


Abstract
Background: The direct lateral (DL) approach to total hip arthroplasty is more commonly used than the newer direct anterior (DA) approach. Both approaches use collared or collarless femoral stems. We sought to assess implant stability of stem designs implanted with the DL approach and compare outcomes from this cohort with those of a previously reported cohort of patients who underwent arthroplasty with a DA approach. We also sought to determine if early recovery influences differences in migration.
Methods: Patients underwent total hip arthroplasty using the DL or the DA approach and were randomized to receive either a collared or collarless, cementless femoral stem. On the day of surgery and at 6 follow-up visits through to 1 year, patients underwent supine radiostereometric imaging to track implant migration. At follow-up visits, patients performed an instrumented walking test to assess their functional ability and logged an average daily step count to assess their activity levels. We assessed whether patient function and activity were correlated with migration.
Results: Stem design did not have a significant effect on migration for the DL group (p = 0.894). Compared with the DA group, the DL group migrated significantly less for both collared (p = 0.031) and collarless (p = 0.002) stems. Migration was not correlated with function or activity at any time point (p > 0.05).
Conclusion: Most implant migration occurred from the day of surgery to 2 weeks after the operation and stabilized thereafter, suggesting adequate fixation and a low risk for aseptic loosening in both patient groups.
Total hip arthroplasty (THA) is the only viable treatment for patients with end-stage osteoarthritis of the hip, and is successful and reliable in improving patients’ quality of life, restoring function and alleviating pain.1,2 Over the last 5 years, the number of THA procedures performed in Canada has increased 17.4% to more than 58 000 annually.3 This continuous increase in THA procedures has placed an economic burden on health care systems. To help reduce costs and cope with this burden, demand exists to further optimize surgical pathways, implement rapid recovery programs and improve patient outcomes.4,5
The direct lateral (DL) surgical approach is the preferred method for THA for about 42% of orthopedic surgeons worldwide.6 The DL approach provides good exposure of the femur and acetabulum, and has a low risk for dislocations. However, the intramuscular nature of the DL approach may lead to greater postoperative pain and longer hospital stays or rehabilitation times.7 In recent years, the direct anterior (DA) approach has increased in popularity for its muscle-sparing nature, leading to a faster recovery, less postoperative pain and an earlier discharge from the hospital.8,9 However, the steep learning curve and decreased surgical view of the femur associated with the DA approach may lead to complications such as risk of fracture and dislocation.6,9,10 Studies have also reported a higher rate of aseptic loosening associated with the DA approach, possibly owing to the greater likelihood of using an undersized stem.10–12
Although some femoral stem migration is common and acceptable throughout recovery, substantial and continuous early migration can predict loosening of the femoral component and implant failure.13,14 Collared stem designs can provide greater stability and are associated with less migration than collarless designs.13,15 Radiostereometric analysis (RSA) is recognized as the gold standard for tracking implant migration and can detect implant movement with an accuracy of 0.2 mm for translations and 0.5° for rotations.14,16,17 Radiostereometric analysis plays an important role in evaluating stem fixation after THA and can be used to compare outcomes between different stem designs and surgical approaches.
The purpose of the present study was to evaluate implant stability between stem designs after primary THA using the DL approach, and to compare outcomes in this cohort to those of a previously reported cohort of patients who underwent the DA approach.18 We hypothesized that the collared stem design would mitigate migration compared with the collarless design, and that patients who underwent the DL approach would have less implant migration than those who underwent the DA approach. We also hypothesized that recovery of patient functional abilities and level of activity would influence femoral stem migration.
Methods
Study design and participants
We included patients undergoing unilateral primary THA. Patients were prescreened and excluded based on the following criteria: symptomatic contralateral hip osteoarthritis, revision or bilateral THA, a body mass index greater than 40, cognitive defects or neuromuscular disorders that would prevent a walking test, inability to understand English and living more than 100 km from our institution given the frequent followup visits required for the study. Eligible patients were recruited and provided written informed consent before participation.
