


Abstract
Breakage of the femoral component of a total hip replacement prosthesis is an uncommon occurrence with modern prostheses. The authors report what appears to be the only case of bilateral prosthetic fracture. A 65-year-old man, who was physically active, suffered bilateral femoral stem fractures 3 and 5 years after total hip replacement. The bilateral cemented hip replacements remained asymptomatic until catastrophic failure of the femoral component occurred. Both the prostheses were titanium (Biomet; Warsaw, Ind.) with chrome cobalt modular femoral heads. The authors stress the importance of maintaining an adequate cement mantle in Gruen zones 1 and 7 because failure to do so may result in micromotion and subsequent stem fracture.
Breakage of the femoral component of modern total hip prostheses is rare. We report the case of a 65-year-old man who underwent staged bilateral cemented total hip replacement with titanium prostheses (Biomet; Warsaw, Ind.). Three years later the prosthesis on the right failed and was revised. Then, 2 years after that, the contralateral prosthesis also failed.
Case report
A physically fit 65-year-old man underwent bilateral total hip replacement (Fig. 1) in 1991. He weighed more than 90 kg, a factor that may have contributed to the stem breakage. 1,2 After informed consent was obtained, he was randomized to have cemented total hip replacements as part of an ongoing study comparing cemented and cementless total hip replacement. Prosthesis size was chosen to provide a cement mantle3 of at least 2 mm over the entire prosthesis after standard preparation of the proximal femur (Fig. 2).

Radiograph of the hips of the 65-year-old man before hip replacement.

Postoperative radiograph of a right total hip joint replacement.
Follow-up x-ray films revealed progressive loosening of the acetabular components bilaterally (Fig. 3), but he remained asymptomatic and continued to participate in physical activities, which included golf.

Progressive loosening of the acetabular components after hip replacement.
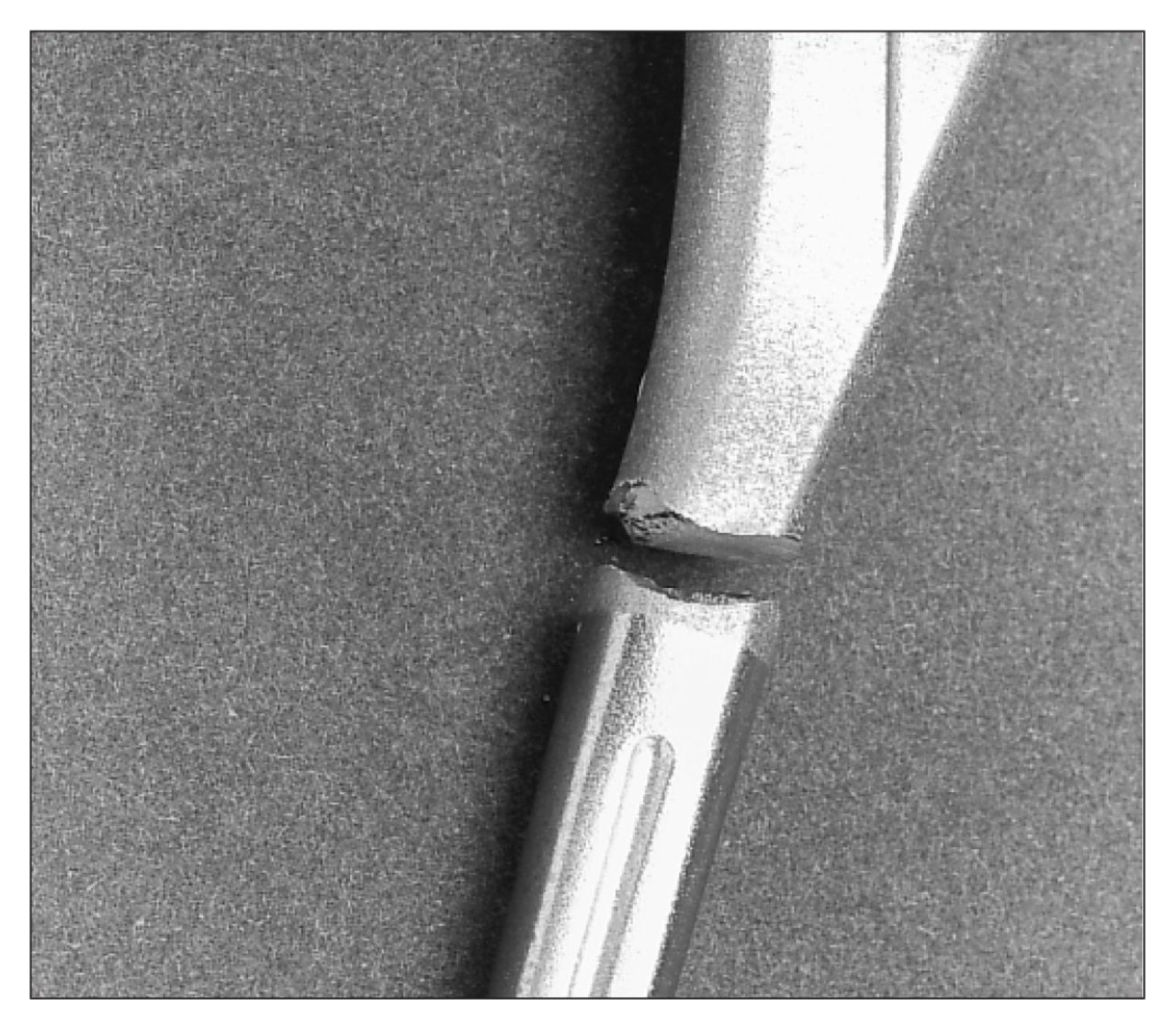
Close inspection of the radiographs demonstrated a lucent line developing between the prosthesis and the cement bilaterally in Gruen4 zones 1 and 7 (Fig. 4). Eventually the prosthesis fractured in its mid-portion, at the lower end of this lucency (Fig. 5). The prosthesis on the left failed in 1994 and that on the right in 1996. Inspection of the latter prosthesis showed that this breakage occurred close to but not directly at the junction of the surface texture change (Fig. 6). The original prosthetic fracture was in a similar position. Burnishing was evident both proximal and distal to the stem fracture (Fig. 7). The burnishing was evident mainly on the medial and posterior surfaces. The extent of the burnishing provided direct evidence of movement of the prosthesis in the cement mantle along much of the stem length. At the time of revision the distal portion of the prosthesis was well fixed in the cement mantle.

