


Abstract
Background: The rapid evolution of genetic technologies and utilization of genetic information for clinical decision-making has necessitated increased surgeon participation in genetic counselling, testing, and appropriate referral of patients for genetic services, without formal training in genetics. We performed a scoping review to describe surgeons’ knowledge, perceptions, attitudes, and barriers pertaining to genetic literacy in the management of patients who had confirmed cancer or who were potentially genetically at risk.
Methods: We conducted a scoping review in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses Extension for Scoping Reviews checklist. We performed a comprehensive literature search, and 2 reviewers independently screened studies for inclusion. These studies included surgeons involved in the care of patients with confirmed gastrointestinal, breast, and endocrine and neuroendocrine cancers, or patients who were potentially genetically at risk for these cancers.
Results: We analyzed 17 studies, all of which used survey or interview-based formats. Many surgeons engaged in genetic counselling, testing, and referral, but reported low confidence and comfort in doing so. Knowledge assessments showed lower confidence in identifying genetic inheritance patterns and hereditary cancer syndromes, but awareness was higher among surgeons with greater clinical volume or subspecialty training in oncology. Surgeons felt responsible for facilitating these services and explicitly requested educational support in genetics. Barriers to genetic literacy were identified and catalogued at patient, surgeon, and system levels.
Conclusion: Surgeons frequently engage in genetics-related tasks despite a lack of formal genetics training, and often report low knowledge, comfort, and confidence in providing such services. We have identified several barriers to genetic literacy that can be used to develop interventions to enhance genetic literacy among surgeons.
The rapid evolution of genetic testing technology over recent decades has allowed genetic information to guide clinical care. Approximately 5%–10% of cancers are hereditary, and once an underlying germline mutation is identified, this information has implications for affected patients and their health care professionals when weighing management options, as well as for unaffected relatives who may benefit from screening, risk-reducing surgeries, or both.1 Results from genetic testing are increasingly used in therapeutic decision-making pertaining to surgery and systemic therapy, such as the use of poly–adenosine diphosphate ribose polymerase (PARP) inhibitors in patients with genetic alterations causing ovarian, prostate, and breast cancer.2,3 As such, there is a gap between the number of health care professionals with specialized training in genetics and the patients who may benefit from such services. Consequently, health care professionals with minimal or no formal training in genetics are increasingly required to provide basic services related to ordering tests, providing pretest counselling, and initiating clinical management.4,5 However, there is growing evidence that these health care professionals may be ill-prepared to provide such services.6–8
Surgeons are frequently involved in the care of patients who require genetic services, including referral of patients identified to be at increased risk for further genetic risk assessment and counselling, appropriate counselling regarding screening and surgical management, and subsequent surveillance of those with confirmed cancer. However, little is known about surgeons’ practices within those domains. Thus, we sought to perform a scoping review to summarize the current literature pertaining to knowledge of, perceptions about, attitudes toward, and barriers to referrals and genetic literacy among practising surgeons involved in the care of patients who had confirmed cancer or who were potentially genetically at risk.
Methods
We performed a scoping review of the literature to identify and summarize studies of referrals for genetic risk assessment and counselling, and knowledge, perceptions, attitudes, and barriers pertaining to genetic literacy among surgeons. This study was designed and conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses Extension for Scoping Reviews (PRISMA-ScR),9 as well as the methodological framework developed by Arksey and O’Malley.10
Data sources and search strategy
We employed a comprehensive search approach to locate published studies and conference materials. A preliminary search was conducted in Ovid Embase, followed by an analysis of relevant citations, to identify applicable text words and subject headings. We developed a comprehensive search approach in Ovid Embase and then adapted it for Ovid MEDLINE and Web of Science Core Collection. All databases were searched from 2000 to August 2021 and limited to English language. The complete search strategies for all databases are provided in the supplementary data (Appendix 1, available at www.canjsurg.ca/lookup/doi/10.1503/cjs.001523/tab-related-content). All search results were imported into Covidence systematic review software for deduplication and screening. The reference lists of all eligible studies were screened to identify any additional studies.
Inclusion and exclusion criteria
Studies were included for analysis if they reported on knowledge, perceptions, attitudes, and barriers with respect to genetic literacy and referrals for genetic risk assessment and counselling among surgeons (i.e., general, colorectal, breast, and endocrine surgeons, and surgical oncologists) who manage the following cancer types: breast, colon, rectum, stomach, pancreas, thyroid, parathyroid, adrenal, and neuroendocrine or carcinoid. Studies were excluded if they assessed other cancer types or if they reported on surgeons within other surgical subspecialties (i.e., urology or urologic oncology, and gynecology or gynecologic oncology). Additional reasons for exclusion were studies involving pediatric populations and cancers, duplicate studies, abstracts with insufficient details for data abstraction and analysis, studies with inadequate surgeon-level data, or studies that summarized only clinical practice patterns.
