


We read the article entitled “Mechanical versus bioprosthetic valves in chronic dialysis: a systematic review and meta-analysis” by Kim and colleagues,1 with great interest. The authors attempted to address limitations of previous meta-analyses by expanding the searching strategy and exhausting more databases without placing any language restriction. They concluded that the significant benefit of lower all-cause mortality with the use of mechanical prosthesis (MP) was at the expense of higher risks of bleeding and stroke. We appreciated the authors’ efforts and contribution, and concur with the authors that most studies were subject to high risk of unmeasured confounding bias owing to unreported demographics, which lowers the quality of evidence considerably. However, we believe that the prosthetic position upon which cardiac surgeons operate is a significant contributor to not only conceptual, but also statistical heterogeneity. Besides, compared with relative risk (RR) that Kim and colleagues selected for the analysis of all-cause mortality, hazard ratio (HR) is supposed to be a more appropriate statistic, as it incorporates time into the consideration.
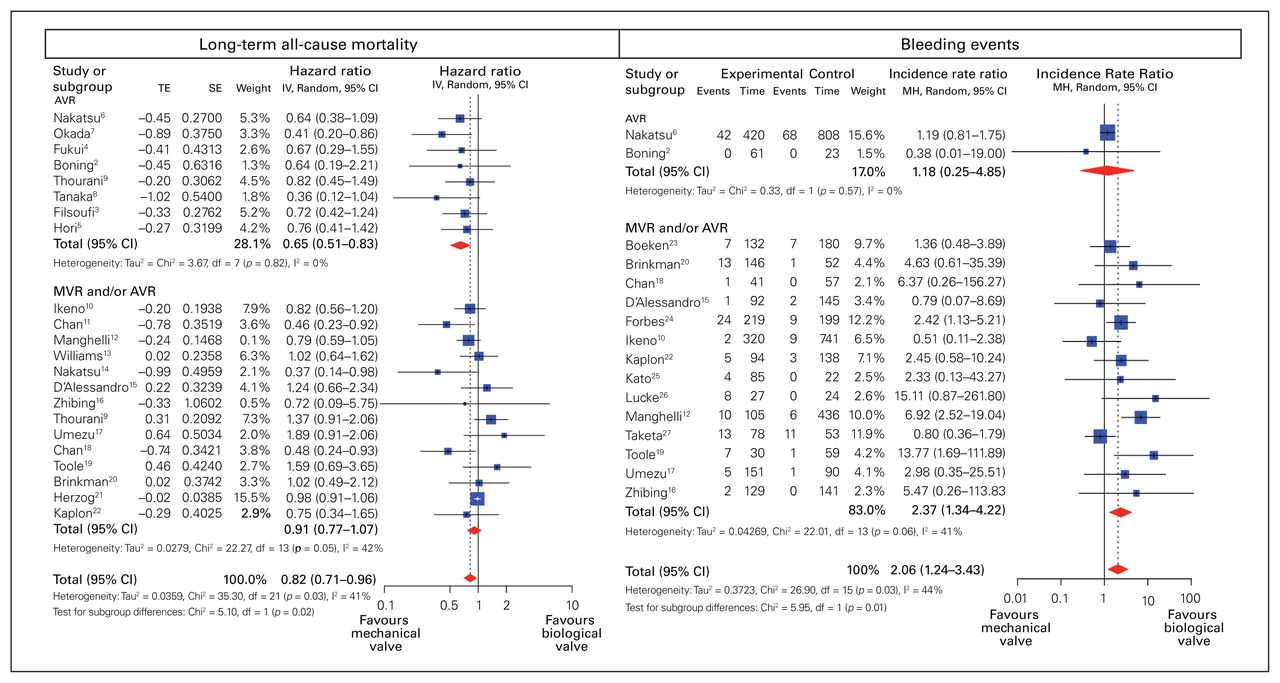
Thus, we followed Kim and colleagues’ inclusion criteria and reconducted the meta-analysis with the introduction of a subgroup analysis based on valve position. There are 8 studies2–9 providing comparative long-term survival outcome for aortic valve replacement (AVR) between MP and bioprosthesis (BP) in dialysis patients. We showed that dialysis patients using MP for AVR was associated with significantly lower long-term all-cause mortality than those using BP (HR 0.65, 95 % confidence interval [CI] 0.51–0.83, I2 = 0 %) (Figure 1). On the other hand, the long-term overall survival was comparable between MP and BP (HR 0.91, 95 % CI 0.77–1.07, I2 = 0 %) (Figure 1) in mixed cohorts of AVR and mitral valve replacement (MVR). Regarding the bleeding events, although the use of MP was associated with a considerably higher risk in studies including mixed cohorts of AVR and MVR (incidence rate ratio [IRR] 2.37, 95% CI 1.34–4.22, I2 = 41%), we found that there was no significant difference in bleeding events between MP and BP in patients undergoing AVR (IRR 1.18, 95% CI 0.28–4.85, I2 = 0 %) (Figure 1). One plausible explanation for similar bleeding risk between MP and BP in dialysis patients undergoing AVR may reside in the lower target of international normalized ratio (INR), usually less than 2.5, used in this population, as compared with the target of 3.0 used in MVR.28 In fact, it has been shown in previous meta-analysis that MP conferred a significantly greater bleeding risk than BP when INR was above 2.5, while bleeding events were comparable when INR was below 2.5.29 Of note, the valve position appeared to be a significant contributor to heterogeneity as both subgroup analyses revealed significant quantitative interaction between different valve positions (p = 0.02 for long-term, all-cause mortality and p = 0.01 for bleeding events) (Figure 1). In summary, when taking the valve position into consideration, our subgroup analysis revealed that MP may be a feasible choice in dialysis patients undergoing AVR given significant lower long-term all-cause mortality with comparable bleeding risk as compared with BP.