Using an expertise-based approach,19,20 patients recruited for this study underwent THA using either the DL approach or the DA approach depending on their surgeon referral. Two fellowship-trained arthroplasty surgeons performed all the operations; 1 surgeon (E.M.V.) performed all the DL surgeries and another (B.A.L.) performed all the DA surgeries. Before their surgery, we randomized patients within each surgical approach group to receive either a collared or collarless Corail cementless femoral stem (DePuy Synthes) using block randomization with concealed envelopes. As required for each patient, the surgeon could choose to use a standard or a high-offset stem, along with either a 28 mm, 32 mm or 36 mm cobalt–chromium femoral head. All patients received a Pinnacle cup, with AltrX highly crosslinked acetabular liner (DePuy Synthes) as the acetabular component. To enable tracking of implant migration with RSA, a minimum of 6 tantalum beads (diameter 1 mm) were inserted into the cortical bone of the proximal femur intraoperatively.
We recruited patients in both surgical approach groups concurrently and followed an identical protocol. We have previously reported on the differences in migration and clinical outcomes between stem designs for the DA cohort.18 Here, we report the differences in outcomes between stem designs for the DL cohort and perform further analyses to compare outcomes between the DL and DA cohorts.
Radiographic analysis
Each patient underwent an RSA exam in a supine position within 24 hours after their surgery, before they were discharged from the hospital. Follow-up RSA exams were conducted at 2 weeks, 4 weeks, 6 weeks, 3 months, 6 months and 1 year after surgery. Patients were consistently positioned at each exam with a uniplanar calibration cage (RSA Biomedical) used to define the coordinate system. We used model-based RSA software (RSAcore) to analyze radiographs. We defined positive translation directions as proximal translation in the y-axis, medial translation in the x-axis and anterior translation in the z-axis. We defined positive rotation directions as internal rotation about the y-axis, anterior tilt about the x-axis and valgus rotation about the z-axis.
We used anteroposterior radiographs to evaluate stem fit in the femoral canal. As per the standard practice of each surgeon, immediate postoperative radiographs were assessed for the DL group and intraoperative radiographs were assessed for the DA group. The discrepancy in radiograph timing is a generalized difference, as intraoperative imaging is routinely used with the DA surgical technique.21,22 We used the femoral head size to calibrate the measurements. We assessed stem fit in the femoral canal using the canal fill ratio (CFR), calculated at halfway from the shoulder to the tip of the stem. We considered a CFR of less than 80% as an undersized stem.23 To characterize femoral bone quality, we analyzed preoperative anteroposterior radiographs for both patient groups. Using the Dorr method, explained in a previous article,18 we measured the canal-to-calcar ratio (CCR) and used it to categorize patients as Dorr type A (CCR < 0.5), B (CCR 0.5–0.75) or C (CCR > 0.75).24
Additional measures
We obtained patient demographic information from the hospital’s database. At preoperative, 3-month postoperative and 1-year postoperative clinic appointments, patients completed the Short-Form 12, Western Ontario and McMaster Universities Osteoarthritis Index and University of California Los Angeles Activity Score questionnaires. Clinicians also completed the Harris Hip Score evaluation for each patient at these visits.
To assess patient function, patients completed 3 trials of the timed-up-and-go (TUG) functional performance test at their follow-up visits at 2 weeks, 4 weeks, 6 weeks, 3 months, 6 months and 1 year after surgery. Patients were instructed to begin the test in a seated position, stand and walk to a marked target 3 m away, turn around, walk back to the chair and sit down. For the duration of the TUG tests, patients wore a previously validated, wearable sensor system that automatically extracted time to test completion.25 We used the average total time to complete the TUG test across the 3 trials as the overall measure of patient function, where less time to complete the test suggested greater function. To assess patient activity, each patient was given a wrist-worn activity tracker (Fitbit Flex 2) at their preoperative clinic appointment. We asked patients to wear their activity tracker for at least a 7-day period leading up to each postoperative follow-up visit. We calculated an average daily step count from each 7-day period.26,27
Statistical analysis
We completed all statistics using Prism version 8.2.1 (GraphPad Software) and reported data as means with ranges or standard deviations. We used unpaired Student t tests to compare age, body mass index, questionnaire scores and CFR between surgical approach groups and a Fisher exact test to detect a difference in sex, implant details and Dorr type. We used a mixed-effects model with Sidak multiple comparison tests to compare femoral stem migration between patient groups over time. We used the Pearson correlation coefficient to correlate migration with function and activity for each patient group at all time points. Statistical significance was set at a p value of 0.05 or less.