Screening
Screening of studies for inclusion and analysis was conducted by 2 reviewers (Z.M.M. and L.Y.N.F.) independently. Any differences were resolved through group discussion with an additional reviewer (S.J.M.).
Data abstraction and analysis
Two reviewers (Z.M.M. and L.Y.N.F.) abstracted the data from the included full-text articles independently and then cross-checked for discrepancies. A data abstraction table was developed a priori for this process, which included study details (i.e., year of publication, study period, analytic method, and study design), surgeons’ knowledge, self-reported perceptions and attitudes, and barriers to referrals and genetic literacy. Thematic analysis was conducted to categorize barriers by patient-, surgeon-, and system-level factors.11
Results
Using the search strategy outlined, we identified 3351 studies, of which 601 were identified as duplicates and removed (Figure 1). After title and abstract screening, 58 studies remained for full-text review, and 17 were included in the final analysis.12–28 The most common reason for exclusion of full-text articles was a lack of surgeon-level data (n = 21). The relevant details of each included study are provided in Table 1.
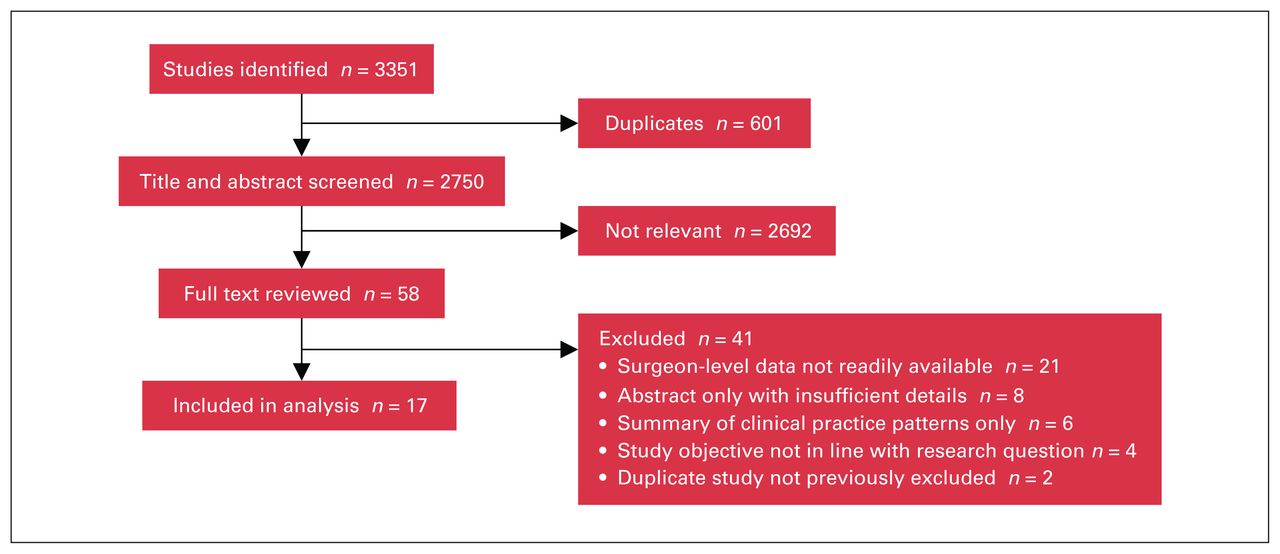
Flow diagram of study screening and selection for final analysis.
Summary of studies included in review
Among the 17 studies evaluated, the earliest was published in 2005. All studies used either survey (n = 14) or interview (n = 3) formats for data collection. Eight studies were from the United States, 6 were from Europe, 2 were from Australia or New Zealand, and 1 was from Canada. Analytic approaches included quantitative (n = 8), qualitative (n = 3), and mixed methods (n = 6). Five studies assessed surgeons’ genetic knowledge, 17 studies characterized their perceptions and attitudes, 7 studies described barriers to genetic literacy, and 1 study evaluated an intervention to improve genetic literacy among surgeons.
Knowledge assessment
Five studies performed knowledge assessments of surgeons’ genetic literacy (Table 2). These examined surgeons’ awareness of the availability of genetic testing, understanding of genetic inheritance patterns, and familiarity with indications for genetic screening and surveillance, and referral for genetic risk assessment and counselling. Subspecialty-trained surgical oncologists reported higher awareness of genetic testing options and knowledge of the referral process for genetic risk assessment and counselling than those without subspecialty training (Table 2). Commonly, surgeons had some difficulty with questions testing genetic inheritance patterns and criteria to identify hereditary cancer syndromes.
