


Splenic tumours are relatively rare and difficult to diagnose before surgery. Splenic neoplasms include hemangioma, lymphagioma, hamartoma, hemangiosarcoma, malignant lymphoma and metastatic carcinoma. Inflammatory pseudotumours of the spleen are extremely rare and are frequently misdiagnosed as maglinant or benign tumours.
Case 1
A 60-year-old man visited our hospital complaining of left upper abdominal discomfort and weight loss of about 10 kg in the last 6 months. The patient had a long history of alcohol intake (about 40 years). Ultrasonography showed a low echoic mass in the spleen. An abdominal CT scan (Fig. 1) confirmed a low-density hypovascular mass located in the spleen and measuring 6.9 × 7.1 cm, and necrosis could be identified in the central area of the mass. Laboratory investigation revealed an elevated level of immunoglobulin G and β2-microglobulin.

CT scan of case 1 showed a low-density mass in the spleen in enhanced modes.
Case 2
A 77-year-old woman was admitted to our department with upper abdominal discomfort persisting for 3 weeks. The patient also had a weight loss of about 5 kg over almost 1 year. Although physical examination and laboratory investigation results were unremarkable, ultrasonography showed a low echoic mass in the spleen. An abdominal CT scan also demonstrated a 6-cm diameter, low-density hypovascular mass in the spleen, with necrosis in the central area of the mass. To rule out a possible malignant neoplasm, splenectomy was performed for these 2 patients. The removed spleen weighed 240 g and 180 g for the first and second patient, respectively. Intraoperative and postoperative courses were uneventful.
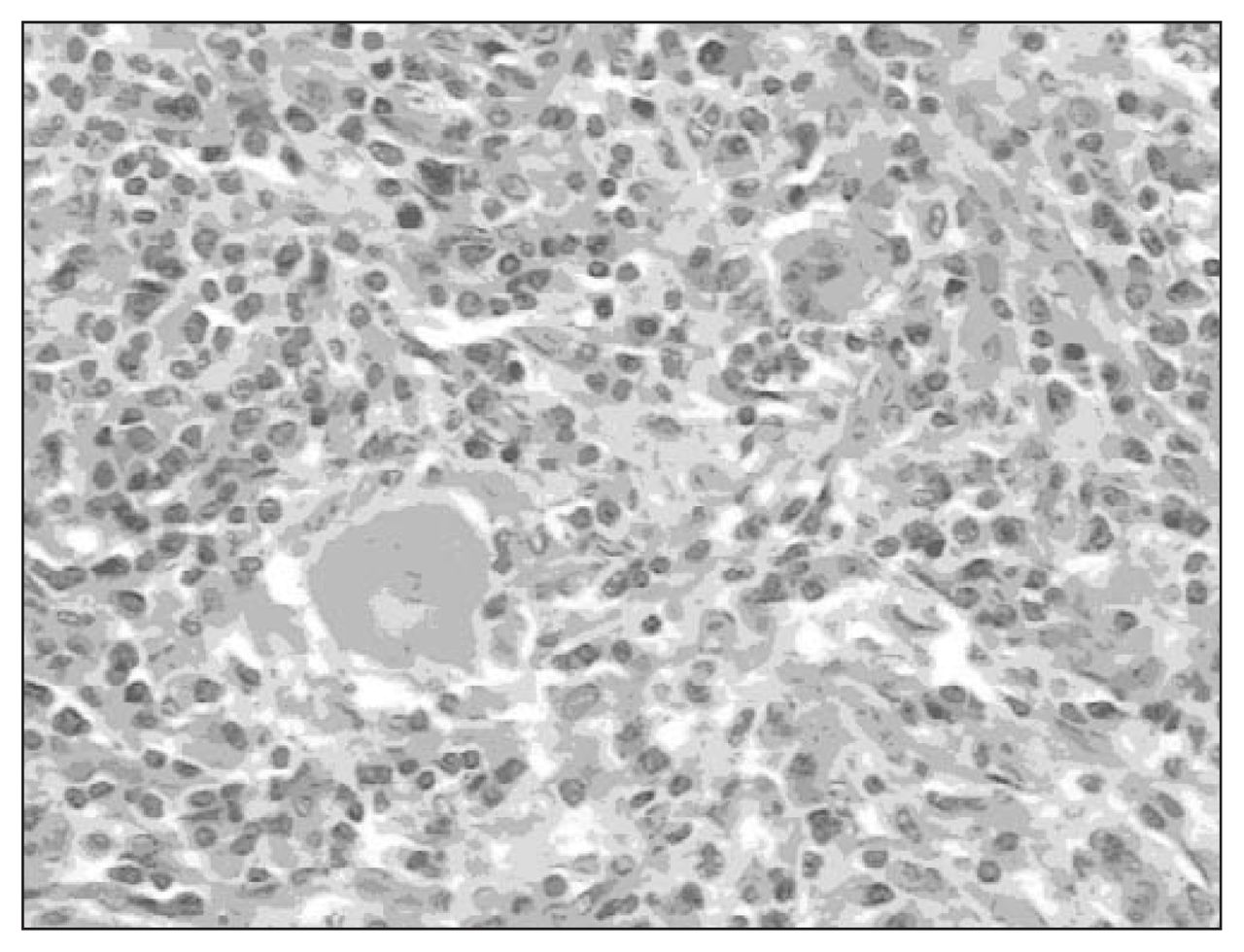
On gross pathological examination, both masses were roughly round and elastically firm. The cut surfaces of the masses were well circumscribed, tan-white and bulging. There were necrotic areas in the centre of the lesions. Histologically, the splenic architecture was effaced in the area of lesion. There was a large, irregularly shaped focus of necrosis in the centre, with a marked inflammatory infiltration composed of an admixture of inflammatory cellular elements, predominantly plasma cells and lymphocytes with hyalinization, fibrosis, lymph follicles and multinuclear giant cells (Fig. 2). Liver biopsy of the first patient showed hepatic schistosomiasis that occurred simultaneously. The patients are alive and asymptomatic 3 months and 10 months, respectively, after surgery.