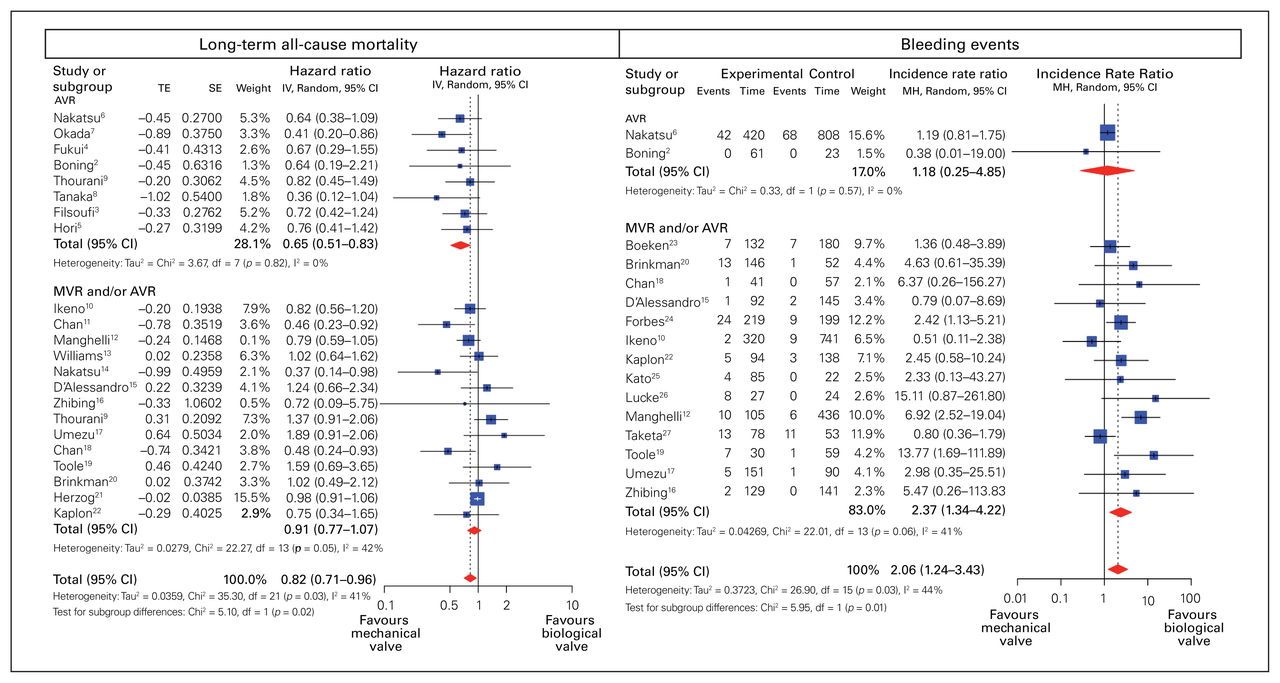
Forest plot of comparative long-term all-cause mortality and bleeding events between mechanical and bioprosthetic prosthesis. Meta-analyses were carried out using random-effects model with restricted maximum likelihood as an estimator for between-study variance.
Footnotes
Competing interests: None declared.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.