October 12, 2022.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
In this issue

{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- Eliminer les causes profondes de lecart salarial entre les sexes en medecine au Canada
- Addressing the root causes of the sex-based pay gap in medicine in Canada
- The Yukon data are incorrect
- Correction to: "Surgical sexism in Canada: structural bias in reimbursement of surgical care for women"
- Pourquoi ignore-t-on encore lequite entre les genres en chirurgie?
- Why are we ignoring gender equity in surgery?