


Abstract
Delayed rupture of the spleen is a rare but serious complication of blunt abdominal trauma. A 47-year-old woman with a history of fractured pelvis from a motor vehicle accident 6 months earlier presented with evidence of a myocardial infarction. Subsequent streptokinase administration was complicated by splenic rupture, which was managed by evacuation of the clotted blood and splenectomy. The patient made a complete recovery. The risk of splenic rupture and bleeding complications resulting from thrombolytic therapy for myocardial infarction is discussed, as are the controversy over whether delayed splenic rupture is a true diagnosis, the mechanism of rupture and the clues to impending rupture.
Although splenic injury is common after blunt abdominal trauma,1 delayed splenic rupture (DSR), occurring 48 hours or more after the injury is rare.2,3 DSR is three times more common in men than women. Rupture occurs in the first 2 weeks after injury in 75% of cases,4 although in some cases rupture is reported from 1 month to 11 years after injury.5,6 The death rate is approximately 10%.7 Before the use of diagnostic peritoneal lavage (DPL), the reported incidence of DSR among patients with blunt abdominal trauma was approximately 15%, but with the use of DPL and computed tomography (CT), its reported frequency has fallen to 1% to 2%.3,8 Thus, whether the condition represents delayed recognition of splenic rupture rather than true DSR is still debated.3,7–9
Thrombolytic therapy for patients with myocardial infarction became common practice in the late 1980s. It has significantly reduced the death rate from acute myocardial infarction when administered within the first 4 to 6 hours after the onset of symptoms. Such therapy, however, may activate bleeding from a number of sites, including organs that have been recently traumatized.
Case report
A 47-year-old woman presented with retrosternal chest pain associated with diaphoresis, nausea and dyspnea. She had a 1-week history of chest pain on exertion but was otherwise well. Six months earlier she had suffered a fractured pelvis and right wrist in a motor vehicle accident. At that time there was no clinical evidence of splenic rupture, and neither DPL nor CT was done.
On admission, she had ST-segment elevation in leads V1 to V3, cardiac enzyme levels indicative of an acute myocardial infarction and a blood hemoglobin level of 143 g/L. A standard dose of streptokinase therapy was started, followed by intravenous heparin (a bolus of 5000 U and infusion at a rate of 1000 U/h). No contraindications to streptokinase therapy were present according to current guidelines (Table I). A brief episode of hypotension followed but responded to fluid infusion. Her hemoglobin level 2 hours after the initiation of therapy was 76 g/L. Nine hours after admission, she complained of neck pain and nausea, and her systolic blood pressure dropped to 50 mm Hg. Heparin was stopped, and she was treated with intravenous fluids, dobutamine and dopamine. Her systolic pressure, however, remained below 80 mm Hg