We defined femoral stem migration as the primary outcome of this study. Based on a previous study of cementless femoral stem RSA at our centre, to detect a difference in migration of 0.4 mm with 80% power, a significance of 0.05 and a standard deviation of 0.45 mm, we required a sample size of 20 per group.28 To allow for a 20% dropout rate, we increased the target recruitment to 24 per group. The target recruitment was met and completed for the DA group. Given supplier issues for the RSA marker beads during the COVID-19 pandemic, we halted recruitment for the DL group (which was contemporaneous to the DA group but proceeded more slowly). We completed an interim analysis of migration, comparing between the DL and DA groups, and found 95% power for collarless stems and 77% power for collared stems, which we deemed adequate given the unusual extenuating circumstances inhibiting further recruitment.
Ethics approval
This prospective cohort study was approved by our institutional research ethics board and registered with ClinicalTrials.gov (NCT03558217).
Results
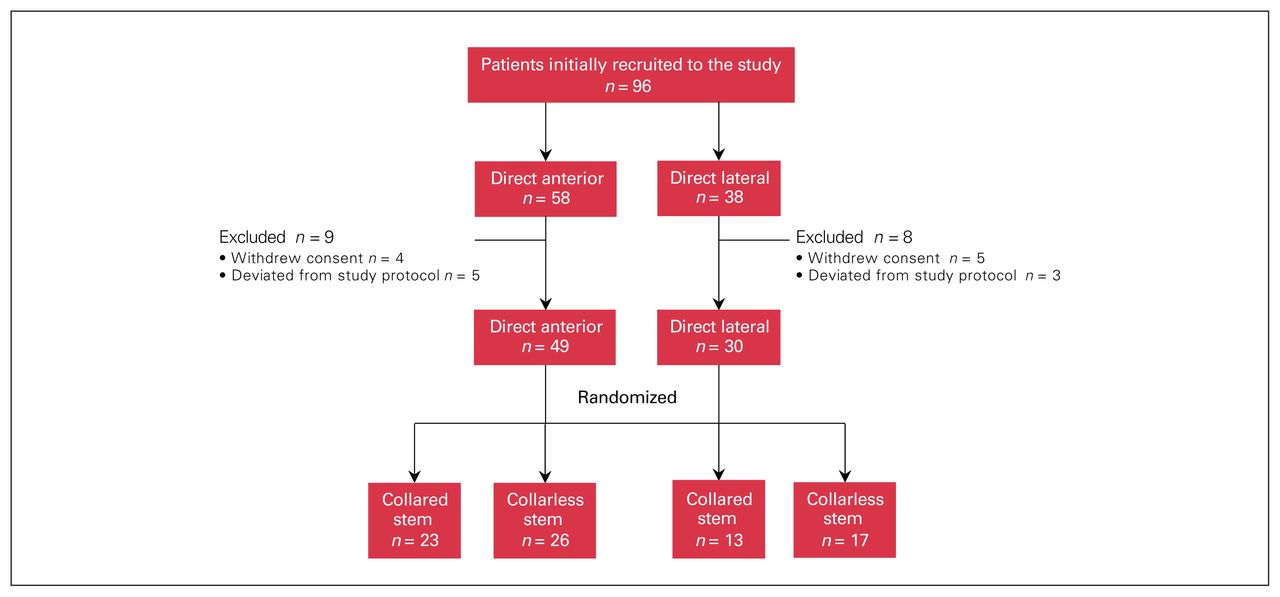
A total of 79 patients were recruited, including 30 who underwent the DL approach and 49 who underwent the DA approach (Figure 1). There were no differences in demographics (Table 1) or patient-reported outcomes (Table 2) between surgical groups. There was a difference in the femoral stem offset between groups, with patients in the DL group receiving fewer high-offset stems than patients in the DA group (p = 0.024). Radiographically, there were no differences in CFR (p = 0.740) or Dorr classification for bone quality (p = 0.545) between the DL and DA groups.

Flow diagram showing study group allocation.