The development of a lucent line in Gruen zones 1 and 7 (arrows).

The fractured stem of the left prosthesis.

The fractured prosthetic stem.

The fractured prosthetic stem with apparent burnishing.
Discussion
The Young’s modulus of titanium and the relatively small cross-section of the prosthesis predispose this implant to deformation when loaded. Cantilever bending5 presumably produced flow of the cement in the proximal femur, particularly in zones 1 and 7. The cancellous bone supporting this cement may not have been supportive enough to prevent this cold flow of the cement. There was no evidence of failure of the cement mantle before fracture of the prosthesis, but such failure cannot be ruled out by our x-ray films.
Preparation of the femoral shaft for cemented total hip replacement commonly involves taper pin reamers and rasps. The reamers open up the proximal diaphysis, usually until the dense transition from cancellous to cortical bone is reached. The rasps prepare the cancellous metaphysis, generally providing a bed for the prosthesis and a predetermined cement mantle. In patients with excellent bone this proximal cancellous bed can support the proximal prosthesis and cement. However, the fractured trabeculae in the proximal femur may either be porotic or heal unpredictably, leading to poor support of the implant proximally.6 If excessive trabecular bone is left in zone 7, it might not allow a 2-mm mantle to be properly fixed to the transitional trabeculae. If this were to occur, micromovement would be possible and failure in the form of fracture of the stem might occur, particularly if the implant was well fixed distally. If movement is allowed to persist, eventually osteolysis will occur, further compounding the micromotion. Eventually osteolysis can undermine a previously well-fixed implant.
Prosthesis fracture at the point where the distal stem was well fixed and the proximal stem unsupported was common with the early Charnley prostheses.7 Prosthesis modification and the introduction of Orthron 90 (DePuy, Warsaw, Ind.) have eliminated this mode of failure for the Charnley prosthesis.
In our case the implant used was titanium. From an early stage a radiolucent line was seen between the prosthesis and the cement in zones 1 and 7. This gap on supine x-ray films may have been due to bending of the prosthesis, flow in the cement or tapping of wear debris pumped into the gap during cyclical loading (Fig. 8). Cyclical bending of the prosthesis obviously occurred, as evidenced by the burnishing of the prosthesis on either side of the ultimate prosthetic fracture. Cyclical bending of a distally fixed prosthesis, resulted in fatigue failure as the degree of deflection was above the fatigue threshold. Given that the prosthesis in question was a relatively small cross-section, along with the lower Young’s modulus of titanium, the degree of bending expected would be greater than that of a bulkier prosthesis made from a stainless steel alloy.

Radiograph showing wear debris.
The advantage of titanium in joint replacement lies in its ability to osseointegrate. Titanium is no longer recommended for the bearing surface in joint replacements, and its role in cemented joint replacement may also be in question. Although a cemented titanium femoral stem is no longer recommended, it is important to point out the importance of maintaining an adequate cement mantle in Gruen zones 1 and 7 as failure to do so may result in micromotion and subsequent stem fracture irrespective of the metal used.
- Accepted January 30, 1997.
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.