for more than 3 hours. Her abdomen gradually became distended and her hemoglobin level continued to fall. She was thought to have a retroperitoneal hematoma and was given 13 units of packed red blood cells, 6 units of fresh frozen plasma and 10 units of cryoprecipitate. That evening, she suffered respiratory distress requiring intubation and assisted ventilation. The chest radiograph was suggestive of adult respiratory distress syndrome. Her oxygen requirement gradually increased, the serum creatinine and creatine phosphokinase levels rose and urine output fell. She was subsequently transferred to a tertiary care centre.
Contraindications to Streptokinase Administration (The Wellesley Hospital Protocol, Department of Pharmacy, 1994)
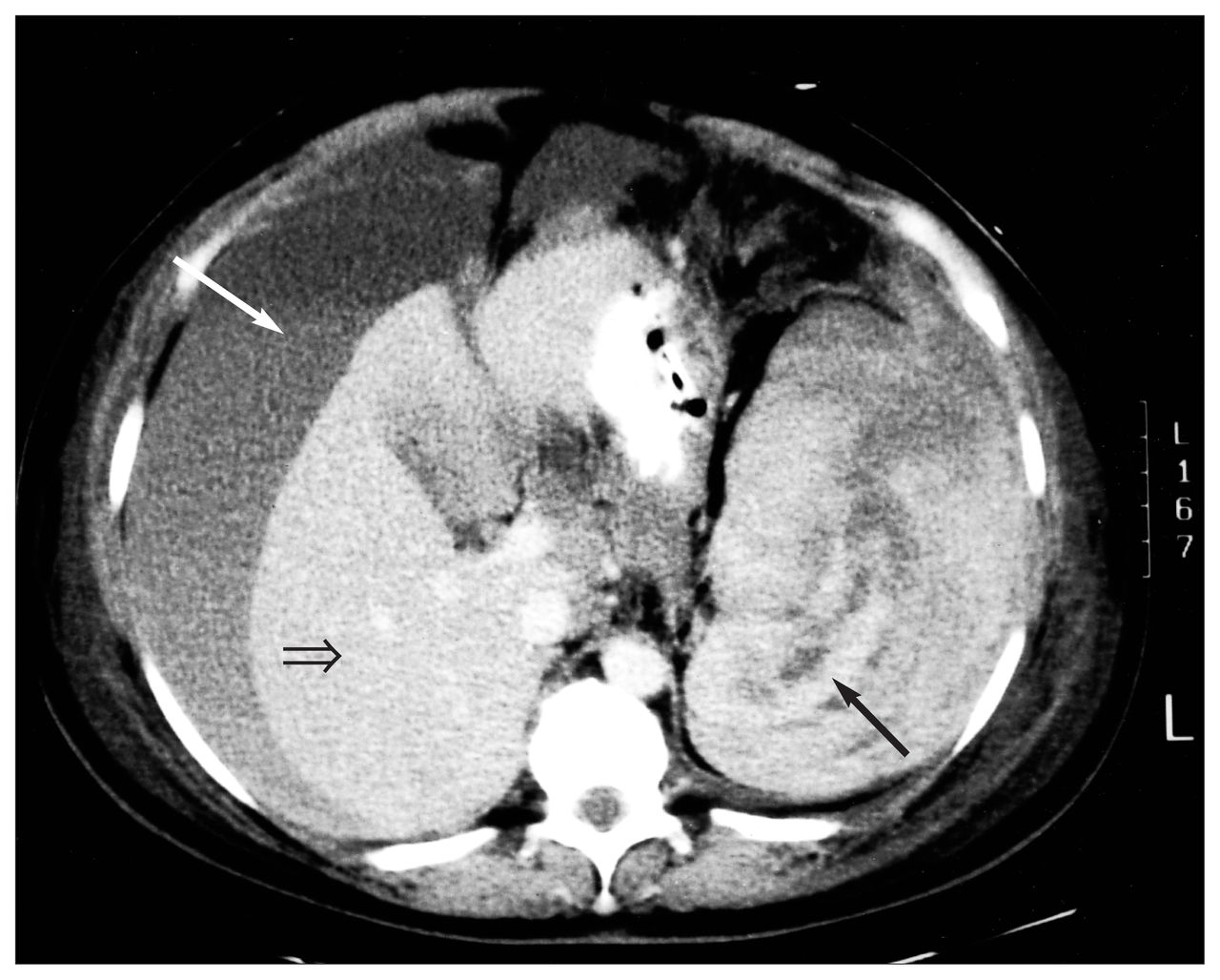
On admission she was hemodynamically stable on dobutamine, with a hemoglobin level of 80 g/L and a normal coagulation profile. However, her abdomen was distended and firm, her lower limbs were grossly edematous and she required ventilation and dialysis. Abdominal CT showed intraperitoneal blood with a fluid–fluid level (suggestive of settled blood components) and a ruptured spleen (Fig. 1).

Computed tomography scan (coronal slice) with intravenous contrast enhancement shows large amount of intraperitoneal fluid (white arrow), suggestive of settled blood components or active bleeding with extravasation of contrast. Liver (open arrow) is displaced by this fluid. There is multi-layered hematoma surrounding enlarged spleen (black arrow) suggestive of splenic rupture.
At operation, a large amount of clotted blood was evacuated from the abdomen, but there were no sites of active bleeding. The anterior splenic capsule was ruptured, so splenectomy was performed. Blood pressure was stable and urine output resumed during the operation.
Her oxygen requirements improved immediately after operation. The serum creatinine and urine outputs had returned to normal by the 10th day, and she subsequently made a complete recovery.
Discussion
Thrombolytic therapy is an accepted treatment option in the management of acute myocardial infarction.10 The risk of severe or life-threatening bleeding from combined streptokinase and intravenous heparin therapy is 0.5%.11 However, splenic hemorrhage has not been documented as a complication in large clinical trials,11,12 rather, intracranial, gastrointestinal, retroperitoneal and pulmonary sites of bleeding have been described.12
Only three cases of spontaneous splenic rupture after streptokinase therapy have been reported.13–15 Two of the reports described the use of streptokinase to treat myocardial infarctions,13,14 whereas the third was for deep venous thrombosis.15 Both patients with myocardial infarctions were previously healthy and neither had any history of trauma. In one patient, Gardner-Medwin and associates14 reported that pathological examination of the spleen revealed a single tear on the posterior surface, an area not usually associated with trauma. No adequate explanations were given for the splenic rupture in these cases.