Characteristics of direct anterior and direct lateral groups
Questionnaire results of direct anterior and direct lateral groups
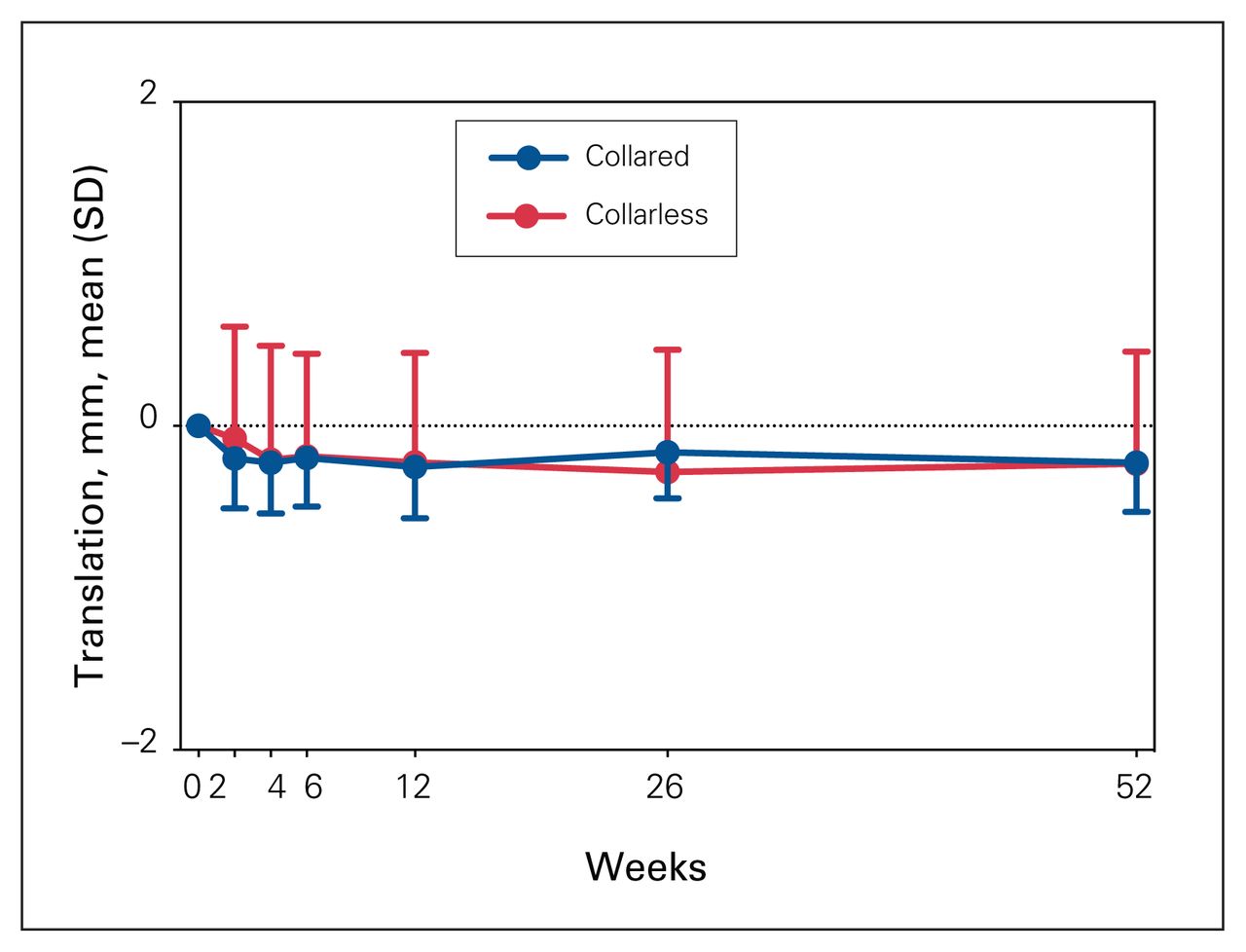
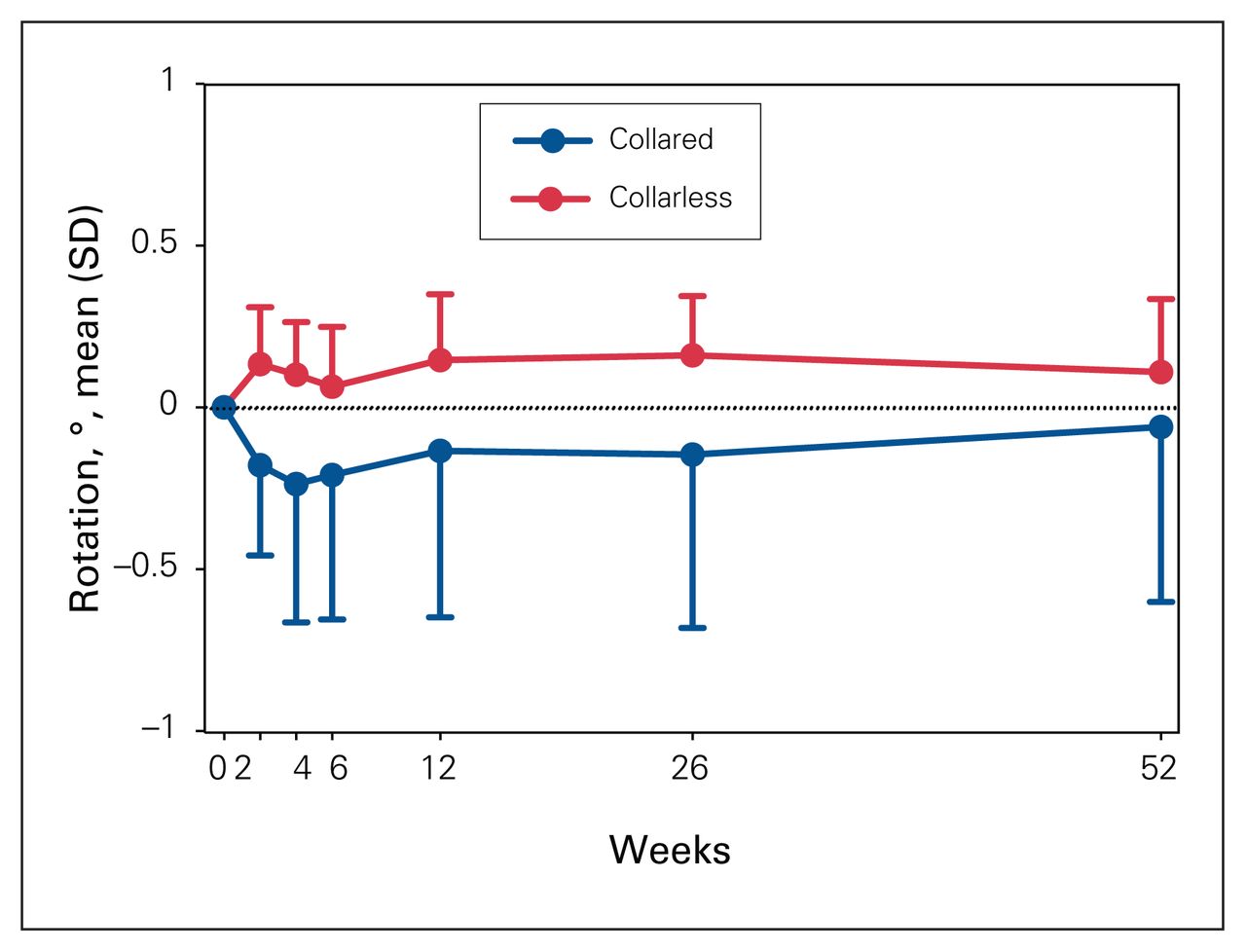
Within the DL group, 13 patients received a collared stem and 17 patients received a collarless stem. There was no difference in migration along the y-axis between stem designs (Table 3 and Figure 2, p = 0.894). The only significant difference of implant movement between stem designs in the DL group was the varus–valgus rotation about the z-axis (p = 0.044), where collared stems rotated more toward varus tilt and collarless stems rotated more into valgus (Figure 3).
