


A 27-year-old man, who had undergone hemorrhoidectomy 7 years previously, presented with intermittent rectal bleeding and anemia that had been present for 8 years. Digital rectal examination confirmed the rectal bleeding, but no mass was palpable in the rectal wall. The physical examination revealed no other abnormalities. Blood count showed mild anemia (hematocrit 27%, hemoglobin 79 g/L). Upper gastrointestinal endoscopy show no abnormalities, but colonoscopy revealed an edematous mucosa and diffuse submucosal bluish nodulation with dilated veins (Fig. 1), extending from the dentate line up for 20 cm. At laparotomy, the rectum and distal sigmoid colon had significant vascular engorgement on the serosal surface, extending through the mesorectum and mesosigmoid. The patient underwent low anterior resection with a stapled colorectal anastomosis. Diffuse cavernous hemangioma (DCH) was diagnosed.

Endoscopic view of the diffuse cavernous hemangioma of the rectum.
The macroscopic view of the rectosigmoid colon showed many abnormal hemangiomatous vessels (Fig. 2). Histopathological examination of the specimen showed DCH invading all layers of rectum and distal sigmoid colon (Fig. 3). The patient was free of any symptoms at 6-year follow-up.

Macroscopic view of the excised rectal cavernous hemangioma.
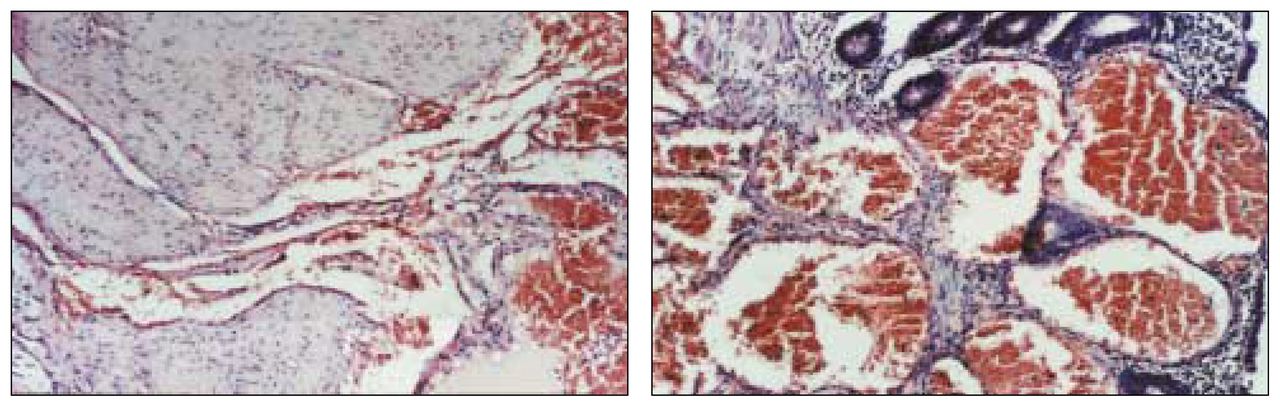
Microscopic findings of the cavernous hemangioma of the rectum show (a) extremely dilated vessels containing erythrocytes in all the layers of rectal wall and (b) the absence of cellular dysplasia in these vessels and the adjacent tissue, proving its hamartomatous nature (hematoxylin–eosin stain, original magnification ×350).
DCH of the rectosigmoid colon is an extremely rare malformation that is generally seen in young adults, with a male-to-female ratio of 2:1.1 Patients usually suffer painless rectal bleeding and anemia. However, there may be associated intestinal obstruction, diarrhea, constipation and hematuria.2 The presence of hemangioma in the cutaneous and mucous membranes, or Klippel–Trenaunay syndrome, should alert the clinician to the presence of rectal hemangioma.3,4 Endoscopy is the method of choice for diagnosis. Upper gastrointestinal endoscopy should be done in all patients to rule out any synchronous hemangiomas. Other diagnostic tools such as barium enema, selective angiography, computed tomography, magnetic resonance imaging or endoscopic ultrasonography may show extramural spread of the lesion and exclude other causes of rectal bleeding. The definitive treatment for DCH is excision of the involved bowel. Sphincter-saving procedures, avoiding damage to perirectal neural structures, is preferred for satisfactory long-term results.5 The vascular malformations that remain in the proximal anal canal, usually 1 to 2 cm above the dentate line, can be managed conservatively by argon or Nd:YAG laser therapy, or sclerotherapy in the case of rebleeding.
Footnotes
Submissions to Surgical Images, soft-tissue section, should be sent to the section editors: Dr. David P. Girvan, Victoria Hospital Corporation, PO Box 5375, Station B, London ON N6A 5A5 or Dr. Nis Schmidt, Department of Surgery, St. Paul’s Hospital, 1081 Burrard St., Vancouver BC V6Z 1Y6.
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.