Knowledge assessment of genetic literacy among surgeons within the included studies
Perceptions and attitudes
Most of the included studies provided surgeons’ self-reported perceptions about and attitudes toward genetic literacy (Table 3). Across 4 studies, surgeons felt they should take on a leading role in referring patients for genetic testing or counselling.12,16,25,27 Surgeon confidence and comfort with counselling patients regarding genetic testing or its results varied across 6 studies.13,15,16,18–20 Repeatedly, surgeons acknowledged the need for improved genetic literacy and its value in their clinical practice.12,13,15,21
Key findings of perceptions and attitudes pertaining to genetic literacy among surgeons within included studies
Barriers
We compiled all of the surgeon-reported barriers to genetic literacy, testing, referral, and counselling within the included studies (Table 4). After thematic analysis, similar barriers were grouped and classified as surgeon-, patient-, or system-level challenges (Table 5). Nine unique barriers were identified in this manner, with most (n = 5) being at the system level. These included a lack of clarity regarding the health care provider responsible for initiating genetic testing and managing high-risk patients, ease of patient referral to genetic risk assessment and counselling, timeliness of appointments following referral, availability of genetics clinics, and difficulties posed by private insurance coverage for genetic testing and counselling. Uncertainty surrounding provider responsibility was the most commonly cited challenge by surgeons within the included studies. Surgeon-level barriers (n = 3) included scarcity of time to provide counselling, difficulty surrounding interdisciplinary communication, and surgeon attitude toward genetic testing and counselling. The only patient-level barrier reported was compliance with attending appointments.
Catalogue of barriers to genetic literacy, referral, and counselling, as identified by surgeons within included studies
Thematic list of barriers to genetic literacy, ordered by frequency within included studies
Discussion
In recent years, the shortage of genetic counsellors, lengthy wait times of genetics clinics, and increased availability and awareness of genetic information have resulted in a greater need for health care professionals with minimal or no formal training in genetics to provide genetics-related services. In this study, we have shown that surgeons participate in many such genetics-related tasks despite low confidence in knowledge, and the considerable challenges posed by barriers at system, surgeon, and patient levels.
Most surgeons order genetic testing and provide genetic counselling to patients.13,14,16–18,21,23 This is despite variable knowledge pertaining to genetic inheritance patterns for breast and colorectal cancer, availability of testing, and criteria for at-risk patient identification.14,17,19 Inadequate curricular exposure to genetics and other cancer-related specialties during surgical residency may contribute to those findings.29,30 To that end, there is variable description of genetics and hereditary cancer topics within the curricula of several surgical accreditation bodies.31–33 With the increasing complexity of genetic information, testing may lead to results requiring more nuanced interpretation and counselling.34,35 Poor genetic literacy among surgeons can lead to negative consequences for patient care. For example, ordering of incorrect genetic tests can lead to pathogenic variants being missed in relevant genes or increased detection of variants of uncertain importance that may be confusing for patients and health care professionals to interpret. Misinterpretation of test results, along with insufficient, incorrect, or missed opportunities for genetic counselling are also possible and may result in underuse or inappropriate utilization of screening and prophylactic surgery both for affected individuals and their at-risk unaffected relatives.36–38 These findings underscore an important need for knowledge-based interventions to improve genetic literacy among surgeons.
Provision of genetics-related services by health care professionals with minimal or no formal training in genetics is met with mixed opinions.37,38 Surgeons often report low comfort with the provision of genetics-related services. In one study, the proportion of surgeons comfortable with counselling their patients regarding hereditary colorectal cancer ranged from 21% to 63%.19 While we noted similar results among surgeons managing hereditary breast cancer, our findings also indicate that confidence with and utilization of genetic services increases with clinical volume and subspecialty training.13,14,18 Interestingly, several surgeons explicitly requested educational support for genetic knowledge, testing, and counselling.13,15 This suggests that low comfort may be related to gaps in genetic literacy, a notion that is bolstered by surgeons’ desire to participate in genetics-related services for their patients.12,16 Many surgeons feel that their participation in ordering genetic testing, for example, can expedite care and minimize delays.16
“Mainstreaming” of genetic testing has been proposed as an approach to address some of the concerns outlined above and is currently implemented across several jurisdictions in Canada.20,39,40 Mainstreaming interventions provide health professionals with minimal or no knowledge in genetics with education, as well as a systematized approach for genetic testing and obtaining results.41 Within the province of Ontario, for example, physician-led mainstreaming initiatives have been recommended and initiated to provide standardized organization and delivery of genetic services.40 Once the initial testing has been performed, patients who require further access to specialized genetic health professionals may then be selectively referred. To that end, surgeons within our analysis held favourable views toward the mainstreaming of genetic testing.12,21 While mainstreaming appears to be a promising approach, a robust characterization of the attitudes of interested parties and patient outcomes across cancer sites is likely necessary. Furthermore, mainstreaming in itself does not preclude the need for high-quality interventions targeting genetic literacy among surgeons.