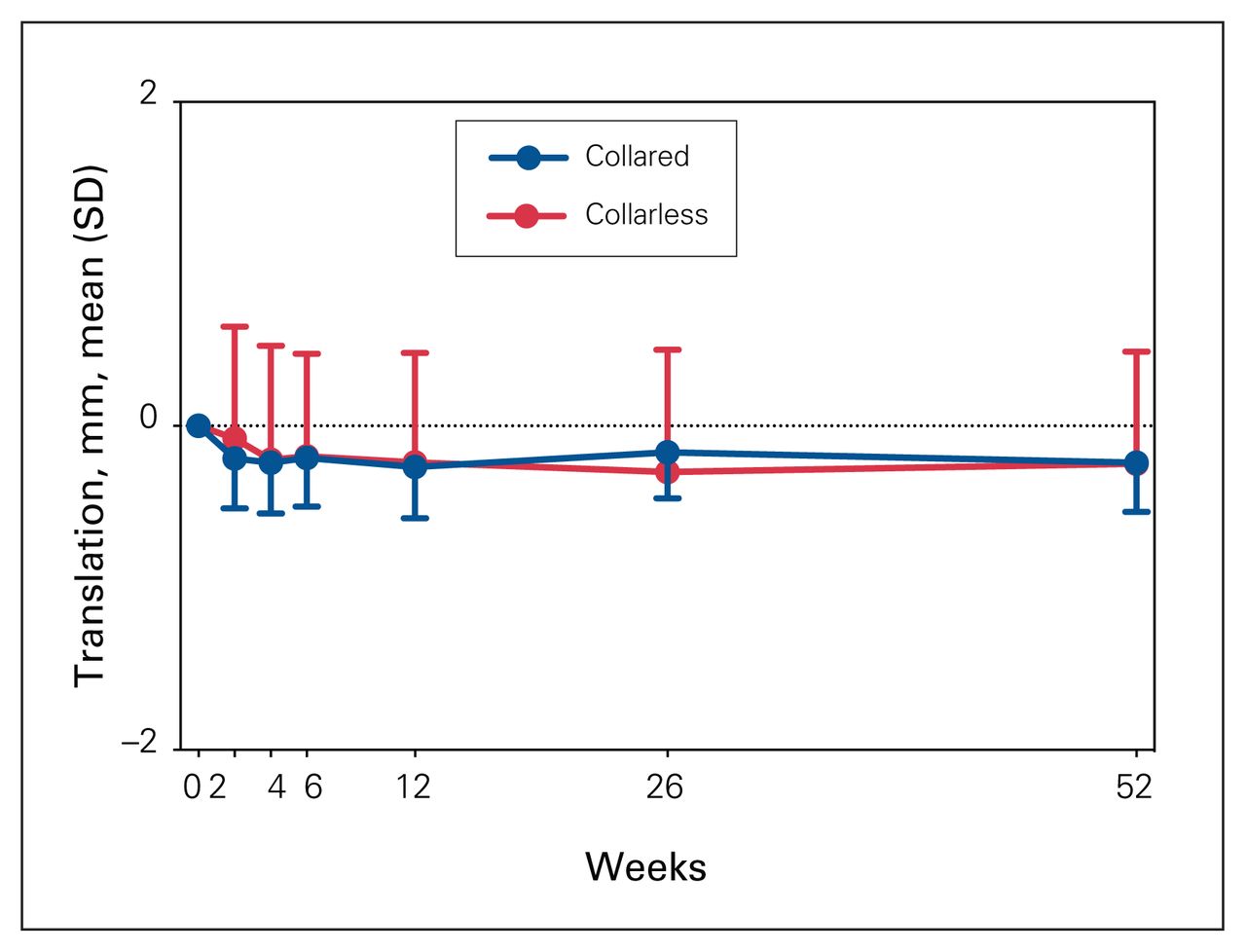
Migration (y-axis translation) between collared and collarless stems in the direct lateral group (p = 0.894), from day of surgery until 1 year after surgery. SD = standard deviation.

Varus–valgus rotation (z-axis rotation) between collared and collarless stems in the direct lateral group (p = 0.043), from day of surgery until 1 year after surgery. SD = standard deviation.