It is unlikely, however, that spontaneous rupture occurred in our patient. It is difficult to accept that the spleen can rupture spontaneously from thrombolytic therapy alone. More likely some minor forgotten trauma predisposed the patient to splenic rupture. Lesser trauma, such as a fall or fight, often forgotten by the patient, has been implicated as a common cause of delayed rupture.9 Our patient had a history of major abdominal trauma 6 months before streptokinase therapy. It would be reasonable to attribute her complications to a streptokinase-induced DSR.
The controversy of whether DSR is a true diagnosis or merely delayed recognition of the rupture has been fuelled by the marked drop in its occurrence, likely from improved diagnostic skills. DPL immediately after abdominal trauma has reduced the incidence of DSR from approximately 15% to 1%.3,8 Abdominal CT has also reduced the incidence of delayed rupture, with reported sensitivities and specificities for acute splenic injury exceeding 96%.16 As a result, some authors have expanded their definitions of DSR to include investigative and clinical considerations. Schlater and Oshita17 defined DSR as rupture that occurs more than 48 hours after injury and when initial splenic imaging is negative. On the other hand, Berlatzky and associates7 suggested that DSR should be restricted to cases in which there is an asymptomatic interval between initial trauma and secondary hemorrhage.
Although most DSRs occur within 2 weeks of injury,4 there have been reports of intervals ranging from 1 to 11 years, with long asymptomatic periods between the time of injury and secondary splenic hemorrhage.5,6 This is consistent with the predominant theories outlining the mechanism of DSR. One theory proposes that the splenic capsule is able to contain the initial parenchymal hemorrhage within a cystic architecture only to rupture sometime later.1,9,17–20 Subcapsular hematomas would account for the initial unremarkable results of DPL, and if the lesion is small enough, CT scans would be negative at the time of initial injury. In contrast, another theory suggests that the splenic capsule is directly compromised from the onset of primary injury with the subsequent hemorrhage being contained by adjacent structures such as omentum.1,9,18,21,22 Although functionally controlled, the plug would be dependent on intra-abdominal stability because of the weak fibrinous union formed between the two viscera.1
Clues to impending DSR are nonspecific. Patients usually complain of diffuse abdominal pain1 or fullness and of discomfort in the left upper quadrant although they may have minimal or no symptoms.6 Taylor and Rosenfield20 found that CT scans, despite their accuracy, could not identify all intrasplenic lacerations at the time of initial injury. Also, Gruenberg and Horan23 reported a case of DSR 25 days after trauma in which initial investigations of DPL and visceral angiography all gave negative results. Although our patient did not undergo CT or DPL at the time of abdominal trauma, there were no signs or symptoms of splenic injury. Thus, it would be easy to miss DSR. Also, because the incidence of a bleeding event after streptokinase treatment has been reported12 to be approximately 30% within the first 96 hours, hypotensive episodes are not infrequent. These are usually treated conservatively with fluids or blood transfusions as needed. Hence, as occurred in our patient, unless specific clinical indications of a splenic rupture arise, streptokinase-induced hemorrhage is unlikely to be suspected.
Splenic hemorrhage is a potential abdominal catastrophe. Signs of hypovolemia accompanied by abdominal distension and tenderness, and hypoactive bowel sounds may be present. Left upper quadrant pain and tenderness, Kehr’s sign (left shoulder pain due to irritation of the left hemidiaphragm) and Ballance’s sign (dullness around the splenic area signifying hematoma formation combined with shifting dullness in the right flank from free blood), however, are felt to be more specific of a splenic injury.1,4,8,9 Although a mild leukocytosis and low hemoglobin and hematocrit levels are consistent with splenic hemorrhage, they are nonspecific and can be misleading. 4,9 Definitive diagnosis can usually be made by DPL and CT (Fig. 1).
In view of the wide range of latent periods reported for DSR (48 hours to 11 years), it is possible that our patient had sustained splenic trauma that remained clinically silent. It is unlikely that her cardiac ischemia was due to DSR before presentation since her hemoglobin level was normal, and significant blood loss would be necessary to prompt cardiac dysfunction in an otherwise healthy person. This degree of splenic hemorrhage would inevitably be associated with abdominal signs and symptoms, which were absent initially. The administration of streptokinase, however, would undoubtedly precipitate a splenic hemorrhage. To our knowledge, there have been no reports in the literature of DSR after streptokinase therapy.
Although early thrombolytic therapy is an accepted treatment for myocardial infarction, an active inquiry into any history of blunt abdominal trauma is reasonable. The danger of DSR is that it can be clinically silent. Initial investigations at the time of abdominal trauma may be negative, and therefore DSR may not be considered in a patient with subsequent intraabdominal bleeding. The effects of thrombolytic agents should be closely followed when DSR is possible. Prompt recognition of abdominal bleeding from DSR could prevent unnecessary morbidity and mortality.
- Accepted April 5, 1995.
References
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.