The admixture of inflammatory cells, predominantly plasma cells and lymphocytes and multinuclear giant cells (hematoxylin and eosin stain, original magnification 200×).
Discussion
Inflammatory pseudotumours are known to occur in a wide variety of anatomic locations, including the orbit, respiratory tract, gastrointestinal tract, liver and others; however, inflammatory pseudotumours of the spleen are extremely rare lesions. When a lesion occurs as a primary splenic tumour, lymphoma is usually clinically suspected. Although imaging examinations have improved greatly in the past 2 decades, the true diagnosis is usually only revealed after the spleen is examined histologically.
To our knowledge, since the first 2 cases were reported by Cotelingam and Jaffe in 1984,1 fewer than 80 cases have been reported in the literature. According to these reports, most patients were of middle to advanced age, and there appeared to be no relation to sex. The clinical symptoms were most diverse, with upper abdominal pain or discomfort found frequently. Sometimes fever and splenomegaly were present, whereas other symptoms were not specific to the disease. The laboratory data of many cases showed no evidence of any abnormality. Note that inflammatory pseudotumour of the spleen may present with both clinical signs and symptoms suggestive of a malignant tendency. As in our reported cases, patients had a comparatively obvious recent weight loss. A fine-needle aspiration was performed in 3 previous cases. This percutaneous biopsy can be used in the preoperative workup of the mass in other organs, but it is not recommended for a mass in the spleen because of poor specificity, the risk of bleeding and the fear of spillage of tumour cells if the tumour is malignant.2
In earlier reported cases the diagnostic imaging of splenic inflammatory pseudotumour showed different patterns. Ultrasonography might reveal a partially calcified, well-defined echogenic mass or hypoechoic discrete lesion, as observed in our cases. CT usually demonstrated a low-density mass in both the nonenhanced and enhanced modes, consistent with the findings in our cases. MRI might show a well-defined mass better than CT scan, reportedly isointense on T1-weighted images and with either increased or decreased signal intensity on T2-weighted images, with respect to the surrounding normal spleen.2 An inflammatory pseudotumour is a benign, well-circumscribed mass, usually solitary, composed of foci of inflammatory cells, mainly plasma cells, and lymphocytes in a fibroblastic stroma.3 The cellular composition of inflammatory pseudotumour of the spleen can be remarkably heterogeneous. Inflammatory pseudotumours of the spleen showing some resemblance to granulation tissue and normal lymphocytes and plasma cells are constant features, although in variable mixtures and numbers. Neutrophilic and eosinophilic leukocytes are also sometimes present.
Although the etiopathogenesis of the disease is unclear, infection, vascular causes and autoimmune disorders have been proposed. The presence of granulomas and giant cells in the tissue suggests infection. However, no microorganism has been identified in tissue sections and cultures from specimens in any of the reports to date. Some cases have been reported to be Epstein-Barr virus–positive inflammatory pseudotumours.4 Vascular cause is another hypothesis, and it is believed by some that these lesions may be due to an intraparenchymatous hemorrhage secondary to trauma or coagulopathy. 5 Cotelingam and Jaffe1 suggest that the main initial event might have been a focal parenchymal necrosis with hemorrhage. The high number of plasma cells in this lesion suggests an immunological origin as another hypothesis. The prognosis of this condition has generally been considered favourable after splenectomy, according to the previously published cases. There have been no reports of metastatic disease, local invasion or recurrence after removal of the lesion. However, careful follow-up is necessary, because some patients with inflammatory pseudotumours of the liver are reported to have likely died as a result of the disease.5
To conclude, inflammatory pseudotumour of the spleen is a relatively uncommon pathology not associated with specific clinical findings; it masquerades as a splenic neoplasm. Currently, no imaging techniques allow preoperative diagnosis; only splenectomy and histopathologic study of the specimen allow diagnosis and treatment of this entity.
Footnotes
Competing interests: None declared.
- Accepted February 5, 2007.
In this issue

{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.