Translations and rotations of femoral stems of the direct lateral group, from the day of surgery to 1 year after surgery
Comparing the DL group to the previously reported DA group, surgical approach did have a significant effect on migration for both collared (Table 4, p = 0.031) and collarless stem designs (Table 5, p = 0.002). From the day of surgery to the 2-week follow-up examination, collared stems within the DL group migrated significantly less than collared stems in the DA group (Figure 4A, mean difference 0.786 mm, p = 0.020). Similarly, in the first 2 weeks after surgery, collarless stems in the DL group migrated less than collarless stems in the DA group (Figure 4B, mean difference 3.136 mm, p = 0.001). After the 2-week visit, there were no differences in migration between the DL and DA groups, and stem designs in both surgical groups remained stable through to 1 year after surgery. Furthermore, there was also a difference in internal rotation about the y-axis between surgical groups for both collared (p = 0.004) and collarless stems and (p = 0.040), with the DA group rotating into greater retroversion than the DL group (Figure 5).

Migration (y-axis translation) between direct anterior (DA) and direct lateral (DL) surgical groups for patients who received (A) collared stems (p = 0.031) or (B) collarless stems (p = 0.002), from day of surgery until 1 year after surgery.
SD = standard deviation.

Version (y-axis rotation) between direct anterior (DA) and direct lateral (DL) surgical groups for patients who received (A) collared stems (p = 0.004) (B) collarless stems (p = 0.040), from day of surgery until 1 year after surgery.
SD = standard deviation.
Translations and rotations of collared femoral stems by surgical approach, from the day of surgery to 1 year after surgery
Translations and rotations of collarless femoral stems by surgical approach, from the day of surgery to 1 year after surgery
We did not observe any correlation between migration and patient functional ability (defined as total TUG test time) or between migration and patient activity (defined as average daily step count) for the DL and DA groups at any time point, regardless of collared or collarless stem design (Table 6; p > 0.05 for all correlations).
Correlation of femoral stem subsidence (y-axis translation) to patient function and patient activity by surgical approach at each time point*
Discussion
As one of the most common interventions for musculoskeletal disorders, there is continuous demand to further improve patient outcomes, minimize patient recovery times and lower health care costs after THA. With the growing popularity of minimally invasive surgeries, surgical approach has become a topic of debate. A network meta-analysis from Putananon and colleagues29 investigated the DA, DL, direct posterior and direct posterior-2 approaches and compared their postoperative outcomes and complications. In terms of complications such as dislocation, infection and fracture, the DL approach followed the posterior approach for fewest complications, and the DA approach had the most complications of the 4 approaches. Further, Petis and colleagues21 conducted a literature review and reported on various large studies that followed patients who underwent THA with different surgical approaches. This showed low dislocation rates associated with both the DA and DL approach and a higher dislocation rate associated with the posterior approach.21 Eto and colleagues12 concluded that the DA approach has higher rates of aseptic loosening and, consequently, a higher early revision rate than the DL and posterior approaches. Sheth and colleagues30 reported no increased risk in early revisions for loosening between surgical groups. We investigated the stability of 2 stem designs implanted with the DL approach and further examined how surgical approach affected implant migration. We also evaluated whether patient functional ability and activity level influenced implant migration after THA.
We found that stem design did not affect migration for patients who underwent the DL approach, as both designs were remained stable through to 1 year after surgery. The same was not noted for the DA approach, as we previously reported that stem design did have a significant effect on migration, particularly in the first 2 weeks after surgery.18 Further, collared stems rotated more toward varus and the collarless stems rotated toward valgus (p = 0.043) in the DL group; however, the amount of rotation was less than 1°. This small amount of motion is not clinically important as varus or valgus malalignment is defined as 5° or more.31
The internervous and intermuscular nature of the DA approach has been reported to result in less postoperative pain and a quicker recovery; however, there are concerns about possible increased rates of intraoperative complications, given challenges with femoral exposure.32,33 A study by Rivera and colleagues10 tested the hypothesis that surgeons’ knowledge of increased risk of complication may interfere with appropriate stem sizing and concluded that the possibility of using an undersized stem is 3 times more likely with the DA approach. Stem undersizing is a documented risk factor for aseptic loosening as it affects primary stability and results in greater micromotion and implant migration.34 When comparing surgical approach groups, we found that the DA group had greater implant migration for both collared and collarless stems than the DL group, though radiographic analysis did not differ in the stem canal fill measured between groups. Most implant migration occurred between the day of surgery and the 2-week follow-up examination for both groups, with the collared stem design significantly reducing the migration in the first 2 weeks within the DA group. Implant migration stabilized from 2 weeks through to 1 year after surgery, suggesting adequate stem fixation and a low risk for aseptic loosening. We did not observe continuous stem migration with either surgical approach or stem design, which would have indicated a risk of early loosening.14,16 This is in keeping with a retrospective review of the Corail stem at this institution, which found no difference in the overall revision rate between approaches but a greater absolute number of revisions owing to aseptic loosening for the DA approach.35
In addition to differences in migration between surgical groups, there was also a rotational difference across the y-axis, which, like migration, mostly occurred from the day of surgery to 2 weeks postoperation. Both collared and collarless stem designs in the DA group rotated significantly more toward retroversion than stems in the DL group (p = 0.004 and p = 0.040, respectively); however, the average at all time points was less than 5°.