We identified and catalogued various barriers to genetic literacy, referral, testing, and counselling. The most common surgeon-level barrier reported was a lack of time to devote toward genetics-related activities.15 We noted that system-level barriers were related to the process of referrals made to certified genetic counsellors. To that end, we identified only 1 study within this evidence synthesis that employed a checklist-based intervention to simplify the identification of patients as potential candidates for genetic counselling referrals.15 Unfortunately, this intervention did not lead to significant differences in patient referral. A more recent study not described in our analysis yielded similar results, in which health literacy interventions for surgical oncologists and nurses did not improve referrals to genetic counselling.42 These findings suggest that further work is needed to better understand existing barriers, and to design and implement effective interventions to improve the genetic literacy and capacity of surgeons.
Optimal strategies to address the barriers to genetic literacy that our work has identified remain undefined. Nonetheless, we hypothesize that several surgeon- and system-level barriers may be addressed by relatively straightforward measures. These may include, for example, identifying the most responsible practitioner within a cancer disease site team to triage and make referrals for further genetic work-up, provision of a framework to simplify the referral process (e.g., electronic referrals), and mandating a time frame within which all new referrals must be seen. The addition of a patient navigator role and genetic specialists to cancer disease site teams or multidisciplinary tumour conferences may lead to improved patient attendance at genetics appointments and better interdisciplinary contact for surgeons. In the province of Ontario, Cancer Care Ontario has published a series of recommendations with the intention of enhancing delivery of clinical cancer genetic services.40 These recommendations were developed by a working group and are aimed at the interdisciplinary team, the patient’s episode of care, and the province as a whole. Within the broader Canadian context, future research may aim to determine the effectiveness of such strategies and if they should be adopted in other provinces and territories.
Our work provides a comprehensive and context-specific synthesis of the literature relating to surgeons’ referral patterns, and knowledge, perceptions, attitudes, and barriers pertaining to genetic literacy. In doing so, we have catalogued reported barriers based on their role at the surgeon, patient, and system levels. These findings may now guide future studies of targeted interventions to improve surgeons’ genetic literacy, allowing them to more effectively incorporate genetic services within routine clinical practice. The strengths of our evidence synthesis include a comprehensive search strategy and rigorous screening process, based on PRISMA guidelines for scoping reviews.
Limitations
Our findings and list of barriers are context-specific to the surgeons and cancer disease sites included in this study and may not be generalizable to other health care professionals and disease sites, which is an important limitation. We analyzed data from studies conducted in Europe, Canada, Australia and New Zealand, and the US, but were unable to find relevant studies from other geographic locations where issues related to referral and genetic literacy may be different. Finally, the results from the included studies are heavily dependent on surgeon self-reporting, which is subject to reporting bias.43
Conclusion
We found that surgeons managing gastrointestinal, breast, and endocrine and neuroendocrine cancers are frequently engaged in genetics-related services. Surgeon knowledge, comfort, and confidence in providing these services is often low but is increased with clinical volume and subspecialty training. There is both a need and desire for knowledge-related and non-knowledge-related interventions targeting surgeons’ genetic literacy.
Acknowledgements
The authors thank Lia McCarthy for her contributions during the early stages of this study.
Footnotes
Competing interests: Rona Cheifetz reports a Community–University Engagement Grant from the University of British Columbia for the development of a virtual support group for BRCA mutation carriers. Dr. Cheifetz is also an unpaid board member for the non-profit BRCA Education and Awareness Society. Shaila Merchant reports unpaid leadership roles in the Canadian Society of Surgical Oncology and in the Specialty Review Committee for Surgical Oncology, Royal College of Physicians and Surgeons of Canada. No other competing interests were declared.
Contributors: Zuhaib Mir, Linda Fei, Rachelle Dinchong, Nicholas Cofie, Nancy Dalgarno, Alison Rusnak, Rona Cheifetz, and Shaila Merchant made substantial contributions to the conception and design. All authors contributed to the data acquisition, analysis, and interpretation. Zuhaib Mir, Linda Fei, and Shaila Merchant drafted the manuscript, which all authors reviewed. All authors gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: The authors acknowledge financial support for this study, which was provided by the Clinical Teachers’ Association of Queen’s University Research Endowment Fund.
- Accepted November 24, 2023.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue

{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.