As a secondary objective, we investigated the possibility that an early recovery may be a factor that increases the magnitude of migration. The DA approach is associated with an earlier recovery and we observed that femoral stems in the DA group had greater migration early on than the DL group.1,21 However, our results showed there was no correlation between migration and patient functional ability or activity level in all groups at all time points through to 1 year after surgery. This suggests that patients who had greater functional ability and higher activity levels soon after surgery did not have more implant migration than patients who took longer to recover, regardless of surgical approach.
Limitations
We were unable to reach target recruitment for the DL group; however, the interim analysis showed we had sufficient power to compare migration between surgical groups. There is also potential bias introduced since surgical approach was not randomized; however, the expertise-based trial design in orthopedics has been reported to reduce challenges related to differential expertise bias and clinical equipoise.19,20 Further, with the steep learning curve associated with the DA approach and substantial differences in surgical technique, the expertise-based design ensured the best technique was used in all cases.21 Another limitation is that the DA surgeon had access to intraoperative images, as these are commonly used for the DA technique; but despite this, the DA group had greater migration. In addition, baseline RSA exams were conducted before each patient left the hospital, but not necessarily before they were bearing weight, so some initial migration may have been missed. It is possible that asking patients to wear their activity tracker at least a week before each appointment may have influenced an increase in their activity, but despite this potential increase, we saw no impact on implant migration.
Conclusion
In this study, we investigated the impact of implant design and surgical approach on implant stability, including the potential effect of enhanced patient recovery. Early functional ability and higher activity levels did not influence the magnitude of migration. Migration did not differ between collared and collarless stem designs in the DL group, but the collared stem design significantly reduced the migration in the DA group. Although the DA group had significantly more migration than the DL group for both stem designs in the first 2 weeks after surgery, both groups had continued stability thereafter, suggesting a low risk of aseptic loosening for both groups. Adequate stem fixation is achievable with either surgical approach, and the collared stem design can provide greater initial stability for patients undergoing THA using the DA approach.
Footnotes
Previously presented at the 2019 meeting of the International Society for Technology in Arthroplasty; the 2019, 2020 and 2021 meetings of the Canadian Orthopaedic Association; the 2019 and 2021 meetings of the International Radiostereometry Society; and the 2021 London Health Research Day.
Competing interests: Edward Vasarhelyi reports grants from DePuy and Microport, consulting fees from DePuy and Zimmer Biomet and participation on an advisory board with Hip Innovation Technology. He also reports institutional and research support from DePuy, Smith and Nephew, Stryker and Zimmer Biomet. Matthew Teeter reports membership with the Canadian Orthopaedic Research Society, the Canadian Radiostereometric Analysis Network and the International Society for Technology in Arthroplasty. Brent Lanting reports grants and consulting fees from DePuy, Smith and Nephew, and Stryker. No other competing interests were declared.
Contributors: Edward Vasarhelyi, Matthew Teeter and Brent Lanting conceived and designed the study. Maxwell Perelgut and Jennifer Polus acquired, analyzed, and interpreted the data. Jennifer Polus drafted the manuscript. All authors revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: This study was funded by The Arthritis Society and by DePuy Synthes. Jennifer Polus is supported by a graduate scholarship from the Canadian Institutes of Health Research.
- Accepted October 4, 2021.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.